Morphometric Analysis of the Maxillary Sinus and Its Implications for Sinus Augmentation Surgery in an Eastern Indian Population
Sanjukta Sahoo, Tara P Tripathy, KC Pradheep Kumar, Siva Priya, Arthi Ganapathy, Praveen K Ravi

TL;DR
This study analyzes the structure of the maxillary sinus in an Eastern Indian population to improve dental implant surgery outcomes.
Contribution
The study provides population-specific morphometric data for the Eastern Indian population to guide sinus augmentation surgery.
Findings
Over half of the patients had insufficient residual bone height for dental implants without surgery.
Lateral wall thickness influenced the choice of surgical approach.
Left-side residual bone height was significantly lower than the right side.
Abstract
Introduction Sinus augmentation surgery, also called sinus graft or lift, involves elevating the Schneiderian membrane in the posterior maxilla to enhance alveolar bone height by placing a bone graft or osteogenic materials. This procedure is commonly performed to support dental implants. This study evaluates the morphometry of the maxillary sinus across different age groups within the Eastern Indian population and its implications for sinus augmentation surgery. Methods We analysed 85 patients (55 males (64.7%) and 30 females (35.3%)) who underwent computed tomography scans, assessing key parameters such as residual bone height, lateral wall thickness, medial wall thickness, and the sinus angle. Data were summarised and presented as mean ± SD for continuous variables and frequencies for categorical data. Inferential tests were used to analyse the parameters, with a significance…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
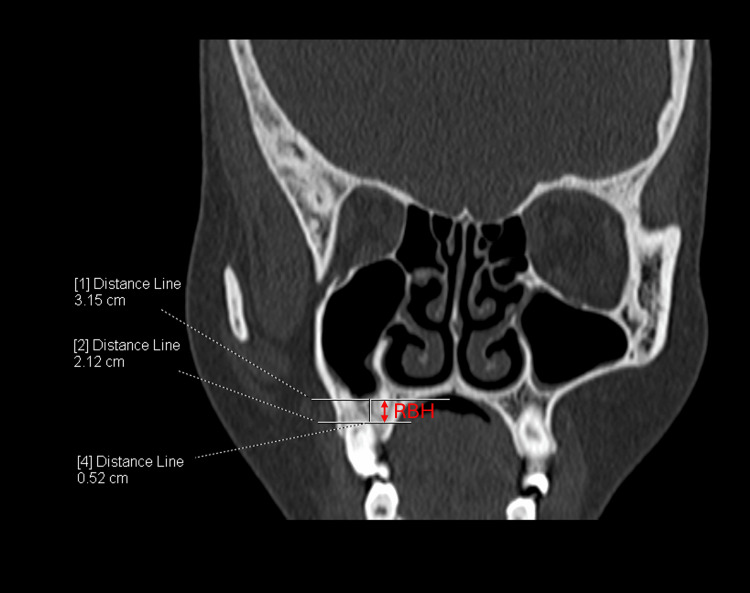 Figure 1
Figure 1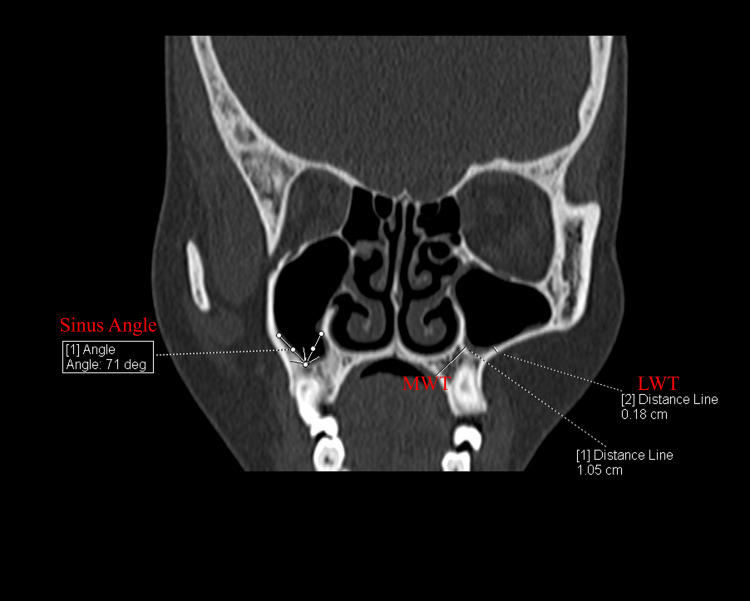 Figure 2
Figure 2| Parameter | Landmark | Method used | Significance |
| Sub-sinus residual bone height (RBH) (mm) | The distance from the alveolar ridge crest to the floor of the maxillary sinus | Measurements were taken from the highest point of the alveolar ridge to the lowest point of the sinus floor at the designated implant site. | This measurement assessed the vertical bone available for dental implant placement |
| Thickness of the lateral walls (LWT) (mm) | The lateral wall of the maxillary sinus. | The thickness of the lateral wall was measured from the outer cortical bone to the sinus membrane. | This measurement indicated the support available from the lateral sinus wall for augmentation and implant stability |
| Thickness of the palatal walls (MWT) (mm) | The medial or palatal wall of the maxillary sinus | The thickness of the palatal wall was measured from the outer cortical bone to the sinus membrane. | This assessment determined the bone volume available for grafting and implant placement |
| Angle of mediolateral walls (Sinus angle) (°) | The angle between the medial and lateral walls of the sinus | CT scans were used to measure the angle formed by the intersection of lines along the medial and lateral walls of the sinus. | This measurement helped in understanding the sinus anatomy and planning the surgical approach by evaluating wall inclinations |
| Age Group (years) | Male (n=55) | Female (n=30) | Total cases (n=85) | Bilateral sinus augmentation surgery required based on residual bone height (n) | Unilateral sinus augmentation surgery required based on residual bone height (n) |
| 0-20 | 8 | 5 | 13 | 4 | 4 |
| 21-40 | 25 | 6 | 31 | 4 | 17 |
| 41-60 | 19 | 11 | 30 | 4 | 7 |
| 61-80 | 7 | 3 | 10 | 2 | 6 |
| 81-100 | 0 | 1 | 1 | 0 | 0 |
| Parameter | Males (n=55) | Females (n=30) | p-value |
| Right RBH (mm) | 8.05 ± 5.33 | 7.70 ± 5.57 | 0.790 |
| Left RBH (mm) | 6.87 ± 4.28 | 6.14 ± 4.58 | 0.493 |
| Right LWT (mm) | 2.45 ± 0.99 | 2.53 ± 1.18 | 0.772 |
| Left LWT (mm) | 2.89 ± 2.71 | 2.47 ± 1.33 | 0.338 |
| Right MWT (mm) | 7.04 ± 4.15 | 6.42 ± 3.38 | 0.471 |
| Left MWT (mm) | 6.28 ± 3.57 | 6.85 ± 3.85 | 0.518 |
| Right sinus angle (°) | 90.90 ± 14.83 | 91.81 ± 15.70 | 0.804 |
| Left sinus angle (°) | 93.10 ± 15.47 | 81.99 ± 22.02 | 0.009* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Implant Techniques and Outcomes · Sinusitis and nasal conditions · Dental Radiography and Imaging
Introduction
The maxillary sinus (MS) is the first developed, largest paranasal sinus located within the body of the maxilla [1]. The MS is the most clinically significant paranasal sinus as it drains against the gravity into the hiatus semilunaris of the middle meatus [2]. The dimension of the MS varies with age, gender, dentation status, and across races [3,4]. The volume of MS increases up to the second decade in females and the third decade in males, followed by a decrease in size in the next few decades [5]. At an old age, the volume of MS again increases during the process of edentation [4,6].
MS is one of the structures that shows a wide range of variations under physiological and pathological conditions, even across the sides of the same individual [7]. Being the prominent structure with variations, the knowledge about the variation of the MS is important for several maxillofacial, rhinal, and dentistry surgeries. One of those surgeries is the maxillary sinus elevation and augmentation, performed to improve the outcome of the dental screw fixations. Sinus augmentation surgery (SAS), otherwise known as sinus graft or lift, is a surgical procedure performed to improve the alveolar bone height of the posterior maxilla by lifting the lower sinus mucous membrane (Schneiderian membrane) and placing a bone graft or osteogenic materials. Various types of SAS procedures were performed, including crestal, lateral, or palatal window sinus lift surgery. Each method has a wide range of applicability and limitations, which will be selected based on the sinus morphometry.
Several studies have been reported in the literature, with the morphometry of the MS across various ethnic groups [3,4,8,9]. However, their implications in the selection of appropriate SAS techniques and outcomes were limited, especially in the Indian population. The present study aimed to assess age-related variations in maxillary sinus morphometry in the Eastern Indian population and evaluate their impact on the selection of sinus augmentation techniques.
Materials and methods
A retrospective cross-sectional study was conducted jointly in the departments of anatomy and radiodiagnosis after obtaining approval from the Institutional Ethics Committee (T/IM-NF/Anatomy/23/180). The study included 85 patients who underwent computed tomography (CT) of the head and paranasal sinuses between January 2020 and December 2023 for indications unrelated to the maxillary sinus, such as headache, trauma, or other neurological complaints.
Selection criteria
Inclusion criteria were the availability of high-resolution CT scans of the paranasal region with clear visualization of maxillary sinuses in patients aged 0 to 100 years. Exclusion criteria included patients with known or radiologically evident maxillary sinus disease, prior facial surgery, trauma affecting sinus anatomy, congenital craniofacial anomalies, or poor image quality.
Sampling method
A purposive sampling technique was used, wherein suitable cases were identified from the hospital's picture archiving and communication system (PACS) based on inclusion and exclusion criteria.
All CT scans were performed using a 256-slice multi-detector computed tomography (MDCT) scanner (SIEMENS SOMATOM Definition Flash, Germany). Post-processing and measurements were performed using Syngo.Via software (Siemens Healthcare, Germany). Image analysis was carried out independently by two anatomists under the supervision of a senior radiologist. For all measurements, the average of the two observers' values was used for analysis. The anatomical parameters assessed are detailed in Table 1 and illustrated in Figure 1 and Figure 2.
CT section showing the measurement of residual bone height (RBH) in the right maxillary sinus. The RBH is measured as the vertical distance from the alveolar ridge crest to the lowest point of the sinus floor in the coronal section.
CT section showing the measurement of medial wall thickness (MWT) and lateral wall thickness (LWT) in the left maxillary sinus. Additionally, the sinus angle in the right maxillary sinus is measured in the coronal section, showing the angle formed by the intersection of the medial and lateral walls.
The data were summarized using mean ± standard deviation (SD) for continuous variables and frequencies for categorical variables. Inferential statistical tests included paired t-tests for right-left comparisons, independent t-tests for gender differences, and chi-square tests for associations between categorical variables (e.g., age group and SAS requirement). A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics for Windows, Version 25 (Released 2017; IBM Inc., Armonk, New York).
Results
The morphometry data of 85 patients, comprising 55 males (64.7%) and 30 females (35.3%), were included in this study. The mean age of the individual is 38.4 ± 18.3 years. The summary of the case distribution was tabulated in Table 2.
Residual bone height (RBH)
RBH is the crucial factor that determines the need for the SAS prior to the dental implants. The mean RBH on the right and left side was 7.94 ± 5.37 mm and 6.65 ± 4.36 mm, respectively. A paired t-test showed a significant difference between right RBH and left RBH (p=0.02), indicating lateral asymmetry in RBH. The majority of the cases (56.47%) (n=48) have the RBH of 5 mm or less on either or both sides, indicating the potential need for SAS. Out of which 14 cases (29.17%) had less than 5 mm of RBH bilaterally and 34 cases (70.83%) had unilaterally.
Lateral wall thickness (LWT)
The thickness of the lateral wall of the maxillary sinus is crucial in selecting the appropriate surgical technique for SAS. The mean LWT of the maxillary sinus on the right and left side was 2.48 ± 1.04 mm and 2.76 ± 2.38 mm, respectively. There was no statistically significant difference in the laterality (p=0.312, paired t-test). In patients requiring SAS, eight cases (16.67%) had an LW of 1.5 mm or less, making them suitable for the lateral window technique, while the remaining 40 cases (83.33%) had an LW greater than 1.5 mm, suggesting the crestal approach might be more appropriate. Out of eight cases, one case (2.08%) was suitable for the bilateral lateral window approach.
Mediolateral wall thickness (MWT)
Mediolateral wall thickness (MW) is important for understanding the structural integrity of the sinus cavity. The mean MWT of the maxillary sinus on the right and left side was 6.85 ± 3.92 mm and 6.45 ± 3.65 mm, respectively. A paired t-test revealed no significant difference between the two sides (p=0.226). Although MW is not directly used in deciding the surgical technique for SAS, it provides additional context regarding anatomical variations of the maxillary sinus.
Sinus angle
The angle between the lateral and medial walls of the maxillary sinus (sinus angle) is a critical parameter influencing surgical access during SAS. The mean sinus angle of the right and left sides was 91.18° ± 15.02° and 89.70° ± 18.33°, respectively. The difference between these angles was not statistically significant (p=0.477, paired t-test). While the sinus angle is not a primary criterion for determining SAS, extreme angles could complicate the surgical approach.
Comparison of morphometric parameters by gender
An independent t-test was conducted to compare morphometric parameters between males and females. The results are summarized in Table 3. No significant differences were observed between males and females for RBH, LWT, MWT, or right sinus angle, suggesting that these parameters are relatively consistent across genders. However, only the left sinus angle shows significantly more in males when compared to females, with p=0.009.
Table 3: Gender comparison of morphometric parameterRBH - residual bone height; LWT - lateral wall thickness; MWT - medial wall thickness p<0.05*
Need for sinus augmentation surgery (SAS)
Based on the morphometric analysis, 48 cases (56.47%) were identified as requiring SAS due to insufficient RBH (≤5 mm). Among these, the distribution of the required surgical techniques was as follows: eight cases (16.67%) of lateral window technique were indicated for this approach due to an LW of 1.5 mm or less. Out of which one is bilateral (2.08%). Crestal approach: 40 cases (83.34%) were better suited for this technique, with an LW greater than 1.5 mm. The requirement for sinus augmentation surgery (SAS) was significantly more prevalent in the 21-40-year age group (χ²(3)=10.84, p=0.013, Cramér's V=0.34). Post-hoc comparisons revealed this difference was specifically significant between the 21-40 group (67.7% prevalence) and the 41-60 group (36.7% prevalence; χ²(1)=6.93, p=0.008, φ=0.33) with no significant gender-based differences. This reflects the increased likelihood of early or moderate alveolar bone resorption in these populations.
Discussion
In elderly patients, tooth loss often leads to the resorption of the alveolar ridge and the pneumatization of the maxillary sinus. These changes can significantly reduce the likelihood of successful outcomes in dental rehabilitation surgeries. To enhance the effectiveness of these rehabilitation procedures, SAS is frequently performed, particularly when the RBH is less than 5 mm. The present study aims to evaluate the morphometry of the maxillary sinus across various age groups within the Indian population, thereby providing valuable insights into the necessity and optimal selection of SAS tailored to this demographic.
Research indicates that SAS can achieve a remarkable success rate, reportedly reaching 100%, with graft survival extending up to three years during follow-up. This success is contingent upon the careful selection and execution of the surgical technique, which should be informed by the anatomical morphometry of the maxillary sinus [10]. Several anatomical parameters are critically evaluated prior to surgical planning, including RBH, LWT, MWT, sinus angle, sinus membrane thickness, and the presence, direction, and height of sinus septa. Additionally, factors such as the type of edentulism, the palatonasal recess angle, and the diameter of the alveolar antral artery also play essential roles in preoperative assessments [9,11-13]. Notably, Lyu et al. emphasized the importance of considering sinus health alongside anatomical factors in the decision-making process for SAS [11].
In our study, we observed that the RBH is significantly lower on the left side compared to the right, a finding that aligns with previous research conducted on the Korean population [14]. However, our results also indicate that there is no significant variation in RBH between the right and left sides, which corroborates existing literature. It is important to note that most studies focusing on the morphometry of the maxillary sinus in the Indian population have primarily documented parameters such as volume, height, surface area, and width [8,15-18]. To the best of our knowledge, our study is pioneering in documenting the RBH and elucidating its clinical significance in the context of SAS.
While this study provides valuable insights into maxillary sinus morphometry and its implications for SAS, certain limitations should be acknowledged. The sample size, though adequate for preliminary analysis, was confined to a single geographic region (Eastern India), which may not fully represent the broader Indian population. The retrospective design, while efficient, relies on pre-existing imaging data, which may introduce variability in scan quality and patient selection. Although inter-observer agreement was ensured by averaging measurements between two anatomists, subtle discrepancies in landmark identification could persist. The cross-sectional nature of the study also limits the ability to assess age-related changes over time. Finally, while morphometric parameters were correlated with SAS suitability, clinical outcomes such as postoperative complications or graft success rates were not evaluated.
Conclusions
This study provides a comprehensive evaluation of the morphometric variations of the MS across different age groups within the Eastern Indian population. Our findings reveal significant anatomical variations in the MS, which play a crucial role in determining the appropriate technique for SAS. These variations, particularly in parameters such as RBH, LWT, and MWT, must be carefully considered during preoperative planning to ensure optimal surgical outcomes. The results also highlight the importance of tailoring SAS procedures, such as crestal or lateral window techniques, based on individual sinus anatomy. This personalized approach can enhance the success rate of SAS by addressing the specific anatomical challenges presented by the patient's sinus morphology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Contemporary Implant Dentistry Misch Misch CECE Mosby 2007 https://www.google.co.in/books/edition/Contemporary_Implant_Dentistry/n M 4JAQAAMAAJ?hl=en&gbpv=1&bsq=%C 2%A 0Misch%27s,+Contemporary+Implant+Dentistry+-+E-Book,+Contemporary+Implant+Dentistry.+3rd&dq=%C 2%A 0Misch%27s,+Contemporary+Implant+Dentistry+-+E-Book,+Contemporary+Implant+Dentistry.+3rd&printsec=frontcover
- 2A literature review of the maxillary sinus with special emphasis on its anatomy and odontogenic diseases associated with it Egypt J Otolaryngol Somayaji K Muliya VS Kg MR Malladi UK Nayak SB 113392023
- 3Morphological aspects of the maxillary sinus Paranasal Sinuses Anatomy and Conditions Bozhikova E Uzunov N Bozhikova E Uzunov N Intech Open 2021
- 4Morphological analysis of the human maxillary sinus using three-dimensional printing Contemp Clin Dent Araneda N Parra M González-Arriagada WA Del Sol M Haidar ZS Olate S 2942981020193230829310.4103/ccd.ccd_548_18PMC 7145240 · doi ↗ · pubmed ↗
- 5The analysis of maxillary sinus aeration according to aging process; volume assessment by 3-dimensional reconstruction by high-resolutional CT scanning Otolaryngol Head Neck Surg Jun BC Song SW Park CS Lee DH Cho KJ Cho JH 42943413220051574685710.1016/j.otohns.2004.11.012 · doi ↗ · pubmed ↗
- 6The development and pathologic processes that influence maxillary sinus pneumatization Anat Rec (Hoboken) Lawson W Patel ZM Lin FY 1554156329120081895149610.1002/ar.20774 · doi ↗ · pubmed ↗
- 7Anatomical and pathological assessment of the maxillary sinus using CBCT imaging: a retrospective descriptive study Acta Stomatol Croat HadžiabdićN ImamovićA DžankovićA KoraćS Tahmiščija I 53675920254022582510.15644/asc 59/1/6PMC 11984808 · doi ↗ · pubmed ↗
- 8Sexual dimorphism of maxillary sinus: a morphometric analysis using computed tomography J Lumbini Med College Kandel S Shrestha R Sharma R Sah SK 26426982020