Recurrent Hyponatremia Mimicking Syndrome of Inappropriate Antidiuretic Hormone Secretion: A Case of Partial Empty Sella Syndrome With Isolated Adrenocorticotropic Hormone Deficiency
Revathi Rajendran, Amirthalingeswaran Govindan

TL;DR
A 45-year-old man with recurring low sodium levels was found to have adrenal insufficiency linked to partial empty sella syndrome, highlighting the importance of proper diagnosis to avoid mismanagement.
Contribution
This case highlights adrenal insufficiency as a cause of recurrent hyponatremia mimicking SIADH in the context of partial empty sella syndrome.
Findings
The patient's hyponatremia resolved with corticosteroid treatment, indicating adrenal insufficiency.
Low cortisol and ACTH levels confirmed isolated ACTH deficiency as the primary cause.
Partial empty sella syndrome was diagnosed as an underlying anatomical condition.
Abstract
Hyponatremia is one of the most frequently encountered electrolyte disturbances in clinical practice and can serve as the initial manifestation of various underlying conditions. Severe cases are often associated with neurological dysfunction and an increased risk of mortality. While syndrome of inappropriate antidiuretic hormone hypersecretion (SIADH) remains the most common cause, a thorough diagnostic evaluation is essential, as simple sodium supplementation may lead to recurrent hyponatremia and serious complications. Notably, adrenal insufficiency can closely mimic SIADH, and mismanagement in this context may exacerbate the condition. Hereby, we present the case of a 45-year-old male who experienced recurrent episodes of hyponatremia and was ultimately diagnosed with partial empty sella syndrome. The strong temporal association between corticosteroid administration and symptom…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3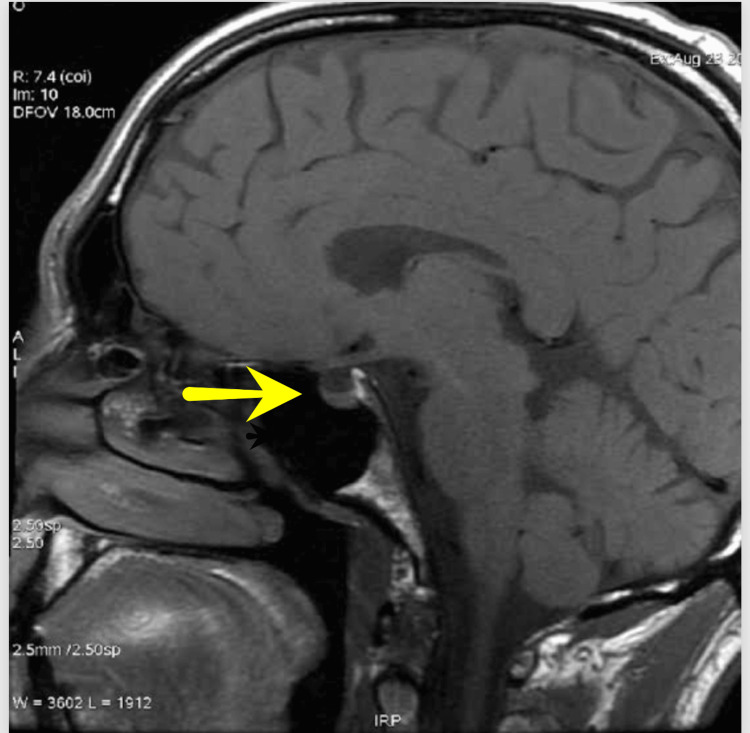 Figure 4
Figure 4| Test | Results | Reference Range | Interpretation |
| Initial serum sodium | 106 meq/L | 135-145 meq/L | Hyponatremia |
| Initial serum osmolality | 221 mosm/kg | 275-295 mosm/kg | Low serum osmolality |
| Initial urinary sodium | 126 mmol/L | 20-100 mmol/L | High urine sodium |
| Initial urinary osmolality | 292 mosm/kg | 100-200 mosm/kg | High urine osmolality |
| Initial serum potassium | 4.0 meq/L | 3.5-5.5 meq/L | Normal |
| Blood urea nitrogen | 12 mg/dL | 7-20 mg/dL | Normal |
| Serum creatinine | 1.1 mg/dL | 0.7-1.3 mg/dL | Normal |
| Serum uric acid | 2.4 mg/dL | 4-8 mg/dL | Low uric acid |
| Serum sodium after correction | 110 mg/dL | 135-145 mmol/L | Hyponatremia |
| Serum osmolality after correction | 260 mosm/kg | 275-295 mosm/kg | Low serum osmolality despite correction |
| Urinary sodium after correction | 132 mmol/L | 20-100 mmol/L | High urine sodium |
| Urinary osmolality after correction | 509 mosm/kg | 100-200 mosm/kg | High urine osmolality |
| 8 AM serum cortisol | 3 mcg/dL | 6-8 mgg/dL | Low serum cortisol |
| Serum ACTH | 6 pg/mL | >10 pg/mL | Low serum ACTH |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectrolyte and hormonal disorders · Adrenal Hormones and Disorders · Diet and metabolism studies
Introduction
Hyponatremia is a complex electrolyte disturbance that primarily results from an imbalance between water intake and the kidneys’ ability to excrete free water. One of the key mechanisms involved is the inappropriate secretion of antidiuretic hormone (ADH), leading to water retention and dilutional hyponatremia [1]. Normally, ADH release is regulated by plasma osmolality and effective circulating volume, ensuring proper fluid balance. However, when this regulatory system is disrupted, excess water accumulates, lowering serum sodium levels. Among the various causes of hyponatremia, syndrome of inappropriate antidiuretic hormone hypersecretion (SIADH) is one of the most frequently encountered [2]. It is characterized by euvolemic hyponatremia, inappropriately concentrated urine, paradoxical natriuresis, and the exclusion of other potential causes. However, diagnosing SIADH requires a careful evaluation, as several conditions can present with a similar clinical picture. Adrenal insufficiency, in particular, is a major differential diagnosis, as it closely mimics SIADH but tends to worsen if mismanaged [2]. Since different causes of hyponatremia require distinct treatment approaches, accurately identifying the underlying condition is crucial for appropriate management and better patient outcomes.
Case presentation
This is a 45-year-old male who presented with a new-onset generalized tonic-clonic seizure lasting for five minutes, associated with up-rolling of eyeballs, tongue biting, and postictal confusion, followed by an altered sensorium for one day. He had no prior history of seizures. Notably, for the past two weeks, he had experienced multiple episodes of watery loose stools along with recurrent episodes of non-bilious, non-projectile vomiting. He had no history of fever, trauma, focal neurological deficits, or known comorbidities and was neither an alcoholic nor a smoker. On examination, he was drowsy and unresponsive to both verbal and painful stimuli (GCS-E1V1MI). His vitals revealed a blood pressure of 100/60 mmHg, a pulse rate of 90 per minute, and an oxygen saturation of 95% on room air. His pupils were 3 mm and reactive to light, bilateral plantar reflexes were mute, and he was able to move all four limbs, though cerebellar and cranial nerve functions could not be assessed. Initial investigations showed severe hyponatremia with a sodium level of 106 mEq/L, while renal function, liver function, complete blood count, potassium, ECG (Figure 1), chest X-ray (Figure 2), and a CT brain were all unremarkable (Figure 3).
ECG taken at the time of ER arrival, showing no significant abnormality
Chest X-ray of our case, showing no significant abnormality
CT brain of our patient, showing no significant abnormalityA: CT brain at the level of the basal ganglia showing no abnormality; B: CT brain at the level of the lateral ventricle showing no abnormality
He was started on 3% NaCl, which led to clinical improvement, though he continued to experience persistent hiccups, drowsiness, forgetfulness, and nausea. Urinary sodium was found to be elevated (132 meq/L). Further evaluation revealed persistent hyponatremia (sodium: 110 meq/L) despite correction with NaCl, with a plasma osmolality of 260 mOsm/kg, urine osmolality of 509 mOsm/kg, and a low serum uric acid level of 2.4 mg/dL. His blood glucose levels consistently ranged between 60 and 80 mg/dL despite having a normal diet. An initial assumption of SIADH was considered, though further investigations to rule out other potential causes were made. The thyroid function test was unremarkable, but the 8 AM serum cortisol level was 3 µg/dL (normal: 6-8 µg/dL). A low adrenocorticotropic hormone (ACTH) level of 6 pg/mL (normal: 10 pg/mL) (Table 1) and normal adrenal cortical imaging on CECT abdomen ruled out primary adrenal insufficiency.
Autoimmune markers, including antinuclear antibody (ANA) and extractable nuclear antigen (ENA) profiles, were negative. MRI brain revealed a partially empty sella (Figure 4), confirming the diagnosis of partial empty sella syndrome with isolated ACTH deficiency.
MRI brain, showing partial empty sella
Ophthalmological evaluation showed normal visual fields, and fundus examination did not show any signs of papilledema. The patient was started on physiological replacement doses of oral hydrocortisone (10 mg in the morning after waking up and 5 mg at 3 PM) to correct the secondary adrenal insufficiency. The patient showed significant clinical improvement, with resolution of hyponatremia and altered sensorium, and was advised long-term endocrinology follow-up. This case highlights an uncommon presentation of isolated ACTH deficiency associated with partial empty sella syndrome, initially manifesting as a seizure due to severe hyponatremia, emphasizing the importance of endocrine evaluation in unexplained electrolyte disturbances.
Discussion
We present the case of a 45-year-old male who was admitted with his first episode of severe symptomatic hyponatremia, manifesting as a generalized tonic-clonic seizure, altered sensorium, and biochemical findings consistent with SIADH. He had low serum sodium, high urine osmolality, elevated urinary sodium, and low serum uric acid, which are hallmark features of SIADH [2]. However, the persistence of hyponatremia despite hypertonic saline and the presence of hypoglycemia raised suspicion of an alternative etiology. Subsequent hormonal evaluation revealed low serum cortisol and ACTH levels, and MRI findings confirmed partial empty sella syndrome, establishing the diagnosis of secondary adrenal insufficiency due to isolated ACTH deficiency.
Kazama et al. described a comparable case of secondary adrenal insufficiency due to ACTH deficiency presenting with hyponatremia, which was successfully treated with corticosteroids [3]. The development of hyponatremia in adrenal insufficiency is well-documented and primarily attributed to cortisol deficiency, which leads to increased ADH secretion [4]. In the absence of cortisol’s inhibitory effect on ADH release, free water retention ensues, mimicking the biochemical picture of SIADH [4,5]. This phenomenon was highlighted in the case series by Kumar et al., where adrenal insufficiency was a common cause of euvolemic hyponatremia and often misdiagnosed as SIADH [2]. Similarly, our patient initially fulfilled the diagnostic criteria for SIADH, but the presence of hypoglycemia and persistent symptoms despite sodium correction warranted further endocrine evaluation.
Like our case, the initial presentation was deceptive and mimicked SIADH, underscoring the importance of endocrine evaluation in cases of unexplained hyponatremia. Furthermore, the study by Grammatiki et al. highlighted a rare cause of adrenal insufficiency due to an ectopic posterior pituitary lobe, causing severe hyponatremia due to disrupted hypothalamic-pituitary signaling [1]. While our patient had partial empty sella syndrome, not an ectopic pituitary, both cases point to structural hypothalamic-pituitary anomalies as culprits for hormonal dysregulation.
Empty sella syndrome itself can lead to varying degrees of hypopituitarism, often presenting with nonspecific symptoms, such as headaches, visual disturbances, and biochemical abnormalities [6]. Auer et al. reported that partial or primary empty sella is frequently associated with isolated hormonal deficiencies, especially ACTH, which was mirrored in our case [6]. In contrast, the review by Charoensri et al. provides a structured approach to diagnosing adrenal insufficiency and emphasizes the importance of ACTH measurement and dynamic testing in ambiguous cases [4]. This aligns with our approach, where, despite initially normal imaging and thyroid tests, targeted hormonal workup clinched the diagnosis. Finally, the case reported by Shanthosh Kumar et al. involved primary adrenal insufficiency leading to severe hyponatremia, which differs from our case in etiology but reinforces the necessity to distinguish between primary and secondary causes for tailored therapy [5].
This case reinforces the diagnostic challenge posed by SIADH mimickers and the pivotal role of thorough hormonal evaluation in patients with unexplained or refractory hyponatremia. Timely recognition of secondary adrenal insufficiency, especially isolated ACTH deficiency, can lead to definitive treatment with corticosteroid replacement, preventing potentially fatal complications.
Conclusions
Hyponatremia is a common yet complex electrolyte disturbance that can arise from a variety of underlying conditions, necessitating a thorough diagnostic workup. While SIADH is often the most suspected cause, this case highlights the importance of considering adrenal insufficiency, particularly in patients with persistent or recurrent hyponatremia despite standard treatment. The identification of partial empty sella syndrome in our patient underscores the critical role of endocrine dysfunction in electrolyte imbalances. Misdiagnosing such cases as SIADH without assessing adrenal function can lead to inappropriate management and worsening clinical outcomes. This case emphasizes the need for clinicians to maintain a high index of suspicion for secondary adrenal insufficiency in unexplained hyponatremia, as timely corticosteroid replacement can lead to complete symptom resolution and prevent life-threatening complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patient with severe hyponatremia caused by adrenal insufficiency due to ectopic posterior pituitary lobe and miscommunication between hypothalamus and pituitary: a case report Medicine (Baltimore) Grammatiki M Rapti E Mousiolis AC 095201610.1097/MD.0000000000002872 PMC 499886426962783 · doi ↗ · pubmed ↗
- 2Prevalence of adrenal insufficiency among patients with euvolemic hyponatremia Endocr Connect Kumar A Ghosh M Jacob JJ 162316311020213478822710.1530/EC-21-0500 PMC 8679923 · doi ↗ · pubmed ↗
- 3Hyponatremia due to secondary adrenal insufficiency successfully treated by dexamethasone with sodium chloride Am J Case Rep Kazama I Tamada T Nakajima T 5775801620152631965510.12659/AJCR.894468 PMC 4557418 · doi ↗ · pubmed ↗
- 4A contemporary approach to the diagnosis and management of adrenal insufficiency Endocrinol Metab (Seoul) Charoensri S Auchus RJ 73823920243825347410.3803/En M.2024.1894 PMC 10901672 · doi ↗ · pubmed ↗
- 5A case of severe hyponatremia in a patient with primary adrenal insufficiency Cureus Shanthosh Kumar S Nagesh VK Hunter J Sange I 013202110.7759/cureus.17946 PMC 851420134660134 · doi ↗ · pubmed ↗
- 6Primary empty sella syndrome and the prevalence of hormonal dysregulation Dtsch Arztebl Int Auer MK Stieg MR Crispin A Sievers C Stalla GK Kopczak A 9910511520182951081910.3238/arztebl.2018.0099 PMC 5842341 · doi ↗ · pubmed ↗