Right Ventricular Outflow Tract Endocarditis: A Very Rare Case and Short View
Selman Dumani, Vera Beca, Devis Pellumbi, Stavri Llazo, Edlira Rruci, Daniela Teferici, Altin Veshti

TL;DR
This paper reports a rare case of infective endocarditis in the right ventricular outflow tract of an intravenous drug user, highlighting the importance of surgical intervention for diagnosis and treatment.
Contribution
The paper presents a rare clinical case of RVOT endocarditis and emphasizes the role of surgery in atypical presentations.
Findings
A 30-year-old intravenous drug user presented with RVOT vegetation and tricuspid valve vegetation.
Surgical intervention confirmed fibrinous-thrombotic vegetation and resulted in an uneventful recovery.
RVOT involvement in endocarditis is rare but should be considered in atypical cases.
Abstract
Infective endocarditis involving the right ventricular outflow tract (RVOT) is rare, even among intravenous drug users, and is infrequently encountered by cardiac surgery teams. We report the case of a 30-year-old man with a history of intravenous drug use who presented with a two-month history of fever reaching 39℃. He was initially treated with antibiotics. Transthoracic and transesophageal echocardiography revealed a 2 cm² vegetation on the anterior leaflet of the tricuspid valve, causing severe tricuspid regurgitation, along with a thin, highly mobile, pedunculated mass (1.8-2 cm²) in the RVOT. Surgical intervention was indicated due to the size and mobility of both lesions and the patient's clinical history. The patient underwent tricuspid valve replacement with a No. 33 Epic Supra bioprosthesis and excision of the RVOT mass. Histopathological examination confirmed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
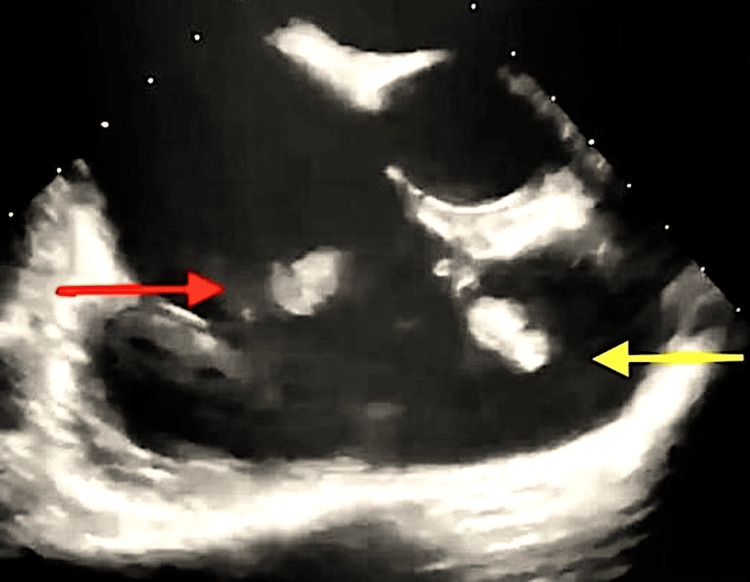 Figure 1
Figure 1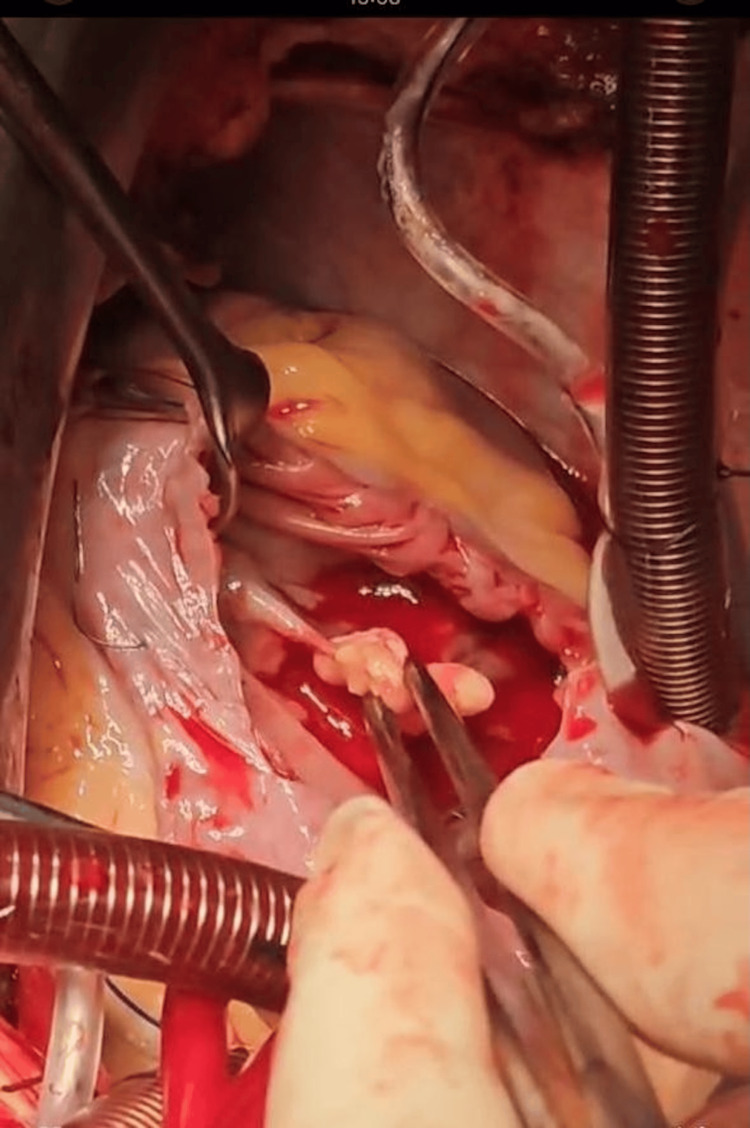 Figure 2
Figure 2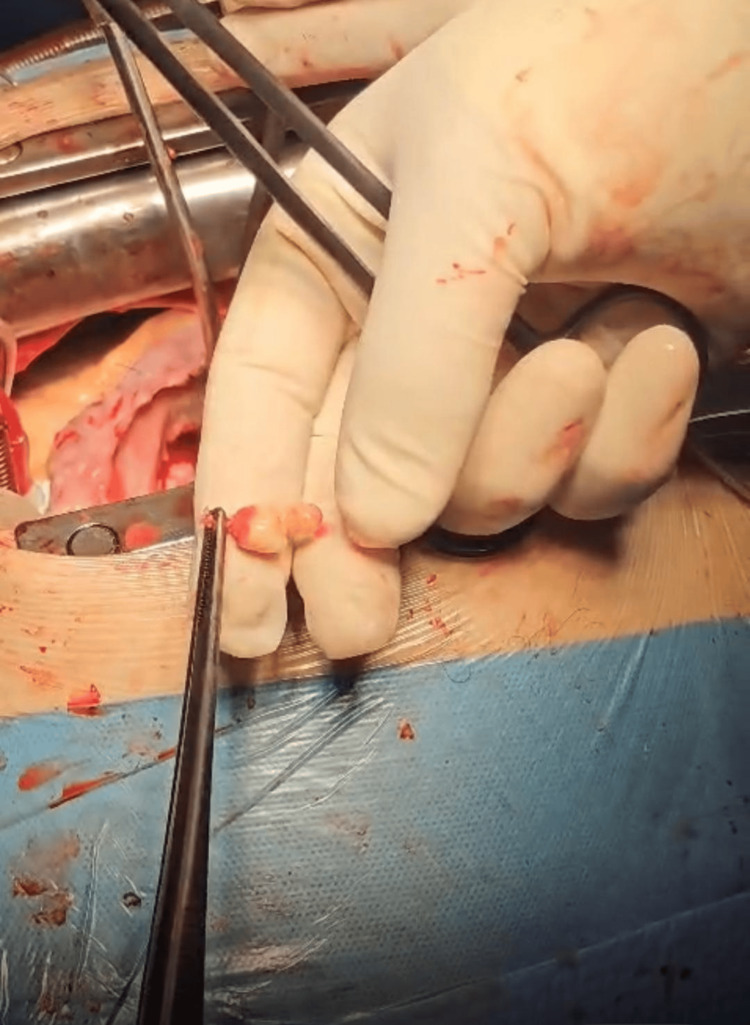 Figure 3
Figure 3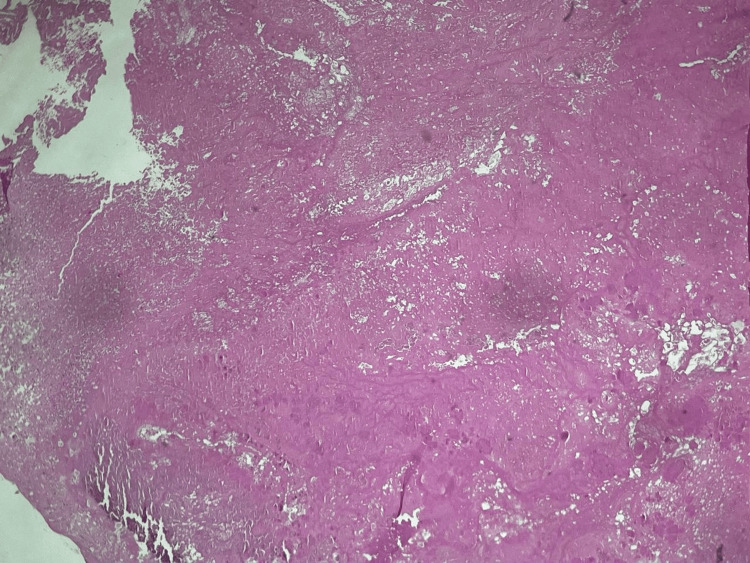 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair
Introduction
Infective endocarditis involving the right ventricular outflow tract (RVOT) is rare, even among intravenous drug users, and is infrequently encountered by cardiac surgery teams.
Right-sided endocarditis is commonly associated with intravenous drug use. However, it can also occur in other clinical contexts, including right-sided heart catheterization, pacemaker implantation, or congenital heart defects. The incidence of infective endocarditis among intravenous drug users ranges from 1.5 to 20 cases per 1,000 users annually [1]. In the United States, the reported incidence is between 1.5 and 3.3 cases per 1,000 users annually [2]. Acute infection accounts for 60% of all hospital admissions among intravenous drug users, while tricuspid valve endocarditis represents 5-15% of hospitalized cases [2,3]. Additionally, the annual incidence of infective endocarditis among drug users varies between 2% and 5%, contributing to 5-10% of overall mortality in this population [4].
In our case, the patient presented with vegetations on both the RVOT and the tricuspid valve (anterior and septal leaflets). To our knowledge, simultaneous involvement of the tricuspid valve and the RVOT has not been previously reported in the literature.
Case presentation
A 30-year-old man with a 10-year history of intravenous drug use, under medical treatment supervised by a toxicologist, was admitted to the Infectious Diseases Department where he started intravenous antibiotic therapy. He reported a two-month history of fever reaching 39°C, although he had been afebrile for the past two weeks. On examination, his general condition was stable, with dyspnea on minimal exertion, a blood pressure of 110/70 mmHg, and an oxygen saturation of 97%. Laboratory findings revealed normocytic anemia (hemoglobin 8.6 g/dL; normal reference range 12.1-15.9 g/dL), elevated C-reactive protein (CRP) (6.04 mg/dL; normal reference range <0.5 mg/dL), and a normal white blood cell (WBC) count (5700/μL; normal reference range 4000-10500/μL). Biochemical parameters were within normal limits.
Transesophageal echocardiography revealed a 2 cm² vegetation on the anterior leaflet of the tricuspid valve, associated with severe tricuspid regurgitation and a pulmonary artery systolic pressure of 41 mmHg. The right atrium and right ventricle were dilated; however, right ventricular function was preserved. A highly mobile, pedunculated mass measuring approximately 1.8-2 cm^2^ was also observed in the RVOT. The aortic and pulmonary valves were normal, the interatrial septum was intact, the left atrial appendage was free, and the mitral valve was functioning normally (Figure 1).
Vegetation on the tricuspid valve (red arrow) and the right ventricular outflow tract (yellow arrow)
Under these conditions, surgical intervention was indicated. The surgery was performed through a median sternotomy with aorto-bicaval cannulation. Following aortic cross-clamping and cardioplegic arrest, the right atrium was incised. Intraoperative inspection revealed the complete destruction of the tricuspid valve, with vegetations extending from the anterior to the septal leaflet, making repair unfeasible.
Additionally, a fragile mass with a very small, thin peduncle was visualized in the RVOT. The tricuspid valve, along with the vegetations, was excised and replaced with a No. 33 Epic Supra bioprosthesis. The excised formations were sent for histopathological and microbiological examination. The right atrium was closed, the aorta was subsequently declamped, and the remainder of the operation proceeded without complication.
The photos below were taken in the operating room during intervention (Figures 2-3).
Vegetation attached to the anterior leaflet (between forceps)
The excised vegetation of the right ventricular outflow tract with a small and very thin peduncle
Postoperatively, the patient had an uneventful recovery. At discharge, transthoracic echocardiography demonstrated a normally functioning tricuspid bioprosthesis with a mean gradient of 4 mmHg and no paravalvular leak. Left ventricular function was normal, with no pericardial or pleural effusion.
Histopathological examination revealed fibrinous-thrombotic vegetations on the tricuspid valve and the RVOT mass (Figure 4). The microbiological culture was sterile. The patient was transferred to the Infectious Diseases Department to continue intravenous antibiotic therapy.
Fibrinous-thrombotic vegetation
Discussion
Right-sided endocarditis is commonly associated with intravenous drug use. However, it can also occur in other clinical contexts, including right-sided heart catheterization, pacemaker implantation, or congenital heart defects. The incidence of infective endocarditis among intravenous drug users ranges from 1.5 to 20 cases per 1,000 users annually [1]. In the United States, the reported incidence is between 1.5 and 3.3 cases per 1,000 users annually [2]. Acute infection accounts for 60% of all hospital admissions among intravenous drug users, while tricuspid valve endocarditis represents 5-15% of hospitalized cases [2,3]. Additionally, the annual incidence of infective endocarditis among drug users varies between 2% and 5%, contributing to 5-10% of overall mortality in this population [4]. In the "International Collaboration on Endocarditis-Prospective Cohort Study", which included 2,781 patients with infective endocarditis, 10% had a history of intravenous drug use [5].
In our case, the patient presented with vegetations on both the RVOT and the tricuspid valve (anterior and septal leaflets). To our knowledge, simultaneous involvement of the tricuspid valve and the RVOT has not been previously reported in the literature.
Vegetations are most commonly found on the tricuspid valve but are rarely observed in the RVOT or on the ventricular side of the pulmonary valve [6]. Tricuspid valve involvement has been reported in 90% of right-sided infective endocarditis cases associated with intravenous drug use [7]. However, other right heart structures, including the pulmonary valve, may also be affected. Simultaneous tricuspid and pulmonary valve endocarditis is possible [8]. Isolated pulmonary valve endocarditis is rare, accounting for <2% of all cases, with approximately 70 cases reported between 1979 and 2013 [9].
Sabzi et al. reported a case of isolated RVOT endocarditis due to brucellosis in which the vegetation was attached to the muscular bundle in the right ventricle, with no tricuspid valve involvement. In that case, the vegetation was surgically excised [10].
The most common complications of tricuspid valve endocarditis include valvular regurgitation, abscess formation, and septic pulmonary embolism [11]. In our case, the patient presented with severe valvular regurgitation caused by endocarditis, without evidence of abscess formation or pulmonary complications.
Surgical indications for right-sided infective endocarditis include vegetations >20 mm, persistent bacteremia lasting more than seven days despite antibiotic treatment, right-sided heart failure due to tricuspid valve insufficiency, recurrent pulmonary emboli, and abscess formation, particularly in prosthetic valves [12]. In this patient, the indication for urgent surgery was based on the presence of a relatively large (1.8-2 cm²) pedunculated RVOT mass, severe tricuspid valve destruction, and the patient's age and clinical status.
Specifically, for tricuspid valve infective endocarditis, 5-40% of patients require surgical intervention [13]. However, surgical management of tricuspid valve endocarditis remains a subject of debate. Valve repair is generally preferred over replacement due to the lower risk of reinfection and reintervention with prosthetic valves [14]. Surgical techniques are classified as either prosthetic (valve replacement or ring annuloplasty) or non-prosthetic (annuloplasty, isolated vegetation excision, or total valve excision) [6]. In patients with tricuspid valve endocarditis related to intravenous drug use, the surgical approach should aim to avoid the use of prosthetic materials and instead focus on vegetation removal and valve repair, as this is associated with better long-term survival [7]. The principle of complete removal of infected tissue and restoration of valve function should be balanced with efforts to minimize the implantation of foreign material. In our case, the anterior leaflet was completely destroyed, and the septal leaflet was partially involved, rendering repair infeasible. Therefore, we performed tricuspid valve replacement using a No. 33 Epic Supra bioprosthesis.
In a study by Yanagawa et al. involving 1,165 patients with tricuspid valve endocarditis, 60% underwent tricuspid valve repair and 40% underwent valve replacement, primarily with bioprosthetic valves. Both approaches showed similar long-term survival; however, valve repair was associated with a longer freedom from recurrent endocarditis, lower reintervention rates, and fewer pacemaker implantations [15]. Similarly, Di Mauro et al. reported no significant difference in short- or long-term survival between tricuspid valve repair and replacement over 25 years among 157 patients with right-sided endocarditis [16].
Histopathological examination of the formation is essential to differentiate between thrombus, Löffler endocarditis, and cardiac tumors. Right-sided cardiac tumors are rare and are most commonly located in the right atrium [17]. Myxomas are the most common type of primary cardiac tumor, originating in the right atrium in approximately 3% of cases, and in about 10% of cases, they originate from the tricuspid valvular apparatus, specifically from the chordae tendineae or papillary muscles [18]. Operative mortality for first-time isolated tricuspid valve surgery ranges from 0% to 15% [16]. In our case, the postoperative course was uneventful.
Conclusions
Right-sided endocarditis is closely associated with intravenous drug use, with the tricuspid valve being the most commonly affected site. Involvement of the RVOT is exceedingly rare. Early diagnosis and appropriately timed intervention, whether medical or surgical, are critical to achieving optimal outcomes. This case report highlights the need for individualized management strategies to improve patient prognosis. A multidisciplinary team is very important to achieve the main the best results. Surgery remains the gold standard for definitive diagnosis and treatment, even in uncommon locations. It can be performed with very good results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Right-side endocarditis in injection drug users: review of proposed mechanisms of pathogenesis Clin Infect Dis Frontera JA Gradon JD 3743793020001067134410.1086/313664 · doi ↗ · pubmed ↗
- 2Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America Circulation Baddour LM Wilson WR Bayer AS 0434111200510.1161/CIRCULATIONA · doi ↗ · pubmed ↗
- 3Clinical manifestations and outcome in Staphylococcus aureus endocarditis among injection drug users and nonaddicts: a prospective study of 74 patients BMC Infect Dis Ruotsalainen E Sammalkorpi K Laine J Huotari K Sarna S Valtonen V Järvinen A 137620061696562510.1186/1471-2334-6-137PMC 1584240 · doi ↗ · pubmed ↗
- 4Infective endocarditis and cardiac surgery in intravenous drug abusers and HIV-1 infected patients Cardiol Clin MiróJM del Río A Mestres CA 1670167-84, v-vi 2120031287489110.1016/s 0733-8651(03)00025-0 · doi ↗ · pubmed ↗
- 5Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study Arch Intern Med Murdoch DR Corey GR Hoen B 46347316920091927377610.1001/archinternmed.2008.603PMC 3625651 · doi ↗ · pubmed ↗
- 6Right-sided infective endocarditis 2020: challenges and updates in diagnosis and treatment J Am Heart Assoc Shmueli H Thomas F Flint N Setia G Janjic A Siegel RJ 09202010.1161/JAHA.120.017293 PMC 779223132700630 · doi ↗ · pubmed ↗
- 7Right-sided infective endocarditis: surgical management Eur J Cardiothorac Surg Akinosoglou K Apostolakis E Koutsogiannis N Leivaditis V Gogos CA 4704794220122242739010.1093/ejcts/ezs 084 · doi ↗ · pubmed ↗
- 8Isolated pulmonic valve endocarditis presenting as neck pain J Community Hosp Intern Med Perspect Goud A Abdelqader A Dahagam C Padmanabhan S 29647520152665369710.3402/jchimp.v 5.29647 PMC 4677583 · doi ↗ · pubmed ↗