Avoiding harm in pediatric heatstroke: Lessons from a case of ice-related frostbite
Mor Rittblat, Shiran Katabi, Dmitry Kotovich, Stav S. Cahan, Ysh-ia Langer

TL;DR
A 22-month-old child developed frostbite from ice packs used to treat heatstroke, highlighting the need for safer cooling protocols in pediatric patients.
Contribution
This case report highlights the risk of iatrogenic frostbite in pediatric heatstroke treatment using ice packs.
Findings
Direct ice pack application caused full-thickness frostbite in a 22-month-old heatstroke patient.
The child required surgical debridement and skin grafting but recovered without long-term effects.
The case emphasizes the need for pediatric-specific cooling protocols to prevent complications.
Abstract
Heatstroke is a life-threatening medical emergency characterized by a core body temperature exceeding 40 °C (104°F). Prompt and effective cooling is critical to prevent multiorgan failure and death. However, aggressive cooling techniques, if improperly applied, may lead to iatrogenic complications. We present a pediatric case of severe frostbite injury resulting from direct ice pad application during emergency treatment for heatstroke. A 22-month-old infant was found unconscious after being left unattended in a parked car and was diagnosed with severe heatstroke. During prehospital care, direct ice packs were applied per emergency protocol. On admission, erythematous skin lesions were noted on both anterior thighs, which progressed to full-thickness eschars. The plastic surgery team later confirmed these as frostbite injuries. The patient underwent surgical debridement and autologous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
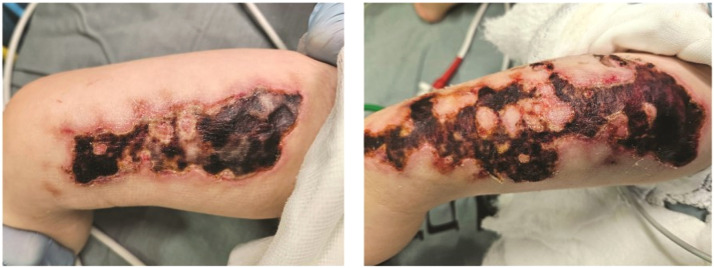 Figure 1
Figure 1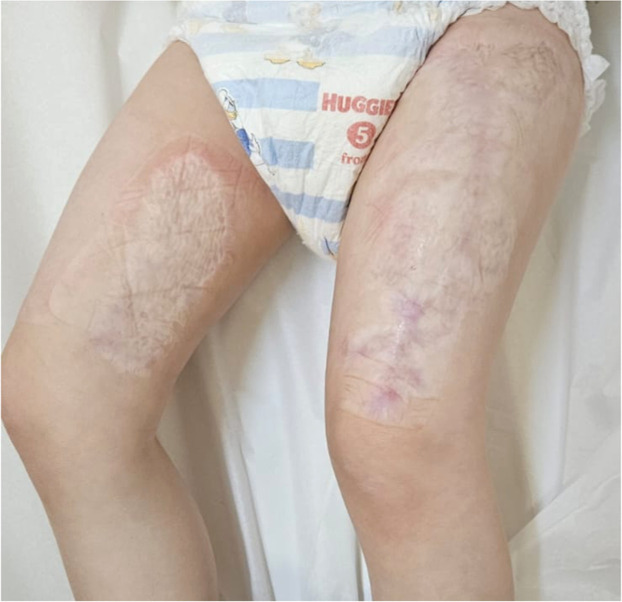 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClimate Change and Health Impacts · Thermoregulation and physiological responses · Thermal Regulation in Medicine
Introduction
Heatstroke is a medical emergency defined by core body temperature 40 °C (104 °F) often due to environmental heat exposure or exertion. It causes systemic inflammatory response, multiorgan dysfunction, and CNS damage.1 The pathophysiology of heatstroke involves the failure of thermoregulatory mechanisms,2 leading to systemic inflammatory response, cellular injury, and multiorgan dysfunction.1 Clinical manifestations include altered mental status, ranging from confusion to coma, hot and dry skin, and potential progression to rhabdomyolysis and disseminated intravascular coagulation.2 The pediatric population is prone to rapid heatstroke development due to the immature thermoregulatory systems, higher metabolic rate, inefficient sweating mechanisms, and greater surface area-to-body mass ratio.3
Prompt cooling is lifesaving, but method selection is critical. Direct ice application, though historically used, may cause cold-induced injuries, particularly in pediatric patients with delicate skin. We present a case where the initial cooling method used in the field was not clearly communicated, leading to a diagnostic challenge. This report aims to raise awareness of cold-induced injuries as a possible complication of emergency cooling, and to highlight the importance of clear communication and vigilance in early diagnosis.
Case report
A 22-month-old girl presented in our institute after being left unattended in a parked car for several hours. She was rescued and brought to the pediatric emergency department (PED) by Emergency Medical Services (EMS). Upon transport, ice was applied in order to reduce core temperature. On arrival to the emergency department, she exhibited signs of severe heatstroke, including hyperthermia, altered consciousness, tachycardia and hypotension. During stabilization erythema was noticed on both anterior thighs, initially thought to be thermal burns from sun exposure or sun-heated surfaces (e.g., metal buckles), delaying recognition of frostbite. A few days into the Pediatric Intensive Care Unit (PICU) admission, these lesions developed to sever full thickness eschar as shown in Figure 1.Figure 1A photo of the preoperative lesions a few days into the Pediatric Intensive Care Unit admission.Figure 1
Given the clinical course, including the rapid progression from local erythema to full-thickness eschar, and the application of ice during transport, the diagnosis of frostbite was made by the plastic surgery team in the burn unit. The burns affected 5 % of her total body surface area (TBSA), with 3 % on the left thigh and 2 % on the right thigh. The patient underwent surgical debridement of burn wounds followed by autologous skin grafting on postburn day 15, using split-thickness skin from the right thigh. The surgery was successful (Figure 1S), and the postoperative course was uneventful. The patient was discharged and continued follow-up care at the burn clinic (Figures 2S and 3S). At her follow-up visit at one year postoperatively, the patient demonstrated normal scar healing and achieved full clinical recovery without any long-term complications or wound-related sequelae as shown Figure 2.Figure 2A photo of the follow-up visit one year postoperatively at the burn clinic.Figure 2
Discussion
Heatstroke is a life-threatening emergency requiring prompt diagnosis and rapid cooling. Pediatric patients are especially vulnerable due to immature thermoregulation, and higher surface area-to-mass ratios.1 Rapid reduction of core temperature remains the cornerstone of management, but the method must balance efficacy with safety.
Whole-body immersion in ice water is considered the most effective cooling method in adults, with high cooling rates (0.20–0.35 °C/min).2^,^4 It’s the preferred method for healthy, young, and well-trained athletes.2 However, it poses risks in young children, including cold shock, arrhythmias, and skin injury.3^,^4 Similarly, ice pack application—especially when unwrapped or applied for prolonged periods—can cause frostbite, as illustrated in our case. However, when used strategically, they should be wrapped in towels and moved frequently.5 Additional in-direct, evaporative cooling techniques, which use air-conditioning, fans and misting devices, enhance heat loss from the skin surface by leveraging the high latent heat of vaporization.4
Controversy exists over what therapeutic modality is most effective in the treatment of heatstroke. Yet, the basic premise of rapidly lowering the core temperature to 39 °C remains the primary goal.1^,^2 To date, there is limited knowledge regarding the management of heatstroke in the pediatric population compared to adults.4 We recommend: (1) avoiding direct ice application in pediatric patients, (2) prioritizing evaporative cooling techniques, and (3) adopting conservative cooling rates (∼0.10 °C/min). Next steps include developing pediatric-specific EMS protocols, training providers in safe cooling practices, and encouraging structured communication between prehospital and in-hospital teams.
Conclusion
While direct ice contact is a well-known risk factor for skin injury, this case highlights a more subtle diagnostic and communication challenge. The frostbite was initially unrecognized, with early signs misinterpreted as thermal burns due to prolonged sun exposure or contact with hot metal surfaces. The delay in identifying the true etiology was partly due to incomplete communication regarding prehospital interventions. This underscores the need for heightened clinical suspicion of frostbite during heatstroke treatment, and emphasizes the need for safer, pediatric-specific cooling protocols. We recommend caution with direct-contact cooling and prioritization of evaporative methods, along with caregiver and provider education to enhance safety and outcomes.
Author contributions
MR—Data curation, Investigation, Writing—original draft; YL—Conceptualization, Data curation, Investigation, Project administration, Supervision, Validation, Visualization, Writing—original draft, Writing—review and editing; SK—Writing—original draft; DK—Writing—original draft; SCC—Conceptualization, Data curation, Investigation, Project administration, Supervision, Validation, Visualization, Writing—review and editing.
Financial support
The authors report no financial support to declare.
Data availability statement
Full demographic data pertaining to individuals cannot be disclosed in order to ensure subjects’ anonymity and data security policies. Derived data supporting the findings of this study may be made available from the corresponding author MR upon request.
Ethics, consent to participate, and consent to publish declarations
Written informed consent for publication of the clinical details and clinical images was obtained from the guardian of the patient.
Declaration of competing interest
MR, YL, SK, DK, SSC reports no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bouchama A.Knochel J.P.Heat stroke N Engl J Med 3462520021978198810.1056/NEJ Mra 01108912075060 · doi ↗ · pubmed ↗
- 2Epstein Y.Yanovich R.Heatstroke N Engl J Med 3802520192449245910.1056/NEJ Mra 181076231216400 · doi ↗ · pubmed ↗
- 3Falk B.Dotan R.Children's thermoregulation during exercise in the heat: a revisit Appl Physiol Nutr Metab 332200842042710.1139/H 07-18518347699 · doi ↗ · pubmed ↗
- 4Jamal D.Abdelgadir I.Powell C.V.E.Cooling methods for paediatric heat-induced illnesses Arch Dis Child 1064202140540610.1136/archdischild-2020-31990533127613 · doi ↗ · pubmed ↗
- 5Lissoway J.B.Lipman G.S.Grahn D.A.Novel application of chemical cold packs for treatment of exercise-induced hyperthermia: a randomized controlled trial Wilderness Environ Med 262201517317910.1016/j.wem.2014.11.00625771030 · doi ↗ · pubmed ↗