Exploring Patient Understandings of Navigation Services Within Alberta's Healthcare System: A Qualitative Study
Sarah Rabi, Maria Santana, Gina Dimitropoulos, Kerry McBrien, Eleanor Benterud, Lorraine Wigston, Karen Tang

TL;DR
This study explores how patients in Alberta understand and value patient navigation services, highlighting key features that make these programs effective.
Contribution
The study identifies consistent patient-perceived functions and characteristics of patient navigators across diverse programs.
Findings
Patients value personalized, seamless, and humanized care provided by navigators.
Approachability, accessibility, and systems knowledge are key navigator characteristics.
Program settings and patient needs influence how these functions are implemented.
Abstract
Patient navigation was first envisioned to assist marginalized cancer patients access timely healthcare services by identifying and addressing social barriers to care. While this understanding of patient navigation may still hold for a subgroup of programs today, its expansion over the past 30 years has resulted in a diverse set of interventions with distinct care settings, patient eligibility criteria, navigator training requirements and program goals. This study aimed to explore patients' understanding of patient navigation programs to identify program features that are of particular value and importance to them. In this qualitative study, we conducted one‐on‐one semi‐structured interviews from November 2023 to February 2024 with patients involved in five distinct hospital‐, clinic‐ and community‐based patient navigation programs across Alberta. Inductive thematic analysis and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
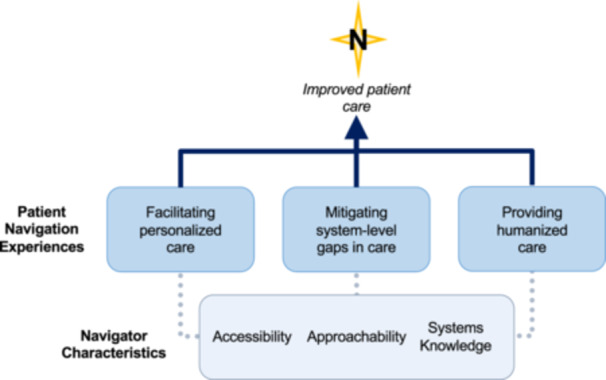 Figure 1
Figure 1| Variable | Categories | Frequency, |
|---|---|---|
| Age | ||
| 18–24 | 3 (13) | |
| 25–64 | 12 (52) | |
| 65 and up | 8 (35) | |
| Gender | ||
| Women | 12 (52) | |
| Men | 11 (48) | |
| Educational attainment | ||
| Less than high school | 5 (22) | |
| High school diploma | 11 (48) | |
| College and bachelor's degree | 6 (26) | |
| Graduate degree | 1 (4) | |
| Employment status | ||
| Employed | 4 (17) | |
| Unemployed | 7 (30) | |
| On disability leave | 6 (26) | |
| Retired | 6 (26) | |
| Navigator type | ||
| Nurse navigator | 11 (48) | |
| Social work navigator | 3 (13) | |
| Lay navigator | 9 (39) | |
| Relationship Duration | ||
| Less than 3 months | 6 (26) | |
| 3 months to 1 year | 10 (44) | |
| More than 1 year | 7 (30) |
| Themes | Quotes |
|---|---|
| Personalized Care |
‘They know me better [after 15 years]. They know my frailties, my bones, my feet. They have never failed to ask me how things are going. That way they understand my outside issues as well as the chemo treatments… They know me better and they are truly interested in their patients.’ (Participant 1 – woman, nurse PN program) ‘[The navigator] definitely helped me find who I was within the healthcare system and my personal life as well. She was able to talk to my doctors if I didn't hear from them… and she kind of kicked them in gear a bit, which was nice, but also knowing that she had my back and she believed me like, ‘Okay, so how can we fix this? How can I help you to become your own independent person? … I want you to find who you are so that I can help you with everything else.’ Yeah, she was just a very positive person and I loved that.’ (Participant 10 – woman, social work PN program) ‘[The navigator] is multitasking what [another clinic] was doing with the different people, right? There was a dietician and counselling and more available, about 3, 4, 5 people there were helping me, but here she's the only one doing lots of stuff.’ (Participant 15 – woman, lay community health PN program) ‘There isn't anything like booking blood tests, booking scans, coming back from surgery, or getting staples removed ‐ anything that I needed could always be taken care of by them.’ (Participant 20 – man, nurse PN program) |
| Seamless Care |
‘Anytime I had appointments, usually with either the different types of doctors or nurses or whatever else, [the navigator] would usually join along. She would listen to it and then afterwards… [would be] able to have that buffer… to put it into words of rather than just like, “Okay, here's the meds,” but “This is why you're taking it. Here's what it's for.”’ (Participant 2 – man, nurse PN program) ‘Any questions that we have or for the oncologist, instead of calling the oncologist's office and having to go through all that, [the navigator would] email them directly and the responses, fortunately, to them are much quicker and then [the navigator] can translate everything. Whereas if we call the office ourselves, there's a little bit more of a lag… The nurse navigators are amazing at helping us to understand what's going on.’ (Participant 6 – man, nurse PN program) ‘She's filling a hole of being discharged from the hospital to your home when you open the door and there's nobody there.’ (Participant 13 – woman, nurse PN program) ‘The doctors, they're a big deal, but they're not there all the time like the navigators are. If I ever had any questions, it was never a problem. I always had their number and could give them a call if you need anything… If they didn't have it, they'd find it for me.’ (Participant 20 – man, nurse PN program) |
| Humanized Care |
‘The person is important to them – that we recognize we are important in this and how all of this impacts us as well… They ask us that if we have any concerns, that it's important to them and that they will help us with anything that we might have a concern about, and they make that clear, and I find that very different from other avenues of medical care.’ (Participant 5 – man, nurse PN program) ‘They're treating you like you are a person, not just a number or just a patient, but you are a person… It's not too often that people get to take the time to get to know you… and so being able to talk to [the one navigator] about Halloween and to talk to [the other] about her [family] for a few minutes, it's nice. You could just have that conversation sort of thing.’ (Participant 8 – woman, nurse PN program) ‘She listened versus lectured.’ (Participant 13 – woman, nurse PN program) ‘It's not like therapy, but it is like a conversation and that's so refreshing.’ (Participant 17 – woman, lay community health PN program) ‘Everybody is treated, and they know everybody, and they know who they are. I've seen people come in and it is like there is a cloud over the top of your head sometimes, and you go in there and they can make the sunshine a little bit.’ (Participant 20 – man, nurse PN program) |
| Themes | Quotes |
|---|---|
| Accessibility |
‘I just want to say they are also really good because they are open outside of the days that they do chemo, and there were several occasions that I just popped into the office because I had questions.’ (Participant 7 – woman, nurse PN program) ‘If I ever had a small question or a concern, I would email her, and it'd be like an instant reply.’ (Participant 12 – woman, social work PN program) ‘When I was at the hotel for two months for any medical appointment, I always had a navigator with me, helping me through the appointment, which made it so much easier for me and it was a very positive experience.’ (Participant 21 – Interpreted – man, lay community health PN program) ‘The [navigators'] phone line is always open and they're like that with everybody. They tell everybody, ‘If you need anything, don't be scared to call’… They have got time for everybody all the time.’ (Participant 20 – man, nurse PN program) |
| Approachability |
‘They're very bubbly and personable and I feel like I can discuss anything with them. If I have a sore throat or even not medical, say, well, you look like you're upset today, what's going on? Or whatever. And you feel like you can talk to them about anything.’ (Participant 1 – woman, nurse PN program) ‘What do I value most? The easiness it was and how she made you feel comfortable asking a question. Somebody else might think it's the stupidest question, so why ask it? You should know the answer. But she never once laughed at my silly question or even my husband's silly question. She answered it truthfully. And I'd like to say with respect to our ignorance on some of these things that we were going through.’ (Participant 4 – woman, nurse PN program) ‘For somebody like myself having… to actually reach out to my [doctor], I mean, I don't know what the actual process is, but I feel like they're busy enough. I don't want to burden them with phone calls, with questions or concerns that I have if I'm having some kind of symptoms or whatever. It was just so much easier to reach out to the nurse navigator, even if she ultimately ended up contacting my oncologist. It was just, for me, it was the comfort of that.’ (Participant 7 – woman, nurse PN program) ‘I thought it would be more the very structured social worker… I was wary of saying anything too personal in the beginning because I just didn't want things written on my record as per what social work would have to. So, being more informal has really, I've loosened up quite a lot and I feel a little more open now and a little more like, “Okay, there is help in the healthcare system.”’ (Participant 17 – woman, lay community health PN program) |
| Systems Knowledge |
‘They're very knowledgeable and very helpful, and they're always there. It seems like they're always there to answer questions.’ (Participant 6 – man, nurse PN program) ‘The biggest thing for me is if I ask a question and someone doesn't have an answer if they go and search for the answer, that makes them higher up in my books, I guess. And she was always like that. If I asked something completely out of the blue, she would be like, “I don't know, but let me get back to you,” and she would always give me an answer no matter what the question was, even if it wasn't related to me [my condition], if it was kind of off topic about me just becoming an adult, she was going to answer the question even if she didn't have an answer, she would figure it out for me.’ (Participant 12 – woman, social work PN program) ‘Sometimes I don't know the system, but I can learn from [the navigator] what are the new things that they can offer. So, whatever they offer me, I can use it.’ (Participant 15 – woman, lay community health PN program) ‘She's very empathetic and has a wealth of knowledge and a lot of, I think, personal experience, which goes a long way… She knows a lot about a lot of things, so if I bring something up that I'm interested in, she's either heard about it or is involved with it in some way.’ (Participant 17 – woman, lay community health PN program) |
- —This study was supported by the Canadian Institutes of Health Research.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Global Cancer Incidence and Screening · Primary Care and Health Outcomes
Introduction
1
Patient navigation (PN) was first envisioned in 1990 as a complex health intervention to support patients facing disproportionate barriers to timely breast cancer treatment in Harlem, New York [1]. In the inaugural PN program, lay (i.e., non‐clinically trained) navigators were tasked with supporting patients following the receipt of a suspicious breast cancer screening finding by working to address financial, informational, logistical, emotional or other barriers to care until the point of diagnostic resolution was achieved [2, 3, 4]. Following program implementation, early breast cancer detection at stages 0‐1 in the Harlem Hospital increased from 6% to 41% and 5‐year survival rose from 39% to 70% [5].
Recognizing the implications of PN, international interest in the intervention has led to widespread uptake and clinical expansion of PN programming beyond the confines of cancer treatment [6], with programs emerging in areas of chronic disease management [7, 8, 9], mental health [10], emergency care [11, 12], primary care [13] and paediatric‐to‐adult care transitions [14, 15, 16]. This broadening in PN scope has also led to the appointment of navigators with different training backgrounds (e.g., nurses, social workers, pharmacists and peer navigators) [17, 18]. While the adaptability of PN programs to different patient contexts and needs is critical, as is the case with any complex health intervention, there ought to remain some irreducible elements of PN that are visible across all programs [19, 20]. It appears, however, that as literature on PN proliferates, these elements have become increasingly difficult to pinpoint [21]. For example, it seems unlikely that a program consisting of lay navigators who link patients struggling with poor mental health to community‐based health and social services would have much conceptual overlap with another program composed of oral oncology nurse navigators who work to support symptom management and patient adherence during chemotherapy treatments [10, 22]. Such a lack of consensus surrounding PN conceptualization poses issues for effective program development and capacity building (e.g., navigator training) [23]. Furthermore, without a universal understanding of PN and navigator roles, researchers and policymakers face significant challenges when attempting to evaluate, replicate and/or scale such interventions [24].
It remains unclear how such program heterogeneity has impacted patients' experiences with and understandings of PN. Prior studies examining patients' experiences with program‐ or condition‐specific PN services have proposed overarching navigator functions related to the provision of comprehensive care [16, 25, 26, 27, 28, 29], explaining pertinent clinical information [12, 16, 25, 26, 28, 30, 31, 32], improving patient self‐efficacy [12, 16, 25, 26, 29, 31, 33], mitigating health‐related social needs (e.g., food access, transportation, housing, caregiver responsibilities) [12, 16, 25, 29, 33], bridging structural gaps in patient care [12, 16, 25, 27, 28, 29, 30, 31, 32, 33], scheduling medical appointments [12, 16, 25, 31, 33] and cultivating strong client‐navigator relationships [12, 16, 25, 26, 27, 28, 29, 30, 31, 32, 33]. While this study provides insightful context‐specific information, the integration of patient perspectives across distinct PN programs is needed to develop a more global understanding of PN [34, 35].
This qualitative study, therefore, sought to explore patients' understanding of distinct PN programs to identify shared PN functions and characteristics felt to be of particular value and importance to patients. Recognizing that PN programs constitute complex interventions where context‐level adaptations are critical to their success, the focus of this study was not per se on what individual programs did but on how they affected care recipients [36]. As such, utilizing patient experiences with PN served as an essential medium through which to address the study's aim.
Materials and Methods
2
Interpretive description (ID) was used as the methodological approach for this study [37]. ID is a qualitative research methodology designed to generate practical, contextually grounded knowledge relevant to applied health disciplines [38]. Its flexible and non‐prescriptive nature allows researchers to critically engage with disciplinary logic, selecting approaches that align best with their research question and support meaningful applications in real‐world settings [38, 39]. To do so, ID necessitates inductive approaches to data analysis that are concurrent with data collection, ensuring that all study findings are developed within the context of the data itself [38].
Employing ID, this study sought to distill a common understanding of the essential functions and characteristics of PN, while not assuming that the findings generated would be comprehensive of all patient experiences with PN. Throughout the study, particular interest was given to ensuring that the research process was guided by a clear and consistent approach to knowledge, that patients' experiences with PN were accurately represented, that data analysis was logical and transparent, and that our interpretations were well‐supported and trustworthy [38, 40]. The promotion of representative credibility and analytic logic in this project was achieved through maximum variation sampling (see Study Participants section below) and the construction of an audit trail, respectively. Interpretive authority was also bolstered through the use of thick description (that which goes beyond superficial accounts of participant responses to explore their underlying context or meaning) and the input of patient partners, who provided a mechanism to check for interpretation accuracy [41].
Patient Engagement Strategy
2.1
Recognizing the importance and need for patient‐oriented health research, the research team incorporated the perspectives of two dedicated patient partners (EB, LW) who served as co‐investigators in the study. Monthly meetings were held with the patient partners throughout the study to ensure our methodologies and questions aligned with the interests of patients in the province. In these meetings, the patient partners helped codevelop the interview guide and drove priority setting [42]. They also provided critical feedback on a range of other research activities, including the generation of the codebook and final themes, manuscript revisions and knowledge translation efforts.
Study Participants
2.2
Patients (or ‘clients’, as recipients of PN programs may alternatively be referred) were recruited from active Albertan PN programs. Maximum variation purposive sampling was performed to recruit a diverse participant sample across three strata (i.e., gender, socioeconomic status and navigation type), selected for their foreseeable implications on PN programming and service reliance [43, 44, 45]. In an effort to learn from patients with differing PN experiences, no restrictions were placed on the clinical scope of navigation services offered by PN programs or the training of their navigators. PN programs were excluded from the study if they were not patient‐facing (i.e., only offered referral‐based services) or if they were privately operated. Additionally, we did not include PN programs that specifically served Indigenous communities, recognizing the distinct roles these programs serve in addressing the historical and ongoing impacts of colonialism in Western healthcare systems [46]. The cultural significance of Indigenous PN programs could not be adequately explored within the scope of this current study, especially without Indigenous voices on our study team [47]. Instead, a separate study, partnered with Indigenous community members, is needed to highlight the unique cultural considerations of these programs.
Tang et al.'s [48] environmental scan of PN programs in the province provided a working list of potential recruitment sources that were further verified and expanded through a secondary search using publicly available program websites, an Alberta Health Services directory (https://www.albertahealthservices.ca/findhealth/), and snowball sampling. All PN programs identified through the secondary search were contacted for additional information on the types of services offered. PN programs that failed to respond to repeated contact attempts were excluded from the study. Of the 58 PN programs identified in the province‐wide environmental scan, only five met the study's inclusion criteria due to incompatibility with the programs' scope (e.g., did not have a clearly outlined ‘navigator’ position) and/or target population (e.g., did not work with adult patients) [48]. Patient experiences from two of the eligible programs were captured in the study alongside other, more recently established, PN programs. PN program directors and navigators of identified PN interventions acted as key informants, helping to identify and recruit study participants. Adult patients who had participated in an Alberta‐based ‘navigation’ program within the past 2 years for at least 1 month were eligible.
Ethics approval for the study was obtained by the University of Calgary's Conjoint Health Research Ethics Board.
Data Collection
2.3
The interview guide (Table S1) was co‐developed with patient partners and grounded in the socio‐ecological model, recognizing that one's interactions with PN programs may be closely linked to their social positioning and various sources of influence [49]. Virtual and in‐person interviews were conducted from November 2023 to February 2024, each lasting up to 1 h, with an average duration of approximately 50 min. For participants with limited English literacy, trained interpreters were utilized to help facilitate interviews. All interviews were conducted by one of two team members (S.R. [female graduate student] and/or K.T. [female clinician researcher]) who were unfamiliar with the study participants, and who both had prior qualitative research experience and training. Audio files for each interview were transcribed verbatim using Rev audio transcription services (rev. com) and reviewed by a study team member (SR) to ensure transcript accuracy [50]. All participant files were given a unique alphanumeric study ID.
Data Analysis
2.4
Participant recruitment, data collection and data analysis were undertaken concurrently until sufficient information power was achieved [51, 52, 53]. Inductive thematic analysis was selected as the analytic approach for this study and performed using NVivo software [54, 55]. Given ID's non‐prescriptive nature, the study team recognizes that a variety of qualitative research approaches could have been employed to identify meaningful patterns in the data set [38]. Our choice to use thematic analysis was rooted in our objective to go beyond simple descriptions of PN (i.e., purely exploring its semantic meaning) to examine patients' perspectives and understanding of the conceptual meaning of PN [54]. Braun and Clark have published a typology of research questions that are well suited to be examined and explored through a thematic analysis approach; one such type encompasses questions related to ‘the views, perceptions, understandings, perspectives, needs, motivations of particular groups, about particular phenomena, in particular contexts’ [56]. Thematic analysis is, therefore, an approach that we believe aligns well with our research question and objective, as well as our intention to code for both semantic and latent meanings from the data collected. Furthermore, the use of inductive thematic analysis enabled us to generate data‐derived thematic outputs that evolved organically throughout the coding process [56]. Two team members (K.T., S.R. and/or S.B. [female health services researcher]) independently generated initial codes for each transcript. The team met regularly to develop and refine a consolidated coding tree (Figure S1) and set of themes. Following theme generation, additional analyses were performed to ensure the study findings were appropriately interpreted and could directly inform PN program implementation [57, 58]. Through reflexive conversations with patient partners, a unified schema was co‐built that more harmoniously distilled the essence of PN in the province. Participants were not asked to provide feedback on the study findings.
Throughout the research process, researchers utilized reflexive journaling, wrote post‐interview field notes and debriefed with peers to limit the effects of researcher bias and subjectivity [59]. An audit trail was also created, keeping a systematic record of memos to document the evolution and interpretation of themes [60].
Results
3
Twenty‐three participants were included in the study (Table 1). The median (IQR) age of participants was 59 (48–67) years, with 12 participants (52%) self‐identifying as women and 17 (74%) identifying as white. Participants worked with a nurse (48%), lay (39%) or social work (13%) navigator for a median (IQR) duration of 7 (3–24) months. Three study participants were non‐English speaking and required the assistance of an interpreter.
The study participants received services from five distinct PN programs across Alberta. One program was specifically designed for patients receiving chemotherapy, offering referral support and medical care provision (n = 8). Two other programs were designed to support transitions of care – one for transitioning from paediatric to adult care (n = 3) and the other from hospital to home (n = 3). The last two programs were based in the community – one in primary care (n = 6) and the other in a community organization that assists individuals who have recently immigrated to Canada (n = 3). All programs offered primarily in‐person services, with opportunities for over‐the‐phone correspondence based on participant preference. Participant perceptions of essential PN functions were not found to differ between navigator training backgrounds.
Six themes were generated that captured participant‐identified functions of PN, as well as the characteristics of PN that were felt to be of particular value and importance in facilitating these functions (Figure 1). Illustrative quotes for function‐ and characteristic‐specific themes are provided in Tables 2 and 3, respectively.
Visual Depiction of Participants' Understanding of PN Functions and Characteristics. Participants' understandings of PN were largely categorized into three function‐based themes surrounding the facilitation of personalized care, the mitigation of system‐level care gaps and the provision of humanized care. These three navigator functions were made possible by three characteristic‐based themes pertaining to navigator accessibility, approachability and systems knowledge. Irrespective of navigator training or navigation setting, the participants' experiences suggest that the programs were further unified in their pursuit of improving perceived patient care.
Themes Relating to the Function(s) of Navigators Within the Healthcare System
3.1
Navigators facilitate personalized care by identifying, addressing and prioritizing the diverse needs of patients
3.1.1
Participants spoke of their navigators' ability to centre the patient and their distinct care needs in service interactions. By allowing patients greater control over their communication and respecting their care preferences, participants felt the navigators were better able to tailor their support to specific patient needs: ‘They seem to make you the centre… they're making sure that you are being looked after’ (Participant 8 – woman, nurse PN program). The prioritization of patients' particular care needs also meant that navigators would often serve multiple different care roles, offering clinical, emotional, social and physical support, if pertinent, to their patients: ‘There's nothing I've asked that they weren't able to help me with… there's nothing that they haven't been able to accommodate’ (PID 9 – woman, nurse PN program).
The consistent willingness of the navigators to provide individualized care was exemplified by one participant who recalled receiving multiple different modes of support from her navigator, including guidance on obtaining her driver's license, assistance with university applications and coaching on how to strengthen their clinician communication skills ‐ all things that the participant identified as critical to supporting their independence. Alternatively, another participant described how their navigator provided medical guidance (i.e., advice on when to discontinue certain medications) and emotional reassurance, as well as liaised with their oncologist, assisted with the scheduling of blood tests and imaging and helped remove their surgical staples. The adaptability of navigators was contrasted by participant retellings of other healthcare professional interactions, described by some as feling excessively rigid or ‘pigeonholed’ (Participant 2 – male, nurse PN program).
Navigators facilitate seamless care by addressing system‐level care gaps in the healthcare system
3.1.2
Participants described the ability of their navigators to help mitigate informational and structural gaps they were experiencing in their care. These gaps pertained specifically to limited provider availability, insufficient appointment lengths and suboptimal patient‐provider and interprofessional communication: ‘There's a lot of stuff that you are kind of just expected to know… [the navigators are] making sure the foundation is there… and filling in any gaps’ (Participant 11 – man, social work PN program).
As a result of these care gaps, patients described feeling overwhelmed by an ‘avalanche of information’ (Participant 6 – man, nurse PN program). Patients highlighted the role of navigators in translating and/or delivering information to make it more digestible for patients: ‘[The navigators] were able to kind of talk you off the ledge and explain to you what's going on…, and who's going to help you, and what you need, and the resources… It's like they're in your corner right from the beginning’ (Participant 20 – man, nurse PN program).
Navigators facilitate humanized care through displays of empathy and warmth
3.1.3
Patients frequently highlighted the importance of empathy and compassion in the navigation process. They discussed the strength and depth of the relationships they were able to cultivate with their navigators, describing their navigators as feeling akin to their friends and family: ‘Beyond the expert care that they're trained to do, it's their input in such a friendly, genuine interaction with you. It doesn't sound clinical. It sounds like you're sitting in a living room having your treatment with people who genuinely want to know more about you’ (Participant 5 – man, nurse PN program).
While such humanistic care provision manifested differently for each patient (e.g., offering physical comforts, personal conversations, or words of encouragement), its presence in PN programs consistently allowed the participants to feel regarded as more than their disease or illness. For many, the empathy and compassion of the navigators emboldened participants and steeled their resilience: ‘It's almost like the light in the tunnel, and it gives you that self‐assurance and it kind of keeps you on that path [to recovery]’ (Participant 2 – male, nurse PN program).
Themes Relating to Navigator Characteristics That Facilitated Their Ability to Provide Personalized, Seamless and/or Humanized Care
3.2
Patients value accessibility, where navigators are available and flexible to their needs
3.2.1
Participants frequently spoke of their appreciation for how navigators made themselves available to patients in times of need, which were often outside of regular business hours: ‘Because of my condition, sometimes I needed to go to the hospital in the middle of the night and they were able to accommodate me… I value that thing a lot. The flexibility and the understanding and the empathy’ (Participant 22 – Interpreted – man, lay community health PN program). Knowing the participants had a go‐to person with whom they could always contact provided considerable reassurance and security: ‘One of the main things was just having somebody there who I could reach out to… I found that [with the navigator] being around, if I had any questions or thoughts, I could dump them on her and she would get the answer for me… I remember lying in the bed in the hospital thinking… ‘Oh my God,’ this time I didn't really have to worry about [my care] because all of a sudden there was this person who was going to help me’ (Participant 3 – man, nurse PN program).
Patients value approachability, where navigators could connect with patients free of clinically imposed hierarchies
3.2.2
Participants appreciated the ability of navigators to create spaces where they felt at ease and could speak freely. Navigators were felt to be approachable: ‘[The navigator] was bubbly and friendly. Now I think if someone else came in and they were more ‘just the facts, ma'am, just the facts’ … I think it would have been hard to open up… It wasn't like I was anxious about her visits to come or anything… it just made it a lot easier.’ (Participant 16 – woman, lay community health PN program). Some patients juxtaposed the approachability and comfort they felt with their navigators with their hesitation to speak with their usual clinical care providers: ‘You could go to your doctor and ask these questions, but you're going to be heart racing the whole time because obviously, they have so many other patients… [The navigator] was able to do it and [you] know that if you're going to ask this question, no one's going to ridicule you’ (Participant 12 – woman, social work PN program).
Patients value having a navigator with extensive systems knowledge
3.2.3
All participants referred to their navigators as rich sources of system information. Participants explained the value of having someone with extensive hospital‐ and/or community‐based information who could allocate the time needed to address patient questions effectively: ‘As soon as I talked to the nurse navigator, she was giving information, stuff that I didn't have yet, stuff that I needed, stuff that I wanted. That's what I was looking for’ (Participant 7 – woman, nurse PN program). For the participants, having greater access to information increased their ability to utilize the supports around them and, in doing so, bestowed them with greater autonomy to make informed decisions about their health: ‘Having the navigator has been so supremely helpful because it's getting the ideas for alternative services that people, like myself, did not know were out there… I feel better knowing that there is an alternative to the static healthcare system that we're used to’ (Participant 17 – woman, lay community health PN program).
Discussion
4
Our study found that, from the patient's perspective, PN consistently offers care that is personalized, seamless and humanized. These PN functions are made possible by the accessibility, approachability and extensive systems knowledge of the navigators themselves. Though the operationalization of these themes varied in response to distinct care settings and participant needs, the essence of navigator functions and characteristics was consistent across interviews.
The expansion and diversification of PN over the past three decades have sparked numerous efforts to identify and synthesize commonalities across contemporary PN programs. In one such project, Champ and Dixon [61] provide an extensive summary of oncology PN programs across Canada, noting that, while similarities exist regarding programs' methods of service delivery (e.g., the incorporation of virtual care in most models) and targeted age ranges (e.g., primarily adult patients), considerable variation was found in their patient demographics, navigator training, scope of practice and patient referral processes. Similarly, a mixed‐methods study examining Cancer Care Alberta's PN programs showed that, despite the evolution and prevalence of PN programs, gaps relating to navigator role ambiguity continue to cause inconsistencies in program delivery [62]. These studies, together with a recent proceedings paper by the Canadian Healthcare Navigation Conference, underscore the continued lack of clarity surrounding PN, including how PN services differ from the roles and supports provided by other members of the healthcare team [63]. The lack of role and conceptual clarity surrounding PN continues to pose significant barriers to the uptake, implementation and appreciation of PN programs today [64, 65, 66]. In response, Canadian stakeholders have called for greater PN standardization, recognizing that the current lack of a shared vision for navigation programs limits the positive impact that PN programs can have [63].
To address this lack of clarity, multiple reviews of PN have been conducted in different PN care fields (i.e., oncology, dementia and mental health and addiction) to better understand not only the operations and characteristics of PN but also their functions and core themes [66, 67, 68]. Although these reviews identified similar PN functions, specifically as they relate to care coordination and relationship building, their interpretations of these thematic concepts varied. For instance, the notion of ‘care coordination’ was described by Katerenchuk and Salas [68] to mean supporting all patient health needs, disseminating medical and nonmedical information, and remaining available throughout their care journey. In contrast, Anthonisen et al. [66] described ‘care coordination’ more literally as navigators facilitating patient access to pertinent services and resources. Relationship‐building was also interpreted differently across these reviews, especially with regard to the depth, extent and purpose of the relationships formed. For example, Mullen et al. [67] promoted the use of navigational teams (i.e., navigators working collaboratively to support patient needs) while others advocated for one‐on‐one patient‐navigator relationships, describing the importance of relationship consistency in counteracting patients' other, often fragmented, connections to clinical support [68]. While these reviews offer a more comprehensive understanding of PN than program‐specific studies, the nuanced differences in their findings and their positioning in specific clinical contexts make it difficult to deduce what PN functions are cross‐contextual and therefore potentially fundamental to the PN construct itself. Although this qualitative study does not, and cannot, aim to definitively identify these fundamental components of the broader PN construct, it does elucidate elements of the intervention that patients feel are of critical importance.
Our study builds upon the findings of these PN studies by integrating patient perspectives across operationally and contextually distinct PN programs. While care coordination was repeatedly identified as an important PN function in prior reviews, our findings suggest that navigator functions extend beyond traditional ‘coordination’ (i.e., connecting patients across care providers, systems and services) to the creation of seamless care experiences more broadly for patients. ‘Seamless care’ is characterized by navigators working to fill gaps in patient care (e.g., patients referred to the ability of their navigators to address gaps related to the use of medical jargon, inefficient access to the broader medical team and abrupt hospital discharges), which resulted in reduced patient stress and increased feelings of comfort in their care. Therefore, while seamless care certainly incorporates aspects of traditional care coordination, this theme encompasses a broader component of PN that better resonates with patients' understanding of PN. As was also seen in prior reviews, our findings highlight the importance of relationship‐building between the navigator and the patient. With that said, we note that study participants from different PN programs often described different manifestations of the patient‐navigator relationship. For example, some described a deep connection with the navigator and valued the emotional support provided, while others valued the relational aspects of PN, even without this depth of relationship. Regardless of how the patient‐navigator relationship was operationalized across programs, its perceived value and importance was rooted in its ability to make the patient feel regarded as more than their illness. We therefore broaden the idea of relationship building to better address the provision of ‘humanized care’ as a PN function.
Taken together, the three PN functions identified in our study appear to collectively compensate for the existing systemic and structural holes in contemporary healthcare systems. The current stresses and fraying of our healthcare systems have made the time, resources and flexibility needed to provide personalized, seamless and humanized care by healthcare teams increasingly untenable [69]. In this study, participants consistently noted the importance of navigators in providing personalized care, in part, because of the difficulty they faced receiving such customization from other care providers. Similarly, the ubiquity with which participants spoke of their navigators' ability to create seamless care experiences was, at times, a direct response to their experiences with increasingly fragmented care pathways [70]. Overall, the commonalities in participant understandings of distinct PN programs suggest key points of overlap in PN that may be indicative of broader PN tenets. This study also highlights the value patients ascribe to PN as a means of patching system‐level problems that have led to such rigid and fragmented care experiences.
Strengths and Limitations
4.1
The study's use of maximum variation purposive sampling enabled the research team to collate experiences from patients of diverse backgrounds and distinct PN program interactions. The heterogeneity present across our participant sample strengthened the credibility of our findings, as well as permitted us to further examine the nuances of patient interactions with PN programs. Additionally, the involvement of our patient partners was crucial in anchoring our work and ensuring our findings resonated with both researchers and patients alike.
Limitations to this project include the possibility that, given our use of key informants in participant recruitment, those with negative PN experiences may have been dissuaded from participating or may have never been contacted. This has the potential to bias our findings to be overly positive, blurring elements of PN that may need modification for broader patient utilization or greater receptivity to the service. While such a bias may be present, it is worth reiterating that the purpose of this study was not to explore patients' satisfaction with PN services, nor to evaluate their effectiveness, but to identify the key functions and characteristics of these programs, should they exist. Additionally, while the participant sample generally displayed a high degree of heterogeneity, it was relatively homogenous in terms of participants' race and ethnicity, with nearly 75% of the sample self‐identifying as white. Moving forward, greater participant diversity should be sought with respect to participant race or ethnicity to provide greater insight into the culturally tailored possibilities of PN. Lastly, several types of PN programs were not included in this project. While this study provides insight on how a subset of patients conceptualize PN programs, future research that explores patient experiences with programs specializing in different care domains (e.g., dementia, mental health, HIV, or autism), with navigators of different training backgrounds (e.g., pharmacists or peer navigators), or with Indigenous‐specific PN programs may elucidate additional navigator functions and/or characteristics not directly captured in this study. Furthermore, because PN programs for this study were primarily identified via publicly available program websites and an Alberta Health Services directory, we likely missed programs that were either (i) not funded, administered, or delivered by Alberta Health Services, or (ii) did not have websites for the public (e.g., smaller programs or those that did not permit self‐referrals). The limited number of PN programs that were ultimately represented may indicate that there are additional PN functions and characteristics beyond those captured in this study, or that further nuances may need to be considered for the functions that were identified. Although an exhaustive overview of patients' understanding of PN was never the intent of this study, this does likely restrict the transferability of our findings.
Conclusion
5
This study extends current knowledge about the commonalities that exist across distinct PN programs, from the patient's perspective. The findings indicate
that patients repeatedly understand PN services as those which offer personalized, seamless and humanized care; and that they deeply value navigators' accessibility, approachability and extensive systems knowledge. This study suggests that, despite increasing heterogeneity in how PN programs are designed and operationalized, key irreducible functions and characteristics of PN continue to persist across contemporary programs.
Author Contributions
Sarah Rabi: conceptualization, project administration, methodology, investigation, validation, data curation, formal analysis, visualization, writing – Original draft. Maria Santana: supervision, conceptualization, methodology, investigation, writing – reviewing and editing. Gina Dimitropoulos: supervision, conceptualization, methodology, writing – reviewing and editing. Kerry McBrien: supervision, conceptualization, methodology, writing – reviewing and editing. Eleanor Benterud: methodology, investigation, formal analysis, visualization, writing – reviewing and editing. Lorraine Wigston: methodology, investigation, formal analysis, visualization, writing – reviewing and editing. Karen Tang: funding acquisition, supervision, conceptualization, project administration, methodology, investigation, validation, formal analysis, visualization, writing – reviewing and editing.
Ethics Statement
Ethics approval for the study was obtained by the University of Calgary's Conjoint Health Research Ethics Board.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
PN_Patient_Experiences_Supplement_Revised.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. P. Freeman , B. J. Muth , and J. F. Kerner , “Expanding Access to Cancer Screening and Clinical Follow‐Up Among the Medically Underserved,” Cancer Practice 3, no. 1 (1995): 19–30.7704057 · pubmed ↗
- 2H. P. Freeman , “A Model Patient Navigation Program,” Oncology Issues 19, no. 5 (2004): 44–46, 10.1080/10463356.2004.11884227. · doi ↗
- 3H. P. Freeman and R. L. Rodriguez , “History and Principles of Patient Navigation,” Cancer 117, no. 15 0 (2011): 3539–3542, 10.1002/cncr.26262.21780088 PMC 4557777 · doi ↗ · pubmed ↗
- 4H. P. Freeman , “Patient Navigation: A Community Based Strategy to Reduce Cancer Disparities,” Journal of Urban Health 83, no. 2 (2006): 139–141, 10.1007/s 11524-006-9030-0.16736361 PMC 2527166 · doi ↗ · pubmed ↗
- 5S. F. Oluwole , A. O. Ali , A. Adu , et al., “Impact of a Cancer Screening Program on Breast Cancer Stage at Diagnosis in a Medically Underserved Urban Community,” Journal of the American College of Surgeons 196, no. 2 (2003): 180–188, 10.1016/S 1072-7515(02)01765-9.12595043 · doi ↗ · pubmed ↗
- 6V. A. Parker , J. A. Clark , J. Leyson , et al., “Patient Navigation: Development of a Protocol for Describing What Navigators Do,” Health Services Research 45, no. 2 (2010): 514–531, 10.1111/j.1475-6773.2009.01079.x.20132342 PMC 2838158 · doi ↗ · pubmed ↗
- 7K. A. Mc Brien , N. Ivers , L. Barnieh , et al., “Patient Navigators for People With Chronic Disease: A Systematic Review,” P Lo S One 13, no. 2 (2018): e 0191980, 10.1371/journal.pone.0191980.29462179 PMC 5819768 · doi ↗ · pubmed ↗
- 8I. V. Bassett , S. M. Coleman , J. Giddy , et al., “Sizanani: A Randomized Trial of Health System Navigators to Improve Linkage to HIV and TB Care in South Africa,” JAIDS Journal of Acquired Immune Deficiency Syndromes 73, no. 2 (2016): 154–160, 10.1097/QAI.0000000000001025.27632145 PMC 5026386 · doi ↗ · pubmed ↗