Prognostic value of sarcopenia in aortic valve replacement: a systematic review and meta-analysis
Jie He

TL;DR
This study finds that sarcopenia is common in patients undergoing aortic valve replacement and is linked to higher long-term mortality.
Contribution
The study provides a systematic review and meta-analysis on sarcopenia's prognostic value in aortic valve replacement patients.
Findings
Sarcopenia prevalence was 31.3% in SAVR patients and 43.7% in TAVR patients.
Sarcopenia was associated with higher long-term mortality in both SAVR and TAVR patients.
The association remained consistent across different diagnostic criteria and ethnic groups.
Abstract
This study aimed to quantify the prevalence of sarcopenia in patients undergoing surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR), and to assess its association with mortality risk. Relevant studies were identified through searches of the PubMed, Cochrane Library, Excerpta Medica Database (Embase), Web of Science, and China National Knowledge Infrastructure (CNKI) from inception through July 1, 2025. The prevalence of sarcopenia and its 95% confidence interval (CI) were calculated, with heterogeneity evaluated using the I2 statistic. The link between sarcopenia and mortality following SAVR/TAVR was quantified by hazard ratio (HR) or odds ratio (OR) with 95% CI. Statistical analyses were conducted using Stata 11.0. Thirty-eight studies were included, with 6 focusing on patients undergoing SAVR and 32 on those undergoing TAVR. Sarcopenia was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
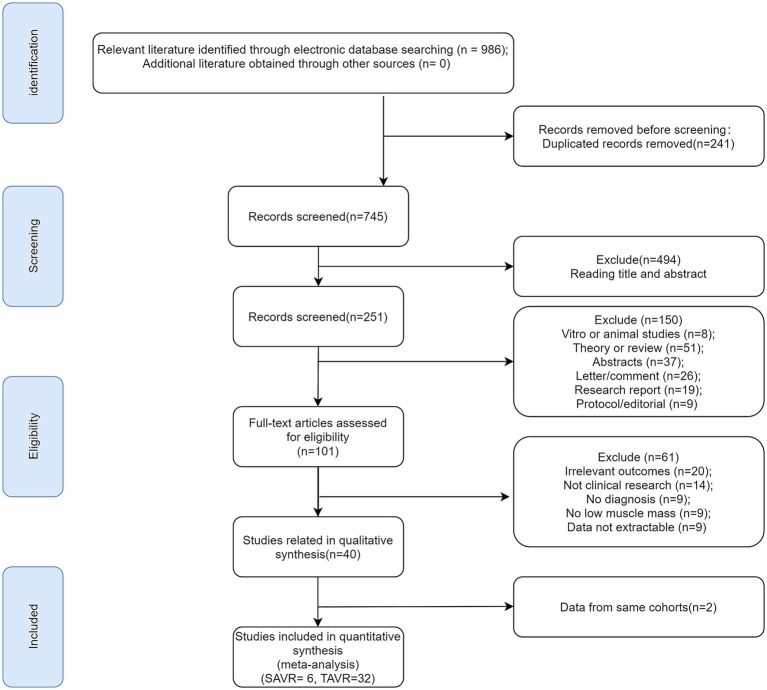 Figure 1
Figure 1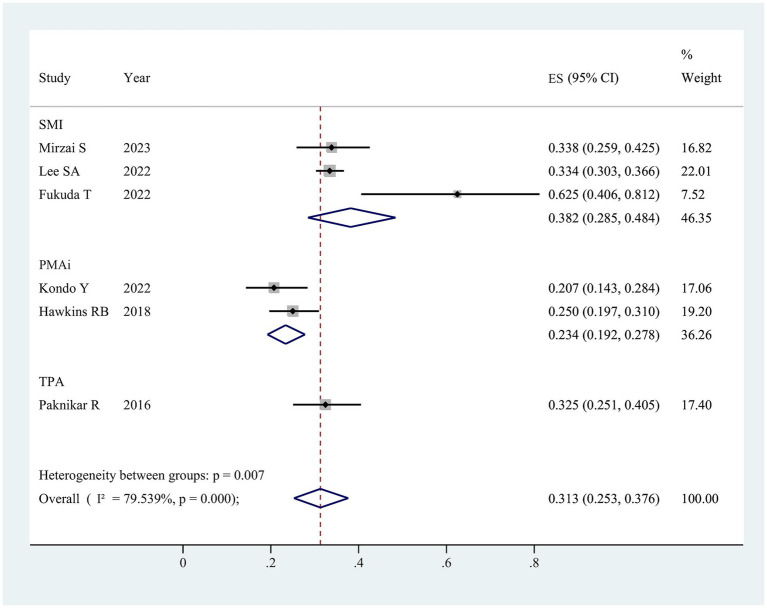 Figure 2
Figure 2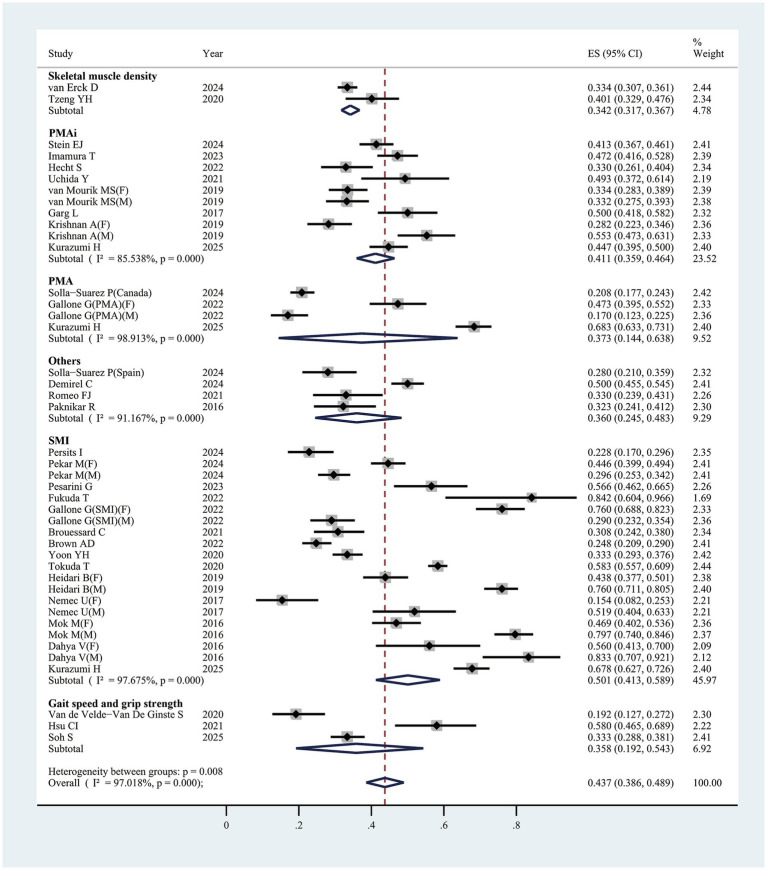 Figure 3
Figure 3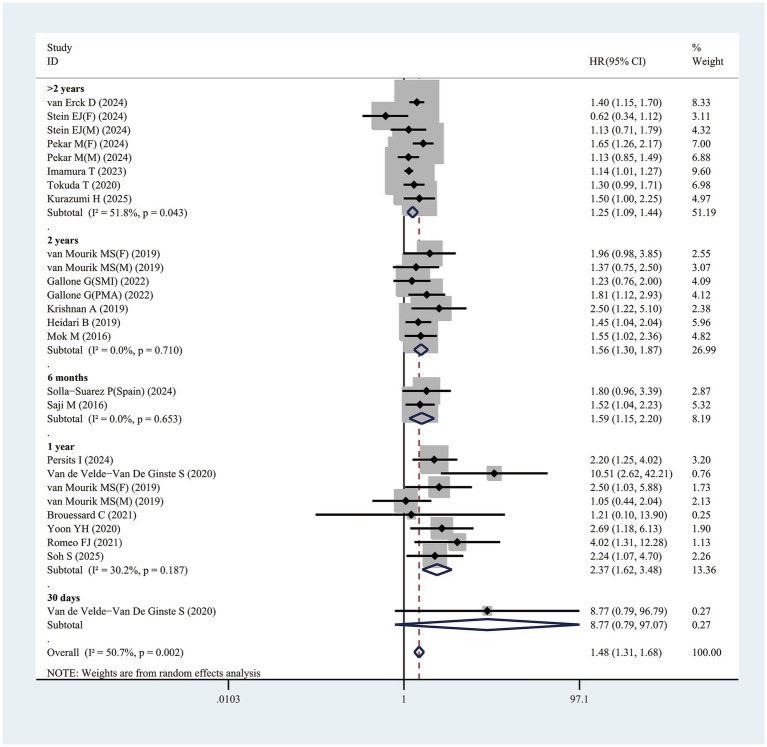 Figure 4
Figure 4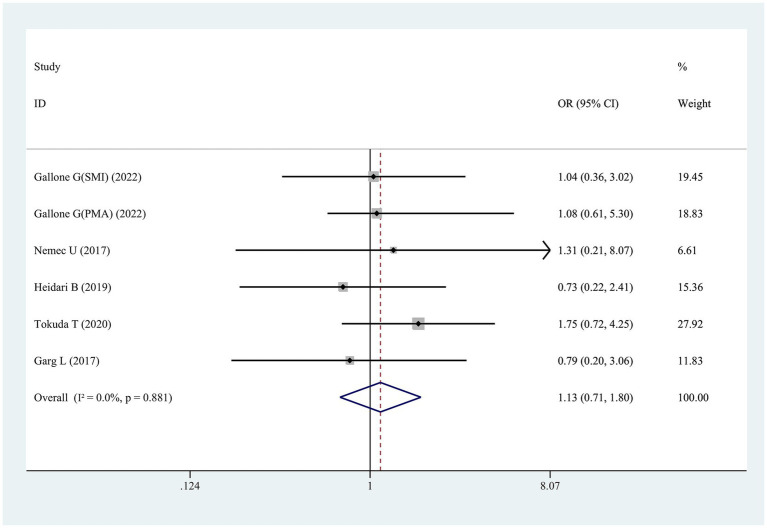 Figure 5
Figure 5| Study, year | Country | Study design | Study type | Mean/median age (years) | BMI (kg/m2) | STS score | Assessment of sarcopenia | Definition of sarcopenia | Prevalence of sarcopenia ( | Study quality | Main outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| van Erck et al. (2024) ( | Netherlands | Retrospective | CS | 80.0 ± 7.0 | 27.1 ± 5.0 | NA | CT: L3-SMD | L3-SMD <10.7 HU in men, <1.2 HU in women | 400 | 1,199 | 7 | B, D |
| Stein et al. (2024) ( | USA | Prospective | CS | 82.9 (76.8–87.4) | 27.3 (24.1–31.6) | 3.66 (2.53–5.39) | CT: L4-PMAi | L4-PMAi <7.5 cm2/m2 in men, <5.2 cm2/m2 in women | 184 | 445 | 8 | B, D |
| Solla-Suarez et al. (2024) ( | Spain | Prospective | CS | 84.8 ± 5.3 | 24.5 ± 3.5 | NA | CT: L4-PMA | L4-PMA <22 cm2 in men, <12 cm2 in women | 126 | 605 | 8 | B, D |
| Solla-Suarez et al. (2024) ( | Spain | Prospective | CS | 83.4 ± 4.3 | 29.8 ± 4.4 | NA | Grip strength; Vscan extend handheld ultrasound system (Total muscle thickness) | Grip strength <27 kg in men, <16 kg in women; | 42 | 150 | 7 | B, D |
| Persits et al. (2024) ( | USA | Retrospective | CS | 80.6 ± 7.7 | 28.7 ± 5.8 | NA | CT: T9-T12-SMI | T9-T12-SMI <266.5 cm2/m2 in men, <182.1 cm2/m2 in women | 42 | 184 | 7 | B, D |
| Pekař et al. (2024) ( | Czech Republic | Retrospective | CS | 79.7 (74.9–83.3) | 28.9 (25.9–32.6) | NA | CT: L3-SMI | L3-SMI <42.44 cm2/m2 | 322 | 866 | 5 | B, D |
| Demirel et al. (2024) ( | Switzerland | Retrospective | CS | 82.8 ± 5.95 | 25.6 (22.7–29.7) | NA | CT: L3-nTMA | NA | 250 | 500 | 7 | B |
| Pesarini et al. (2023) ( | Italy | Prospective | CS | 81.6 ± 4.6 | 25.6 | 3.37 | CT: L3-SMI | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women | 56 | 99 | 6 | B |
| Imamura et al. (2023) ( | Japan | Retrospective | CS | 85.0 (83.0–88.0) | 21.7 (19.4–24.4) | 4.60 (3.9–6.1) | CT: L3-PMAi | L3-PMAi <10.7 × 10 cm3/m2 | 152 | 322 | 7 | B, D |
| Hecht et al. (2022) ( | Austria | Retrospective | CS | 83.03 ± 4.68 | 25.80 ± 4.19 | 3.19 ± 1.87 | CT: L3-PMAi | L3-PMAi ≤757.16 mm2/m2 in men, ≤569.88 mm2/m2 in women | 59 | 179 | 8 | B |
| Fukuda et al. (2022) ( | Japan | Prospective | CCS | 84.8 ± 3.6 | NA | NA | SMI, Grip strength, gait speed | Grip strength <18 kg or walking speed <1.0 m/s, and SMI < 5.7 kg/m2 only in females | 16 | 19 | 5 | A, B |
| Van de Velde-Van De Ginste et al. (2021) ( | Belgium | Retrospective | CS | 84.9 ± 5.3 | 25.7 ± 4.5 | 5.0 ± 3.1 | Gait speed and grip strength | Gait speed <0.8 m/s and | 24 | 125 | 8 | B, D |
| Uchida et al. (2021) ( | Japan | Prospective | CS | 85.0 ± 5.0 | 22.5 ± 3.3 | 6.0 ± 4.1 | PMAi | NA | 35 | 71 | 7 | B |
| Romeo et al. (2021) ( | Argentina | Retrospective | CS | 83.9 ± 5.7 | 27.2 ± 4.4 | 3.3 ± 1.7 | Sarcopenia index | SI ≤66 | 33 | 100 | 8 | B, D |
| Tzeng et al. (2020) ( | Taiwan | Retrospective | CS | 79.2 ± 7.8 | 23.9 ± 3.9 | 11.03 ± 3.9 | CT: L3-SMD | 10.4 HU | 73 | 182 | 8 | B |
| van Mourik et al. (2019) ( | Netherlands | Retrospective | CS | 82.6 | 27.1 | 4.6 | CT: L3-PMAi | 9.1 × 10 mm2/m2 | 192 | 576 | 7 | B, D |
| Garg et al. (2017) ( | USA | Retrospective | CS | 83.3 ± 6.5 | 28.1 ± 5.6 | 6.9 ± 3 | CT: L3-PMAi | L3-PMA <4.15 cm2/m2 in men, <3.47 cm2/m2 in women | 76 | 152 | 5 | B |
| Paknikar et al. (2016) ( | USA | Retrospective | CS | 80.0 ± 8.9 | 29.6 ± 7.1 | 6.5 ± 4.5 | CT: L4-TPA | NA | 40 | 124 | 7 | A, B |
| Gallone et al. (2022) ( | Italy | Retrospective | CS | 81.0 ± 6.0 | NA | 4.4 ± 3.6 | CT: L3-SMI, L3-PMA | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women; | SMI: 192; | 391 | 8 | B, D |
| Hsu et al. (2021) ( | Taiwan | Prospective | CCS | 78.16 ± 7.95 | 23.66 ± 3.75 | NA | Calf circumference, grip strength, and gait speed | Handgrip strength <27 kg in men, <16 kg in women, | 47 | 81 | 8 | B |
| Brouessard et al. (2021) ( | France | Retrospective | CS | 84 | 26.4 | NA | CT: L3-SMI; Gait speed | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women; | 56 | 182 | 7 | B, D |
| Brown et al. (2022) ( | Canada | Retrospective | CS | 80.7 ± 9.6 | 29.2 ± 13.8 | NA | CT: L3-SMI | L3-SMI <52.6 cm2/m2 in men, <40.9 cm2/m2 in women | 116 | 468 | 9 | B |
| Yoon et al. (2021) ( | Korea | Prospective | CS | 78.9 ± 5.2 | NA | 4.1 ± 3.0 | CT: L3-SMI | L3-SMI ≤38.9 cm2/m2 in women, ≤31.3 cm2/m2 in men | 174 | 522 | 7 | B, D |
| Tokuda et al. (2020) ( | Japan | Retrospective | CS | NA | NA | NA | CT: L3-SMI | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women | 802 | 1,375 | 7 | B, D |
| Krishnan et al. (2019) ( | USA | Retrospective | CS | 82.0 ± 8.0 | 27.9 ± 10.0 | 7.1 ± 5.5 | CT: L3-SMI, L4-PMAi | L3-SMI <50.0 cm2/m2 in men, <35.0 cm2/m2 in women; | 151 | 381 | 8 | B, D |
| Heidari et al. (2019) ( | USA | Retrospective | CS | 80.9 ± 8.9 | NA | NA | CT: L4-SMI | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women | 374 | 602 | 8 | B, D |
| Nemec et al. (2017) ( | USA | Retrospective | CS | 82.3 ± 10.0 | 27.3 ± 6.1 | 7.1 ± 5.3 | CT: L3, Th7 and Th12-SMI | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women; | 53 | 157 | 7 | B |
| Mok et al. (2016) ( | Canada | Prospective | CS | 80.0 ± 8.0 | 26.8 ± 5.8 | 6.9 ± 3.9 | CT: L3-SMI | L3-SMI <55.4 cm2/m2 in men, <38.9 cm2/m2 in women | 293 | 460 | 8 | B, D |
| Dahya et al. (2016) ( | USA | Prospective | CS | 81.0 ± 10.0 | 28.0 ± 5.0 | NA | CT: L3-SMI | L3-SMI <55.0 cm2/m2 in men, <39.0 cm2/m2 in women | 73 | 104 | 7 | B |
| Mirzai et al. (2023) ( | USA | Retrospective | CS | 67 ± 9 | 27.1 ± 4.8 | 6.7 (5.5–12.2) | CT: pectoralis SMI | Pectoralis SMI < 9.16 cm2/m2 in men, <6.21 cm2/m2 in women | 45 | 133 | 8 | B, C |
| Lee et al. (2022) ( | Korea | Retrospective | CS | 72 (68–75) | 24.2 (21.9–26.3) | 2.2 (1.6–3.1) | CT: L3-SMI | L3-SMI < 55.0 cm2/m2 in men, <39.0 cm2/m2 in women | 292 | 874 | 7 | A, C |
| Kondo et al. (2022) ( | Japan | Retrospective | CS | 78.1 ± 5.2 | 22.5 ± 3.8 | NA | CT: L4-PMAi | L4-PMAi <956 mm2/m2 in men, <730 mm2/m2 in women | 29 | 140 | 5 | A |
| Hawkins et al. (2018) ( | USA | Retrospective | CS | 81 (77–85) | NA | NA | CT: L4-PMAi | NA | 60 | 240 | 5 | A |
| Subgroup analysis ( | ES (95% CI) |
| ||
|---|---|---|---|---|
| Overall (43) | 0.437 (0.386, 0.489) | <0.001 | 97.01% | <0.001 |
| Assessment of sarcopenia | ||||
| SMI (20) | 0.501 (0.413, 0.589) | <0.001 | 97.68% | <0.001 |
| PMAi (10) | 0.411 (0.359, 0.464) | <0.001 | 85.54% | <0.001 |
| PMA (4) | 0.373 (0.144, 0.638) | <0.001 | 98.91% | 0.016 |
| SMD (2) | 0.342 (0.317, 0.367) | <0.001 | 97.20% | <0.001 |
| Gait speed and grip (2) | 0.334 (0.270, 0.400) | <0.001 | 66.91% | <0.001 |
| Others (5) | 0.355 (0.267, 0.448) | <0.001 | 90.50% | <0.001 |
| Gender | ||||
| Male (9) | 0.505 (0.334, 0.675) | <0.001 | 98.34% | <0.001 |
| Female (10) | 0.462 (0.364, 0.561) | <0.001 | 94.44% | <0.001 |
| Mixed (24) | 0.403 (0.343, 0.465) | <0.001 | 96.92% | <0.001 |
| Study design | ||||
| Prospective (17) | 0.497 (0.399, 0.595) | <0.001 | 97.20% | <0.001 |
| Retrospective (26) | 0.402 (0.342, 0.464) | <0.001 | 97.00% | <0.001 |
| Ethnicity | ||||
| Caucasian (31) | 0.411 (0.351, 0.473) | <0.001 | 96.87% | <0.001 |
| Asian (11) | 0.520 (0.436, 0.607) | <0.001 | 96.22% | <0.001 |
| Latino (1) | 0.330 (0.239, 0.431) | <0.001 | NA | NA |
| Subgroup analysis ( | ES (95% CI) |
| ||
|---|---|---|---|---|
| Overall (26) | 1.48 (1.31,1.68) | <0.001 | 50.7% | 0.002 |
| Assessment of sarcopenia | ||||
| SMI (9) | 1.43 (1.25, 1.65) | <0.001 | 13.6% | 0.321 |
| PMAi (9) | 1.31 (1.04, 1.64) | 0.022 | 49.0% | 0.047 |
| Others (8) | 1.92 (1.42, 2.60) | <0.001 | 52.1% | 0.041 |
| Gender | ||||
| Male (4) | 1.15 (0.93, 1.42) | 0.205 | 0.0% | 0.939 |
| Female (4) | 1.45 (0.85, 2.48) | 0.176 | 72.3% | 0.013 |
| Mixed (18) | 1.59 (1.36, 1.85) | <0.001 | 53.4% | 0.004 |
| Study design | ||||
| Prospective (5) | 1.29 (0.86, 1.94) | 0.227 | 63.9% | 0.026 |
| Retrospective (21) | 1.52 (1.33, 1.74) | <0.001 | 49.3% | 0.006 |
| Ethnicity | ||||
| Caucasian (21) | 1.52 (1.31, 1.76) | <0.001 | 43.3% | 0.019 |
| Asian (5) | 1.39 (1.10, 1.75) | 0.005 | 53.6% | 0.097 |
| Follow up time | ||||
| 30 days (1) | 8.77 (0.79, 96.79) | 0.077 | NA | NA |
| 6 months (2) | 1.59 (1.15, 2.20) | 0.005 | 0.0% | 0.653 |
| 1 year (8) | 2.37 (1.62, 3.48) | <0.001 | 30.2% | 0.187 |
| 2 years (7) | 1.56 (1.30, 1.87) | <0.001 | 0.0% | 0.710 |
| >2 years (8) | 1.25 (1.09, 1.44) | 0.001 | 51.8% | 0.043 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
Introduction
1
Given advancements in extracorporeal circulation and cardiac surgical techniques, surgical aortic valve replacement (SAVR) has become the predominant cardiac intervention for elderly patients with aortic valve disease (1). While transcatheter aortic valve replacement (TAVR) now offers an alternative approach for treating aortic stenosis, SAVR remains advantageous for patients experiencing aortic regurgitation, infective endocarditis, ascending aortic aneurysms, or other valvular disorders (2, 3). Optimal treatment for elderly patients, however, necessitates a thorough evaluation of benefits and risks, with accurate postoperative mortality assessment remaining a fundamental concern for clinicians.
Baseline functional status is recognized as a strong indicator of surgical risk (4). Identifying specific patient risk factors is essential in guiding clinical decisions on whether TAVR or SAVR represents the optimal approach or if aortic valve replacement (AVR) is potentially non-beneficial. Modifiable factors among these may highlight possible avenues for additional interventions accompanying valve replacement to enhance post-procedural outcomes. Sarcopenia, a condition with implications for adverse clinical results in SAVR/TAVR, is characterized by age-associated reductions in skeletal muscle mass, strength, and physical function (5). Globally, sarcopenia prevalence spans 8–36% in individuals under 60 and 10–27% in those aged 60 or older (6). Prior research has consistently linked sarcopenia with cardiovascular diseases such as coronary heart disease, heart failure, and aortic stenosis (7, 8), positioning it as a risk factor for cardiovascular disease progression and negatively influencing patient prognosis (9, 10). Notably, sarcopenia independently predicts mortality in cardiac surgery patients and is prevalent among elderly patients, where it correlates with poorer post-surgical outcomes (11). Consequently, comprehensive sarcopenia evaluation is increasingly viewed by researchers as integral to refining decision-making in SAVR/TAVR.
As the population ages, the prevalence of age-related frailty increases sharply, which increases the risk of poor health status of older adults (12). Frailty syndrome is becoming increasingly prevalent with population aging, characterized by diminished physiological reserve and impaired stress response capacity. Research indicates that this state of heightened vulnerability exerts significant adverse effects on elderly patients undergoing AVR, manifesting as worsened postoperative dependency, increased readmission rates, elevated mortality, and other negative clinical outcomes (13). Frailty holds significant importance in assessing the risks of TAVR, particularly given the advanced age of many patients (14). However, frailty assessments are often subjective and rely on indirect measurements. Sarcopenia, one of the key biological contributors to frailty (15), can be utilized to evaluate surgical risks in TAVR patients. In the pursuit of objective frailty parameters, previous studies have extensively investigated the analysis of body composition metrics, with a particular focus on muscle mass and muscle strength (16). These parameters are widely applied in cardiac risk assessment. Numerous studies have examined sarcopenia’s predictive role in outcomes post-SAVR/TAVR, yet findings remain inconsistent and, in some cases, contradictory. For instance, Brouessard et al. (17) observed no significant association between sarcopenia and one-year rehospitalization or mortality rates following TAVR. Conversely, Heidari et al. (18) identified sarcopenia as an independent predictor of mortality in TAVR patients. Additionally, Mirzai et al. (19) demonstrated that unilateral pectoralis muscle measurements from preoperative cardiac magnetic resonance imaging may serve as a supplementary metric to conventional risk scores in predicting mortality risk post-SAVR. Despite these varied findings, no meta-analysis has yet synthesized evidence on sarcopenia’s impact on clinical outcomes in SAVR/TAVR patients. This study was therefore undertaken to (i) quantify sarcopenia prevalence in SAVR/TAVR patients, and (ii) assess sarcopenia’s association with post-SAVR/TAVR mortality.
Materials and methods
2
Searching strategy and methods
2.1
The study adhered to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (2020) guidelines, with the protocol registered in PROSPERO database (CRD42024606633).1 PubMed, Cochrane Library, Excerpta Medica Database (Embase), Web of Science, and China National Knowledge Infrastructure (CNKI) were searched, covering records from inception to July 1, 2025, with no language restrictions to ensure a thorough capture of relevant studies. Two researchers executed this search, utilizing keywords encompassing but not limited to: “TAVI” OR “TAVR” OR “transcatheter aortic valve implantation” OR “transcatheter aortic valve replacement”; “aortic valve replacement” OR “AVR” OR “surgical aortic valve replacement” OR “SAVR”; AND “sarcopenia” OR “sarcopenic” OR “muscle mass” OR “muscle strength” OR “hand strength” OR “grip strength” OR “muscle atrophy” OR “muscle wasting.” Related references in these studies were achieved. The search strategy employed across databases has been documented in detail (Supplementary Table 1).
Inclusion and exclusion criteria
2.2
Eligible studies were selected: (i) Participants: patients with sarcopenia undergoing SAVR/TAVR; (ii) Exposure: sarcopenia, defined per each study’s criteria due to the lack of a standardized definition; (iii) Comparison: patients without sarcopenia; (iv) Outcome: association between sarcopenia and mortality risk; (v) Study design: prospective or retrospective cohort studies. Exclusion criteria: (i) absence of definitely reported diagnostic criteria for sarcopenia, rendering data extraction infeasible; (ii) narrative reviews, comments, editorials, case series, conference abstracts, or related letters; (iii) studies treating sarcopenia as an outcome rather than a prognostic factor; (iv) publications in non-English languages.
Data extraction
2.3
Data extraction from each study was executed in a standardized form. Two reviewers independently gathered the following details: first author’s name, publication year, study design, location, patient sample size, mean or median age, body mass index (BMI), Society of Thoracic Surgeons (STS) score, sarcopenia definitions, muscle mass and function metrics, sarcopenia prevalence, and outcomes. For studies lacking specific data, attempts were made to contact the authors for supplementary information or clarification; studies were excluded if responses were not obtained.
Quality assessment of included studies
2.4
Assessment of study quality was conducted independently by at least two authors employing a standardized assessment scale. The Newcastle-Ottawa Scale (NOS) scale was applied to case–control and cohort studies, comprising criteria on study population selection (4 items, one point each), comparability (1 item, two points), and exposure or outcome (3 items, one point each); scores between 0–3 signified low quality, 4–6 moderate quality, and 7–9 high quality. Disagreements during the quality assessment were addressed through discussions by reviewers or resolved by expert arbitration when necessary.
Statistical analysis
2.5
This meta-analysis focused on two primary outcomes: (1) sarcopenia prevalence in SAVR /TAVR patients and (2) the association between sarcopenia and mortality. A single-proportion meta-analysis was used to pool the prevalence estimates, with subgroup analyses stratified by sarcopenia definition method and sex. The prevalence of sarcopenia was used as the common effect size in this meta-analysis. The effect of sarcopenia on mortality was quantified through pooled hazard ratio (HR) or odds ratio (OR) with 95% confidence interval (CI), applying a random- or fixed-effects model based on study variance. The heterogeneity test employed I^2^ and Cochran’s Q statistics, with significant heterogeneity indicated by a p-value ≤ 0.1 or I^2^ ≥ 50% (20). Predefined subgroup analyses examined variables such as follow-up duration, diagnostic criteria, ethnicity, and study design. Sensitivity analysis Sensitivity analyses will be conducted, excluding studies from the analysis one by one (21). Given the limited studies per outcome, meta-regression analysis was not conducted to examine sources of heterogeneity. Begg’s funnel plots were conducted to evaluate the publication bias qualitatively. A (Begg’s) funnel plot was used to visually detect the presence of publication bias in the meta-analysis. Begg’s test and Egger’s test were performed to quantitatively assess the publication bias (22). Statistical significance was defined as a two-tailed p < 0.05, with all analyses performed in STATA 11.0.
Results
3
Literature screening process
3.1
A total of 986 articles were initially retrieved through the search (strategy detailed in Supplementary Table 1). Following duplicate removal, 745 unique articles remained, from which titles and abstracts were reviewed, yielding 251 for further analysis. Of these, 101 full texts underwent screening, and 61 articles were excluded for reasons specified in Figure 1. After additional exclusions of partially irrelevant or duplicate studies (n = 2), 38 eligible articles were included. In SAVR patients, one article (11) analyzed ORs, 2 examined HRs (11, 19), 6 focused solely on prevalence (11, 19, 23–26). For TAVR patients, 31 articles addressed prevalence (16–18, 23, 26–52), 19 examined HRs (16–18, 27, 29, 32, 34, 36, 37, 39–41, 44, 45, 47, 49, 51–53), 5 focused solely on ORs (18, 33, 36, 45, 46). The identification process was illustrated in the flowchart in Figure 1.
Flow diagram of literature screening.
Literature characteristics
3.2
Table 1 provides an overview of study characteristics included in this study. SAVR patients: Six studies contributed to the qualitative analysis, with all studies published post-2016. Among these, six studies used retrospective designs. Sample sizes ranged from 15 to 874, with patient ages averaging between 67 and 85 years. The participant population covered diverse regions: three studies in Asia, and three in America. TAVR patients: Similarly, 32 studies were analyzed qualitatively, all published after 2016, comprising twenty-two retrospective and 10 prospective cohort studies. Sample sizes varied between 19 and 1,375, with a mean age range of 67 to 85 years. NOS scores indicated moderate to high study quality. Table 1 also details the diagnostic criteria for sarcopenia commonly applied. Twenty-eight studies identified sarcopenia via diminished muscle mass measured by CT scan, one used ultrasound, and another employed the sarcopenia index. Two additional studies (49, 50) utilized low muscle strength (grip strength) and physical performance (gait speed) as sarcopenia indicators. This finding highlighted the limited use of comprehensive sarcopenia criteria (only 2 studies using combined muscle mass and strength/performance) is valuable and underscores a gap in standardization.
SAVR
3.3
Prevalence of sarcopenia
3.3.1
In the six studies analyzed, sarcopenia prevalence varied between 20.7 and 62.5% (Table 1), with an overall pooled prevalence of 31.3% (95% CI 25.3–37.6%) (Figure 2). Subgroup analysis based on differing definitions of sarcopenia revealed substantial variation across groups. When defined by skeletal mass index (SMI), the prevalence was 38.2% (95% CI 28.5–48.4%, three studies); for psoas muscle area index (PMAi), the prevalence was 23.4% (95% CI 19.2–27.8%, two studies); and for TPA, a single study reported a prevalence of 32.5% (95% CI 25.1–40.5%).
The pooled overall prevalence of sarcopenia in patients undergoing surgical aortic valve replacement. ES, effect size; 95%CI, 95% confidence interval; SMI, skeletal muscle index; PMAi, psoas muscle area index; TPA, total psoas area.
Publication bias and sensitivity analysis
3.3.1.1
Funnel plots, along with Egger’s and Begg’s tests, assessed potential selection bias in the literature. The funnel plot demonstrated symmetry (Supplementary Figure 1A), and both Egger’s test (p = 0.707) and Begg’s test (p = 0.828) indicated no significant publication bias. Sensitivity analysis, conducted by sequential exclusion of individual studies, revealed no statistically significant variation in outcomes, confirming the stability of the results (Supplementary Figure 1B).
Sarcopenia and mortality risk
3.3.2
HRs
3.3.2.1
Two studies (11, 19) examined the correlation between sarcopenia and long-term mortality (≥1 year) post-SAVR, presenting multivariate analysis results that identified sarcopenia as a significant predictor of elevated mortality risk, with a pooled adjusted HR of 3.10 (95% CI 2.00–4.79, p < 0.001; Supplementary Figure 2). Additionally, the included studies demonstrated minimal heterogeneity (I^2^ = 0%, p = 0.46).
ORs
3.3.2.2
A study (11) identified an association between sarcopenia and 30-day post-TAVR mortality. According to Lee SA, sarcopenia correlated with an increased short-term mortality risk, with an OR of 2.46 (95% CI: 1.63–3.79, p < 0.05).
TAVR
3.4
Prevalence of sarcopenia
3.4.1
In the 31 studies reviewed, sarcopenia prevalence varied from 15.4 to 83.3% (Table 1), with a pooled estimate of 43.7% (95% CI, 38.6–48.9%) (Figure 3). Subgroup analysis by differing sarcopenia definitions revealed substantial variations across groups. Specifically, using SMI as the criterion, prevalence reached 50.1% (95% CI, 40.3–58.9%, 20 studies); with psoas muscle area index (PMAi), prevalence was 41.1% (95% CI, 35.9–46.4%, ten studies); psoas muscle area (PMA) indicated a prevalence of 37.3% (95% CI, 14.4–63.8%, four studies); gait speed and grip strength showed a prevalence of 33.4% (95% CI, 27.0–40.0%, two studies) (Table 2). Among male patients, the prevalence was 50.5% (95% CI, 33.4–67.5%) compared to 46.2% (95% CI, 36.4–56.1%) in females, indicating a slightly higher incidence in males (Supplementary Figure 3) (Table 2). The results of subgroup analyses are shown in Table 2.
The pooled overall prevalence of sarcopenia in patients undergoing transcatheter aortic valve replacement. ES, effect size; 95%CI, 95% confidence interval; SMI, skeletal muscle index; PMAi, psoas muscle area index; PMA, psoas muscle area.
Publication bias and sensitivity analysis
3.4.1.1
Potential publication bias in the literature selection was assessed through funnel plots, Egger’s test, and Begg’s test. Symmetry observed in the funnel plot (Supplementary Figure 4A) suggested minimal bias. Neither Egger’s test (p = 0.507 > 0.05) nor Begg’s test (p = 0.121 > 0.05) yielded statistically significant results, confirming an absence of notable publication bias. After sequentially excluding individual studies, sensitivity analysis revealed no statistically significant impact on outcomes, affirming the stability of the results (Supplementary Figure 4B).
Sarcopenia and mortality risk
3.4.2
HRs
3.4.2.1
Nineteen studies evaluated the link of sarcopenia to mortality risk following TAVR. All studies provided multivariable analysis, demonstrating a significant correlation between sarcopenia and increased mortality risk, with a pooled adjusted HR of 1.48 (95% CI 1.31–1.68, p < 0.001; Figure 4). Substantial heterogeneity was observed across studies (I^2^ = 50.7%, p = 0.001). Publication bias test used funnel plots, Egger’s, and Begg’s test (Supplementary Figure 5A). After excluding 1 study at a time, sensitivity analysis showed no significant change in results, affirming the finding robustness (Supplementary Figure 5B).
Forest plot for the association between sarcopenia and the risk of mortality after transcatheter aortic valve replacement (pooled HR value). HR, hazard ratio; 95%CI, 95% confidence interval.
Furthermore, this study identified that follow-up duration influenced mortality risk in sarcopenic patients, with longer follow-up times correlating with higher risk. For patients with follow-up exceeding 2 years, sarcopenia was linked to a HR of 1.25 (95% CI 1.09–1.44, p = 0.001) (Figure 4). In those followed up for exactly 2 years, the mortality risk associated with sarcopenia rose further, with HR of 1.56 (95% CI 1.30–1.87, p < 0.001) (Figure 4). Patients with a 1-year follow-up exhibited a HR of 2.37 (95% CI 1.62–3.48, p < 0.001), while for a 6-month follow-up, the HR was 1.59 (95% CI 1.15–2.20, p = 0.005) (Figure 4). One study reported a 30-day follow-up duration. However, Van de Velde-Van De Ginste et al. (49) reported no significant association between sarcopenia and mortality risk in TAVR patients (HR = 8.77, 95% CI 0.79–97.07, p = 0.077).
In addition, this study revealed that among the analyzed subgroups, variations in sarcopenia definitions (e.g., SMI or alternative criteria) may affect the association between sarcopenia and mortality risk. Patients with sarcopenia diagnosed through SMI exhibited a significantly elevated mortality risk, with HR of 1.43 (95% CI 1.25–1.65, p < 0.001) (Table 3). Furthermore, sarcopenia identified via the PMAi method showed statistically significant correlation with mortality risk, reflected in a HR of 1.31 (95% CI 1.04–1.64, p = 0.022), as detailed in Table 3. For patients diagnosed with sarcopenia using other diagnostic approaches (e.g., ultrasound, gait speed, grip strength, sarcopenia index, standardized PMA, PMA, muscle density), the condition remained significantly linked to increased mortality risk, yielding a HR of 1.92 (95% CI 1.42–2.60, p < 0.001) (Table 3). Notably, subgroup analysis by sex indicated no significant association between sarcopenia and mortality risk for either male (HR = 1.15, 95% CI = 0.93–1.42, p = 0.205) or female patients (HR = 1.45, 95% CI = 0.85–2.48, p = 0.176) (Table 3). Additional subgroup analysis results were presented in Table 3.
ORs
3.4.2.2
Six studies examined the link of sarcopenia to short-term mortality (≤30 days) following TAVR (Figure 5). No statistically significant association was found, with ORs spanning 0.73 to 1.75 and a pooled OR of 1.13 (95% CI 0.71–1.80, p = 0.616; Figure 5).
Forest plot for the association between sarcopenia and the risk of short-term mortality after transcatheter aortic valve replacement (pooled OR value). OR, odds ratio; 95%CI, 95% confidence interval.
Discussion
4
This study presents the first comprehensive systematic review and meta-analysis evaluating sarcopenia prevalence among patients with aortic stenosis (SAVR/TAVR). Sarcopenia is notably prevalent and increases with advancing age, yet it remains underdiagnosed and its clinical significance is often undervalued (54). Notably, patients selected for TAVR—representing a high-risk, elderly demographic with severe aortic stenosis ineligible for SAVR—exhibit a higher incidence of sarcopenia compared to SAVR patients. Clinicians are therefore encouraged to assess sarcopenia severity in both patient cohorts, as preoperative sarcopenia screening can enhance management planning and improve perioperative and postoperative risk assessment. Furthermore, this analysis explored the association between sarcopenia and patient outcomes across these surgical approaches, suggesting that sarcopenia may influence long-term postoperative mortality risk, potentially linked to frailty and malnutrition. Variability in diagnostic criteria likely contributed to differing sarcopenia prevalence rates across studies, but no significant disparity in sarcopenia prevalence was observed between the SAVR and TAVR groups. Additionally, race, sex, and study design were not found to impact sarcopenia prevalence.
Sarcopenia was initially defined as age-related skeletal muscle mass loss. More recently, it has been broadly characterized by both diminished muscle mass and reduced muscle strength (e.g., weak grip strength) and/or physical performance (e.g., slow gait speed) (55). In cardiovascular research, however, sarcopenia is predominantly diagnosed based on skeletal muscle mass, typically assessed by measuring muscle area at L3 vertebra using CT imaging (56). This method was employed by most studies included in the current review. A few studies, however, utilized chest CT scans at the thoracic vertebra levels T7 and T12 for muscle mass estimation. Given that CT scans in patients undergoing TAVR or SAVR are generally performed on the chest rather than the abdomen (57), the link to skeletal muscle measurements at L3 and T12 becomes particularly relevant, with stronger associations observed between these two levels (46). Further investigation is needed to establish the optimal threshold for defining sarcopenia using chest CT scans in TAVR and SAVR patients.
The prevalence of sarcopenia exhibited significant variability across studies in this meta-analysis, largely due to inconsistent cutoffs for low muscle mass. While cutoff values for sarcopenia are sex-specific, prevalence tends to be higher among male patients than female patients undergoing TAVR/SAVR, indicating a potential influence of sex on sarcopenia rates in this population. Prior research also suggests a stronger link between sarcopenia and functional decline in men compared to women (58, 59), possibly due to the higher incidence of smoking among men. Cigarette smoke, rich in free radicals, induces oxidative stress in skeletal muscle (60), and prolonged smoking contributes to neuromuscular junction degeneration (61). In this meta-analysis, smoking status likely served as a confounding factor in the sex-based differences in sarcopenia prevalence; however, subgroup analyses by smoking status were not feasible due to a lack of sex-specific smoking data in the included studies. Future research should further investigate the impact of sex differences on sarcopenia.
In noncardiac procedures, such as elective spine surgery, sarcopenia independently predicts intensive care needs and postoperative transfusion requirements (62). In cases of acute mesenteric ischemia, sarcopenic patients experience reduced postoperative complications and lower 30-day mortality rates (63). Defined by psoas muscle mass, sarcopenia also serves as an independent predictor of 2-year mortality, major complications, and complication severity following major colorectal surgery (64). As an objective indicator of frailty, sarcopenia reliably predicts early morbidity and mortality post-spine surgery (53). In the context of cardiac surgery, sarcopenia correlates with poorer prognostic outcomes (26, 65), including prolonged hospital stays among older adults (66). Consequently, sarcopenia has been increasingly recognized as a relevant predictor of adverse outcomes in cardiac procedures. This study identified sarcopenia as a significant predictor of mortality risk following TAVR/SAVR procedures. While findings suggest a limited impact of sarcopenia on short-term mortality among these patients, this may be attributed to the limited sample size across included studies. Most studies assessed sarcopenia using the SMI method, associating it with an elevated risk of postoperative mortality. In subgroup analysis, nine studies using PMAi to diagnose sarcopenia yielded a pooled HR of 1.31, also indicating the significant association between sarcopenia and post-TAVR mortality risk. In this study, we further separated participants into subgroups for ethnicity stratified analysis. In either Asian population or Caucasian population, sarcopenia was broadly and robustly associated with a higher risk of mortality. The relationship between skeletal muscle mass and post-TAVR/SAVR mortality likely involves the vital role of skeletal muscle in frailty syndromes (67), though underlying mechanisms remain poorly defined. Skeletal muscle serves as the primary amino acid reservoir, and depletion impairs several recovery-critical functions (68). TAVR/SAVR patients with diminished muscle mass exhibit reduced muscle protein synthesis and heightened vulnerability to deconditioning post-intervention, exacerbated by inadequate nutrition and limited physical activity (69). Emerging research indicating the anti-inflammatory and anti-apoptotic properties of skeletal muscle may offer insights into the observed outcomes (70). Patients with sarcopenia, however, may derive limited benefit from these protective effects (71). Post-operative muscle mass reduction extends beyond survival outcomes in TAVR/SAVR, as sarcopenic patients show an increased likelihood of requiring transfer to rehabilitation facilities (33). Consequently, CT has become a valuable tool in assessing muscle mass, facilitating early identification of sarcopenic patients who may benefit from targeted interventions—such as protein supplementation and physical rehabilitation—to improve frailty status post-TAVR/SAVR. With advances in medicine, nanoparticles may hold promise for the diagnosis and treatment of sarcopenia (72). Furthermore, several studies have shown positive impact of physical therapy and nutritional interventions on sarcopenia (73, 74), suggesting that preoperative strategies, including exercise training and dietary supplementation, may enhance outcomes for patients undergoing TAVR.
In addition, sarcopenia demonstrated a strong association with elevated long-term mortality following TAVR/SAVR, aligning with evidence from patients undergoing other cardiac procedures, including heart valve surgery (75), PCI (76), and endovascular aneurysm repair (77). Additionally, the studies analyzed indicated that sarcopenia served as an independent predictor of 1-year mortality risk, even after adjustments for STS scores and relevant covariates, reinforcing its value as a practical and accessible alternative to conventional risk scores in assessing TAVR/SAVR patients.
Analysis of studies included in this review indicated no significant link between sarcopenia and short-term (30-day) mortality in TAVR patients. This observation supports the view that short-term post-TAVR outcomes remain favorable and unaffected by sarcopenia, suggesting TAVR’s safety across a wide patient demographic with varying degrees of muscle mass decline during short-term follow-up. However, this result contrasts with findings from other cardiac surgeries. For instance, Ganapathi et al. reported the association of frailty with discharge to other than home and 30-day mortality in proximal aortic surgery patients (78), while Lee et al. (11) found sarcopenia correlated with higher 30-day mortality and extended hospital stays. Given that only six studies in this meta-analysis assessed 30-day mortality, further research is needed to clarify these findings. Accordingly, future investigations should explore the relationship between sarcopenia, short-term mortality, and other adverse outcomes post-TAVR.
However, several limitations affect this meta-analysis. First, the analysis only included English-language publications, which may exclude relevant studies in other languages. Second, the studies employed varying definitions of sarcopenia, which were adopted in this review. Although most studies rely on CT-based sarcopenia assessments, discrepancies in scan locations and cutoff values across studies may have introduced bias, potentially contributing to publication bias. Notably, sex-specific cutoff values for sarcopenia have been previously derived through optimal stratification, with thresholds of 38.9 cm^2^/m^2^ (women) and 55.4 cm^2^/m^2^ (men) being widely adopted; however, cutoff values in post-SAVR/TAVR studies remain inconsistent. Finally, limited reporting on postoperative complications related to sarcopenia is due to limited studies evaluating early mortality, with such interpretations vulnerable to competing risks bias. Thus, while the observed effects of sarcopenia on early outcomes merit attention, further research is needed for this domain.
Conclusion
5
In summary, the study reveals a high incidence of sarcopenia among SAVR/TAVR patients, correlating with increased long-term mortality but showing no significant association with short-term mortality. While existing guidelines advocate preoperative body composition measurement and functional assessment as screening measures (79), the findings support a stronger recommendation for pre-surgical muscle mass evaluation to enhance risk stratification and outcome prediction. Given the high prevalence and prognostic importance of sarcopenia in SAVR and TAVR patients, integrating nanoformulated therapies could offer a future-oriented, precision-based strategy to improve muscle health and reduce mortality. Future research should focus on translational applications of nanomedicine in cardiac geriatrics to bridge the gap between diagnosis and therapeutic efficacy in managing sarcopenia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Choe J Koo HJ Kang JW Kim JB Kang HJ Yang DH. Aortic annulus sizing in bicuspid and tricuspid aortic valves using CT in patients with surgical aortic valve replacement. Sci Rep. (2021) 11:21005. doi: 10.1038/s 41598-021-00406-3, PMID: 34697359 PMC 8549004 · doi ↗ · pubmed ↗
- 2Thongprayoon C Cheungpasitporn W Gillaspie EA Greason KL Kashani KB. The risk of acute kidney injury following transapical versus transfemoral transcatheter aortic valve replacement: a systematic review and meta-analysis. Clin Kidney J. (2016) 9:560–6. doi: 10.1093/ckj/sfw 055, PMID: 27478597 PMC 4957730 · doi ↗ · pubmed ↗
- 3Lim SJ Koo HJ Jung SC Kang DY Ahn JM Park DW . Sinus of Valsalva thrombosis detected on computed tomography after Transcatheter aortic valve replacement. Korean Circ J. (2020) 50:572–82. doi: 10.4070/kcj.2019.0385, PMID: 32281322 PMC 7321751 · doi ↗ · pubmed ↗
- 4Rumsfeld JS Ma Whinney S Mc Carthy M Jr Shroyer AL Villa Nueva CB O'Brien M . Health-related quality of life as a predictor of mortality following coronary artery bypass graft surgery. Participants of the Department of Veterans Affairs Cooperative Study Group on processes, structures, and outcomes of Care in Cardiac Surgery. JAMA. (1999) 281:1298–303. doi: 10.1001/jama.281.14.129810208145 · doi ↗ · pubmed ↗
- 5Kao CC Yang ZY Chen WL. Association between protoporphyrin IX and sarcopenia: a cross sectional study. BMC Geriatr. (2021) 21:384. doi: 10.1186/s 12877-021-02331-6, PMID: 34174837 PMC 8235857 · doi ↗ · pubmed ↗
- 6Petermann-Rocha F Balntzi V Gray SR Lara J Ho FK Pell JP . Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2022) 13:86–99. doi: 10.1002/jcsm.12783, PMID: 34816624 PMC 8818604 · doi ↗ · pubmed ↗
- 7Sohrabi E Rezaie E Heiat M Sefidi-Heris Y. An integrated data analysis of m RNA, mi RNA and signaling pathways in pancreatic Cancer. Biochem Genet. (2021) 59:1326–58. doi: 10.1007/s 10528-021-10062-x, PMID: 33813720 · doi ↗ · pubmed ↗
- 8Wong A Frishman W. Sarcopenia and cardiac dysfunction. Cardiol Rev. (2020) 28:197–202. doi: 10.1097/crd.0000000000000285, PMID: 31868771 · doi ↗ · pubmed ↗