Enhancing knowledge of hypertension among general practitioners in Pakistan through a Train-The-Trainer initiative
Tariq Ashraf, Rafat Sultana, Musa Karim, Kanwal Fatima Aamir, Mustajab Mujtaba, Shoukat Memon, Deedar Hussain Gajju, Abdul Qadir Bhutto, Umair Arif, Hassan Irshad Bajwa, Naveed Shehzad, Haji Maqsood Mehmood, Ijaz Ul Hassan, Syed Gulzar Ul Hassan, Waheed Ashraf, Muhammad Saleem

TL;DR
A training program for doctors in Pakistan significantly improved their knowledge of diagnosing and managing hypertension, which could help improve patient care in low- and middle-income countries.
Contribution
The study demonstrates the effectiveness of a Train-The-Trainer model in improving hypertension knowledge among general practitioners in Pakistan.
Findings
Before training, 92% of GPs scored less than 50 on a hypertension knowledge test.
After training, 38.5% of GPs achieved moderate or high knowledge scores (≥50).
Significant improvements were observed across all demographic groups, including female and younger GPs.
Abstract
Hypertension (HTN) affects over a billion people worldwide, with most cases in low- and middle-income countries (LMICs) where awareness and control remain low. In Pakistan, general practitioners (GPs) are usually the initial contact for hypertensive patients. Through the Train the Trainer (TTT) initiative, a group of consultant cardiologists were trained as master trainers to conduct training for GPs across Pakistan. This study aimed to assess the effectiveness of the TTT initiative regarding knowledge of GPs about the diagnosis and management of HTN. This study included 540 GPs from all over Pakistan. Participants attended HTN training workshops run by Master Trainers under the TTT model and completed a structured online questionnaire in relation to knowledge of HTN before and 1–3 months after training. Knowledge scores were derived from correct responses for 19 items. Pre-training…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
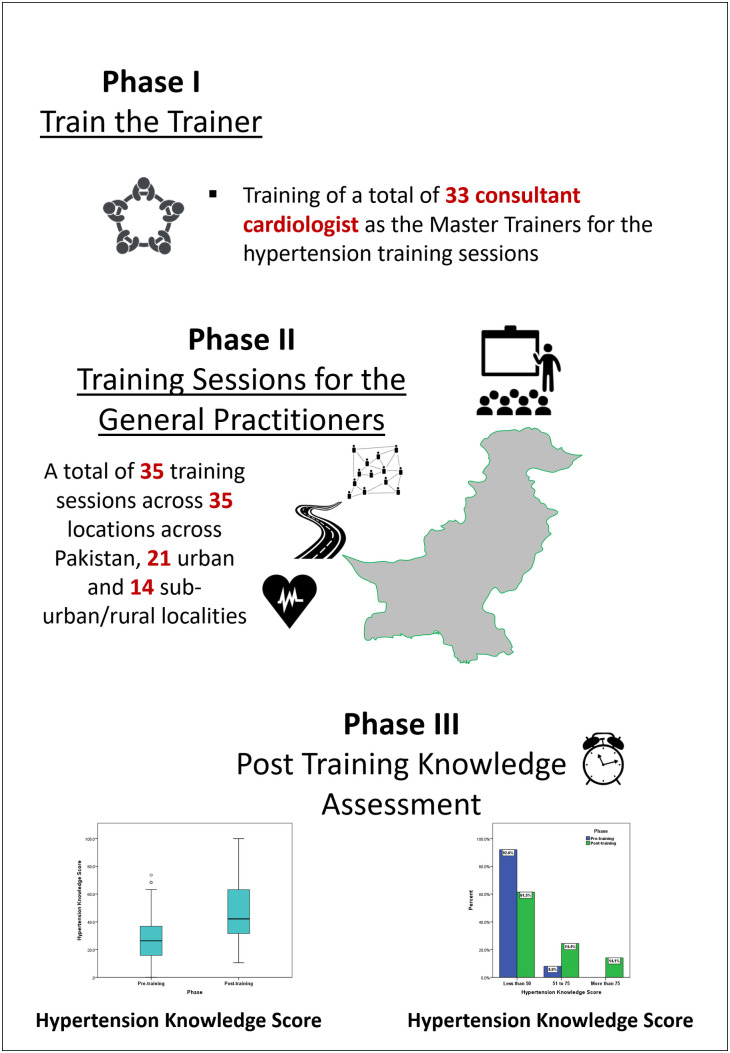 Fig 1
Fig 1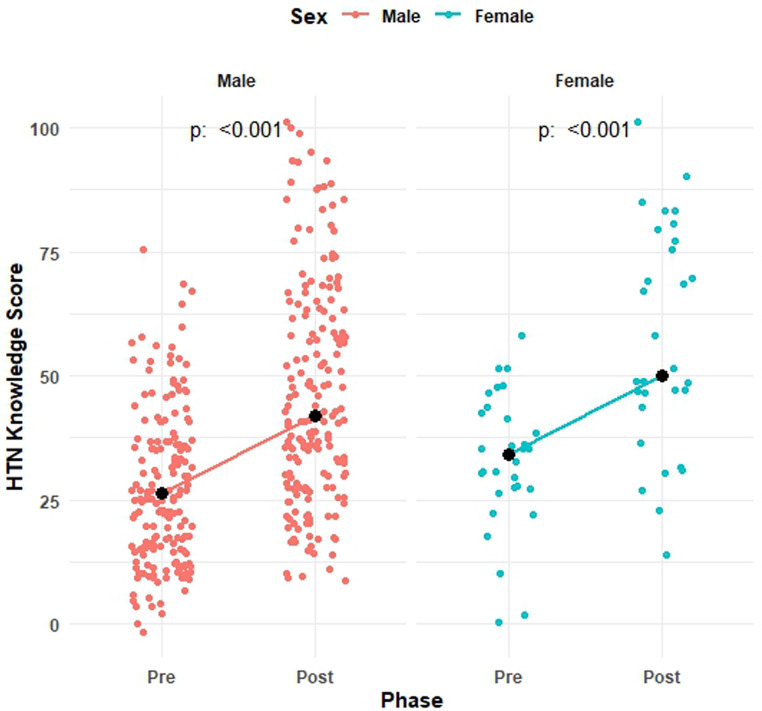 Fig 2
Fig 2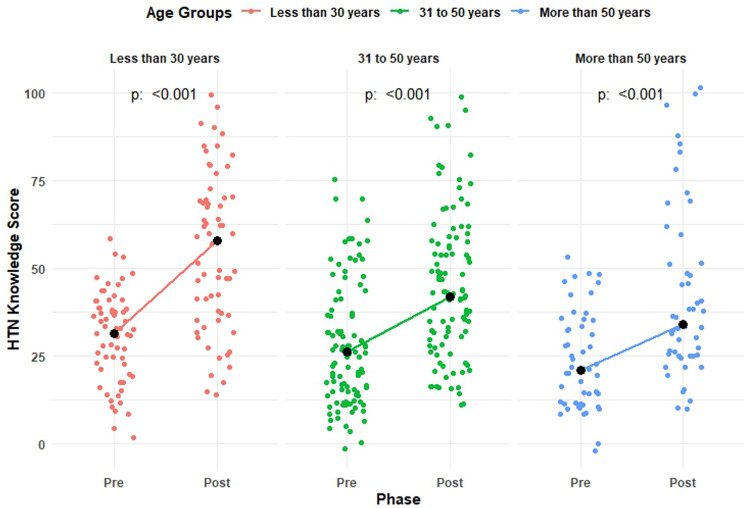 Fig 3
Fig 3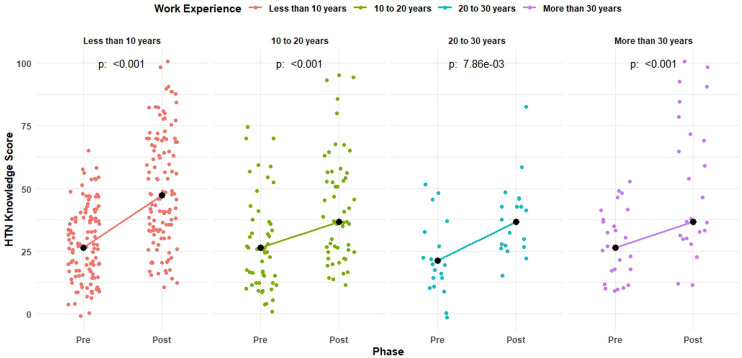 Fig 4
Fig 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Ophthalmology and Visual Health Research · Primary Care and Health Outcomes
Introduction
Hypertension is a medical condition defined by chronic elevation of arterial pressure in the systemic arteries above threshold values that have been established [1,2]. Recent estimates show that approximately a third of the world’s adult population (>1 billion people) are living with hypertension (HTN), and approximately 50% of these are unaware of their conditions [3]. The global prevalence of HTN among adults surged from 594 million in 1975 to 1.13 billion in 2015 [4], and WHO projections indicate this will rise to 1.56 billion by 2025, representing 29.2% of the global population [5]. Of patients with HTN, roughly 3/4th live in low- and middle-income countries (LMICs); of these, only perhaps 1 in 10 has their blood pressure controlled [3,6–9]. It is estimated that global direct medical costs for the treatment of HTN are approximately US100 billion annually [10]. Aside from its health impact, HTN is now also considered to be an economic problem in LMIC, with direct and indirect economic burdens brought about by the increasing healthcare cost and loss of productivity due to disabilities caused by the disease [8,11].
Epidemiological studies have reported the prevalence of HTN in Pakistan. For instance, one study estimated the rate to be 19.0% from 1990 to 1994 [12] using data from the National Health Survey, and another study specifically conducted in northern rural areas reported a prevalence of 14% in 2001 [13]. A couple of years ago, a more recent national health survey conducted by Saleem F et al. [14] in 2010 estimated that 33% of adults aged 45 years and 18% of all adults in Pakistan were hypertensive. Interestingly, one-third of the hypertensive clients over the age of 40 years were at risk due to a wide range of diseases. There is a dearth of primary research and updated surveillance data on the prevalence of hypertension in Pakistan. However, estimates from secondary sources, such as the Global Burden of Disease (GBD) study, indicate the age-standardized prevalence rate (per 100,000 population) of hypertensive heart disease is 138.55 for Pakistan in the year 2019 with a 3.79% change between 1990 and 2019 [15].
The survey also clearly showed that out of all the diagnosed hypertensive cases, only half received some form of treatment that resulted in controlled hypertension in just 12.5% of the cases [14]. These statistics underline the urgent need for improved screening, diagnosis, and management strategies in Pakistan, particularly given the associated risks of cardiovascular disease, diabetes mellitus, and chronic kidney disease. Several barriers at the patient, provider, and healthcare system level are identified that are derailing proper control and management of hypertension in LMICs. These include poor or lack of awareness of the condition, inadequate access to hypertension care, poor adherence to the treatment regimen and preventive measures, lack of proper distribution and drug procurement, poor surveillance and screening, lack of trained healthcare staff, and above all lack of proper training and awareness of healthcare providers [11].
HTN is mostly comorbid or precedes many other chronic diseases in Pakistan, such as diabetes mellitus, cardiovascular disease, and chronic kidney disease. Further, it is highly comorbid with behavioral factors, obesity, lack of exercise-and socio-demographic factors like family history [16]. Due to its majorly asymptomatic nature, coupled with the absence of systematic surveillance and screening protocols, HTN mostly goes undetected until its advanced stages, especially in LMICs like ours. Additionally, deviations from recommendations on testing largely contribute to inappropriate diagnosis and management [17]. Generally, patients with the condition or with high-risk features often seek help from general practitioners (GPs) [18]. An improper diagnosis and management by the GPs may result in further aggravation of the situation [17].
The limited availability of continuing medical education and the lack of access to updated guidelines among GPs contribute to poor adherence to best practices. Addressing these gaps requires national-level strategies focused on cost-effective and sustainable interventions, such as structured training programs for primary care providers [19,20]. No attempts are, however, made to increase the GPs’ awareness of hypertension, its prevention, and control in the communities in our population. However, the lack of structured training leads to significant gaps in their clinical knowledge and skills, potentially affecting patient outcomes. Traditional continuing medical education (CME) programs may not fully address these deficiencies due to their rigid structures, limited accessibility, and lack of competency-based approaches. To bridge this gap, there is a growing need for flexible, hybrid, and competency-based CME programs that provide tailored learning opportunities for GPs [21]. Consequently, a Train the Trainer (TTT) initiative was launched by the Pakistan Cardiac Society (PCS), the largest cardiology platform in Pakistan. Through this initiative, a group of consultant cardiologists were trained as master trainers to conduct sessions for GPs across Pakistan on the diagnosis and management of HTN.
In the light of above, a series of training for GPs all over Pakistan was planned to enhance GPs’ knowledge in the diagnosis and management of hypertension through the TTT approach. The study aimed to assess the effectiveness of the TTT initiative in improving awareness and knowledge regarding the diagnosis and management of HTN.
Materials and methods
Study design: This study employed a quasi-experimental design to assess the pre- and post-training knowledge of GPs regarding the diagnosis and management of hypertension.
Study setting: In this study, we included GPs from across Pakistan who attended the hypertension training workshop through a non-probability convenient sampling technique. The study was conducted under the platform of the Pakistan Cardiac Society (PCS) and carried out with the guidance and oversight of its Executive Council. A total of 35 training sessions were conducted by 33 master trainers in 35 locations across Pakistan, including 21 urban and 14 suburban/rural areas, between February 17, 2024, and July 16, 2024 (Central Illustration).
Ethics: The study was designed and conducted in compliance with the Declaration of Helsinki and was approved by the Pakistan Medical Association Committee on Ethics (Reference No. BO/056/AMP/09). As data collection was conducted via an online questionnaire, electronic informed consent was obtained from all participants.
The consent form provided detailed information about the research, including its objectives, potential risks and benefits, and participants’ rights and responsibilities. Participants were informed that participation was entirely voluntary and that they could withdraw at any time without any repercussions. It was explicitly stated that their decision to participate or decline would not affect their professional standing. Additionally, participants were assured that all personal and medical information would be kept strictly confidential and secured.
Study participants: The study participants included GPs, also known as family physicians or general physicians, who were recruited from diverse backgrounds across Pakistan for the HTN training and assessment program. Participants met the inclusion criteria of being between 20 and 75 years old, regardless of gender, currently working as GPs in Pakistan, and having agreed to attend the hypertension training workshop. To minimize potential bias and confounding effects from recent training, GPs who had attended a structured HTN education or training program within the past six months were excluded from the study.
The Train the Trainers initiative: The TTT program was a structured training strategy designed for GPs. In the initial phase, 33 volunteer consultant cardiologists from across Pakistan were trained as master trainers for the hypertension awareness and knowledge workshop. Upon completion of their training, each master trainer conducted a GP training workshop at their respective home stations.
An audio-visual module, titled “Hypertension Essentials: A Comprehensive Guide/Course on Hypertension Management,” based on the latest hypertension diagnosis and management guidelines, was used for training both master trainers and GPs.
Assessment: The baseline and 1–3 months post-workshop knowledge of GPs was assessed using an online multiple-choice structured questionnaire, adapted from a previous study by Chen Q et al. [22] and modified to the regional context. One additional question on salt consumption behavior was included, based on the latest clinical guidelines [23,24].
The study instrument comprised 19 multiple-choice questions related to the diagnosis and management of hypertension and salt consumption. To ensure validity and consistency, the modified questionnaire was piloted with 30 respondents, who were not included in the final study sample.
The online questionnaire was developed using Google Forms, and all enrolled GPs were contacted 1–3 months after the training, with responses recorded using the same instrument and parameters.
Data collection: The online questionnaire began with an informed consent section, where participants were informed about the study’s purpose, the estimated completion time, and their right to object to the use of collected data for research and publication.
Each participant was allotted 15 minutes before the commencement of the workshop to complete the questionnaire via an online platform. The same questionnaire was used 1–3 months post-training to assess improvements in knowledge.
To protect participant confidentiality, no personally identifiable information was collected beyond consent. The survey data remained accessible only to the research team through a password-protected institutional Google Drive account with restricted access. Additionally, Google’s built-in security features, including two-factor authentication, were implemented to safeguard data integrity and prevent unauthorized access.
Sample size calculation: The sample size was calculated using the WHO Sample Size Calculator (Version 2.0), based on a previously reported accuracy rate of hypertension prevention knowledge of 49.2%, as cited by Chen Q et al. [21]. Assuming a 10% increase in knowledge post-intervention, with 80% power and a 5% level of significance, the minimum required sample size was estimated to be 388.
Consequently, a total of 547 GPs were enrolled in the hypertension training program through a non-probability convenience sampling approach. However, contact could not be established with seven (7) GPs for the post-training knowledge assessment, resulting in a final analysis of 540 GPs
Data analysis: Data analysis was performed using IBM SPSS version 21 and R version 4.3.1. Descriptive statistics such as mean ± SD/median and frequency (%) were obtained, and an appropriate McNemar test or Wilcoxon signed rank test was applied to compare the pre and post-correct response rate on each item of the questionnaire. The level of significance was set at ≤ 0.05 throughout the study. The cumulative knowledge score was calculated as 100 × percentage correct responses on 19 items and categorized as low, moderate, and high as a score of less than 50, 50–75, and more than 75, respectively.
Results
The study participants consisted of 540 GPs working across Pakistan. Participants were predominantly male (85.7%) and young with a mean age of 40.7 ± 13.2 years. More than half of the participants had work experience of less than 10 years. The distribution of baseline characteristics of the study participants is given in Table 1.
Table 1: Distribution of baseline characteristics of the study participants.
Poor knowledge regarding diagnosis and management of hypertension was observed with a median score of 26.3 [IQR: 15.8 to 36.8] and 92% (497) were reported to have poor (<50) scores (Fig 1). A significant improvement in overall knowledge score was observed after 30 days of training with a median score of 42.1 [31.6 to 63.2] (p < 0.001) and 38.5% (208) were reported to have moderate or high (≥50) scores increased by 8%, highlighting a substantial and meaningful improvement in hypertension knowledge among GPs. Significant improvement was observed in all knowledge parameters (Table 2).
Table 2: Distribution of correct response pre- and post-HTN training session.
Effectiveness of the TTT initiative in regards to knowledge of GPs about the diagnosis and management of HTN.
A significant improvement was observed in the pre and post-median scores of males (21.1 [15.8 to 36.8] vs. 42.1 [26.3 to 57.9]) and females (31.6 [26.3 to 42.1] vs. 52.6 [47.4 to 78.9]) participants (Fig 2), emphasizing potential differences in knowledge acquisition that may warrant further investigation.
Distribution and median pre and post-median knowledge score by gender.
A significant improvement was observed in the pre and post-median score in each of the age groups with median scores of 31.6 [21.1 to 36.8] vs. 57.9 [36.8 to 68.4], 21.1 [15.8 to 31.6] vs. 42.1 [31.6 to 57.9], and 21.1 [10.5 to 31.6] vs. 31.6 [26.3 to 52.6] among participants aged less than 30 years, 31–50 years, and more than 50 years, respectively (Fig 3). Suggesting that early-career physicians may benefit the most from structured training interventions.
Distribution and median pre and post-median knowledge score by age.
Similarly, a significant improvement was observed in the pre and post-median scores in each of the work experience groups with median scores of 26.3 [15.8 to 36.8] vs. 47.4 [31.6 to 68.4], 26.3 [10.5 to 31.6] vs. 36.8 [26.3 to 57.9], 15.8 [10.5 to 26.3] vs. 36.8 [26.3 to 42.1], and 26.3 [10.5 to 36.8] vs. 36.8 [31.6 to 78.9] among participants with work experience of less than 10 years, 10–20 years, 20–30 years, and more than 30 years, respectively (Fig 4).
Distribution and median pre and post-median knowledge score by work experience.
Discussion
In Pakistan, well-trained healthcare providers are not sufficient, and almost all GPs are often without access to new evidence-based medical guidelines or resources for CME. Healthcare resources are at a premium in large areas of Pakistan, and thus tailored cost-effective educational interventions are called for. Resulting from the largest cardiology platform in the country, we thus designed a series of training sessions involving consultant cardiologists for GPs across Pakistan to enhance their knowledge regarding the diagnosis and management of HTN.
The result has shown that the TTT approach significantly enhanced the GPs’ understanding regarding HTN. Most participants had low levels of knowledge before the intervention, with a median score of 26.3 (IQR: 15.8–36.8), and 92% scoring below 50. Whereas post-training knowledge scores have increased significantly to a median of 42.1 (IQR: 31.6–63.2) and 38.5% achieved moderate to high scores ≥50. Improvement was found across all groups: women and younger GPs with less than 10 years of experience showed the greatest improvement. The low HTN knowledge among GPs at baseline agrees with previously reported findings in LMIC countries, which did not show awareness about HTN among health professionals due to the general scarcity of available training opportunities and resources [28]. Notably, the greatest improvements were observed among younger GPs and female participants, reinforcing the potential impact of targeted training interventions. These findings align with previous studies in LMICs, which report similar challenges related to awareness and training opportunities among healthcare providers.
Our study demonstrates that the significant post-training increase in knowledge supports the utility of the TTT programs for enhanced diagnostic skills among GPs. Additional support for this result is demonstrated in other successful TTT models in LMICs, which show that training primary care providers results in improved HTN control rates in their respective communities. Importantly, a parallel study by Mujtaba et al. [25] also investigated the effectiveness of a workshop intervention aimed at improving GPs’ knowledge in five cities of Sindh, Pakistan, about the correct methods of BP measurement. It indicated that there was a statistically significant improvement in GPs’ knowledge, with mean correct responses increasing from 8.0 ± 2.1 to 14.0 ± 2.5 post-workshop. Dalfó-Pibernat et al. [26] conducted a study to learn the effect of focused training on knowledge regarding ambulatory blood pressure monitoring (ABPM) among nurses and physicians in Spain. The findings indicated that 85.3% of participants reached adequate scores post-training compared to 26.7% pre-training, showing a significant gain in knowledge. The mean global punctuation received an increase of almost 3 points, from 6.3 to 9; 90.5% of the participants scored higher after the intervention. The study conducted by Setia et al. [27] assessed management practices related to hypertension and blood pressure variability (BPV) among physicians in Singapore. In the same manner, significant gaps in adherence to guidelines and the need for training on BPV were observed. Collectively, these studies underscore the importance of continuous professional development initiatives in optimizing hypertension care.
This questionnaire-based study conducted among 60 physicians from various specialties revealed that while the majority used home blood pressure measurements, only a small fraction of physicians followed the recommended cutoffs of blood pressure for diagnosis. ABPM was most valued by specialists but underutilized, often because of refusals due to cost barriers. The survey indeed found that only 48% of the respondents used the threshold levels of BP recommended by the guidelines to diagnose hypertension, and the pattern of treatments varied among the specialties. For the patients with comorbidities, therapies in combination were preferred. A similar finding reporting a disconnect between guidelines and actual practice was also noted by Green BB et al. [28]. This was reflected in the survey of healthcare professionals in these 10 clinics, wherein most acknowledged the accuracy of manual BP and 24-hour ABPM but generally used clinic BP measurements as a rule for diagnosis. Besides that, few providers followed the recommended threshold of 135/85 mmHg for out-of-office measurements; the use of 140/90 mmHg was common. Although many physicians, physician assistants, and advanced practice nurses expressed a preference for ABPM if readily available, the lack of adherence to guidelines and limited availability of preferred tools suggest barriers to optimal hypertension diagnosis [28].
In the scoping review, Todkar S, et al. [29] present a synthesis of global studies assessing the knowledge, perception, and practice of healthcare professionals regarding BP measurement through the home, ambulatory, automated office, and traditional office BP modalities. Knowledge of home blood pressure measurement (HBPM) and office blood pressure measurement (OBPM) was suboptimal at 40% unfavorable and 68% unfavorable, respectively. On the other hand, ABPM demonstrated a higher positive knowledge of 86%. Of all these, the overall belief had it that the blood pressure measurement (BPM) methodologies were informative, but the HBPM came close to 80% while the ABPM attained an incredible 93%. However, for the adherence to the hypertension guidelines in practice, the results were all negative for all the BPM methodologies, with the ABPM at 71%, closely followed by the OBPM at 73%, and lastly, the automated blood pressure measurement (AOBP) at 50%. A global scoping review by Todkar et al. [29] further revealed significant discrepancies between knowledge and practice, with adherence to recommended BP measurement methods remaining suboptimal across various settings.
These findings of the study further bring into focus the fact that there is a dire need to have regular targeted training among GPs, as they are usually the first contact for hypertensive patients. Better knowledge of the diagnosis and management of HTN among the GPs will lead to early detection and better education of the patients, thus possibly a reduction in healthcare costs due to unmanaged complications of HTN. This would further help in bridging the gap in HTN care in Pakistan, where a considerable number of patients remain undiagnosed and poorly managed due to poor capacity among specialized providers.
This in turn will ultimately determine the longer-term effect this TTT initiative has on actual clinical practices and patient outcomes, such as BP control rates and incidence of HTN-related complications. This kind of training should be extended to other healthcare providers, such as nurses and community health workers, as a way of further reinforcing hypertension management at the level of primary care. Other post-training reinforcement modalities could include follow-up workshops, online resources, and periodic refresher sessions that would help to maintain knowledge gains over time. A wider review might also consider at greater length the place of the TTT programs in medical curricula with respect to continued knowledge acquisition and use.
Limitations: This study has several limitations. First, the quasi-experimental design without a control group prevents direct attribution of knowledge improvements solely to the Train-the-Trainer (TTT) intervention. Second, the study relied on self-reported assessments, making it susceptible to social desirability bias and self-selection bias, as GPs who chose to participate may have been more motivated or already more knowledgeable. Third, the follow-up period of 1–3 months is relatively short for assessing long-term knowledge retention, and the study did not evaluate whether knowledge gains were sustained over time. Finally, while the study assessed knowledge improvement, it did not measure whether these changes translated into improved clinical practices or better patient outcomes. Future research should incorporate long-term follow-up assessments and explore the impact of knowledge enhancement on clinical decision-making and patient care.
Conclusion
The TTT approach has been found to be effective in improving the knowledge of GPs for the diagnosis and management of HTN in Pakistan and may indicate that similar models lead to an important role in the improvement of HTN control in LMICs. This might result in early detection, better treatment, and a reduction in complications of the disease by providing competency in dealing with HTN to primary healthcare providers. Continuation and scale-up of the TTT programs are hereby recommended to further these improvements and, eventually, reduce the burden of HTN in such countries as Pakistan.
Supporting information
S1 FileData file in MS Excel Format.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/A Ph A/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e 127–248. doi: 10.1016/j.jacc.2017.11.006 29146535 · doi ↗ · pubmed ↗
- 2Bakris G, Ali W, Parati G. ACC/AHA versus ESC/ESH on hypertension guidelines: JACC guideline comparison. J Am Coll Cardiol 2019;73(23):3018–26.31196460 10.1016/j.jacc.2019.03.507 · doi ↗ · pubmed ↗
- 3Moran AE, Gupta R. Implementation of global hearts hypertension control programs in 32 low-and middle-income countries: JACC International. J Am Coll Cardiol 2023;82(19):1868–84.37734459 10.1016/j.jacc.2023.08.043 · doi ↗ · pubmed ↗
- 4Mahadir Naidu B, Mohd Yusoff MF, Abdullah S, Musa KI, Yaacob NM, Mohamad MS, et al. Factors associated with the severity of hypertension among Malaysian adults. P Lo S One. 2019;14(1):e 0207472. doi: 10.1371/journal.pone.0207472 30605462 PMC 6317782 · doi ↗ · pubmed ↗
- 5GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–49. doi: 10.1016/S 0140-6736(20)30752-2 33069327 PMC 7566194 · doi ↗ · pubmed ↗
- 6Geldsetzer P, Manne-Goehler J, Marcus M-E, Ebert C, Zhumadilov Z, Wesseh CS, et al. The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. Lancet. 2019;394(10199):652–62. doi: 10.1016/S 0140-6736(19)30955-9 31327566 · doi ↗ · pubmed ↗
- 7Rosende A, Di Pette D, Brettler J, Rodríguez G, Zuniga E, Connell K, et al. HEARTS in the Americas appraisal checklist and clinical pathway for comprehensive hypertension management in primary care. Rev Panam Salud Publica. 2022;46:e 125. doi: 10.26633/RPSP.2022.125 36071921 PMC 9440731 · doi ↗ · pubmed ↗
- 8Turana Y, Tengkawan J, Chia YC, Nathaniel M, Wang J-G, Sukonthasarn A, et al. Hypertension and stroke in Asia: A comprehensive review from HOPE Asia. J Clin Hypertens (Greenwich). 2021;23(3):513–21. doi: 10.1111/jch.14099 33190399 PMC 8029540 · doi ↗ · pubmed ↗