Bandage Contact Lens-Assisted Plaque Brachytherapy for Anterior Segment Tumors: A Novel Technique to Prevent Corneal Complications
Neiwete Lomi, Deepsekhar Das, Bhavna Chawla, Tapashree Ghosh, Dhanabalan Rajasekaran, Radhika Tandon

TL;DR
A new technique using a bandage contact lens during eye tumor treatment helps prevent corneal damage while effectively controlling the tumor.
Contribution
Introduces a bandage contact lens as a buffer in plaque brachytherapy to reduce corneal complications.
Findings
A 48-year-old patient showed tumor regression with no corneal complications after seven months.
Two additional patients had stable tumors and no adverse effects after six months.
The technique may be safer than amniotic membrane grafts for anterior segment brachytherapy.
Abstract
Anterior segment tumors pose challenges in treatment due to their location and potential for globe loss. Plaque brachytherapy allows globe salvage, but placing plaques over the cornea and limbus may lead to epithelial defects and ulcers. We report a novel technique using a bandage contact lens as a buffer between the plaque and cornea in a 48-year-old woman with iridociliary melanoma. The lens thickness (0.07 mm) was included in radiation dose planning. The patient had no corneal complications and showed tumor regression at seven months. Two additional patients treated similarly showed stable tumors and no adverse effects at six months. This method may offer a safer alternative to amniotic membrane grafts for anterior segment brachytherapy, reducing corneal toxicity without compromising tumor control.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1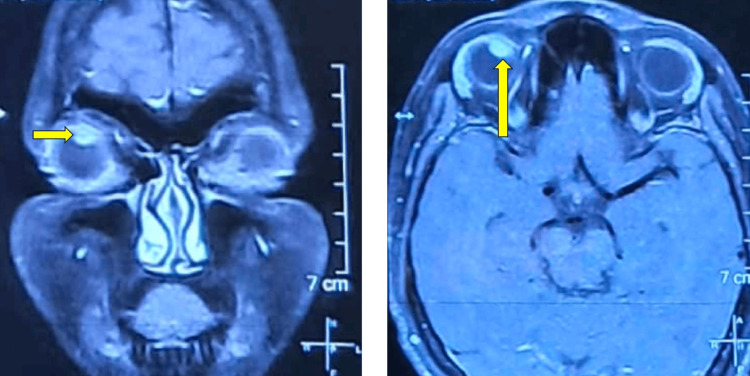 Figure 2
Figure 2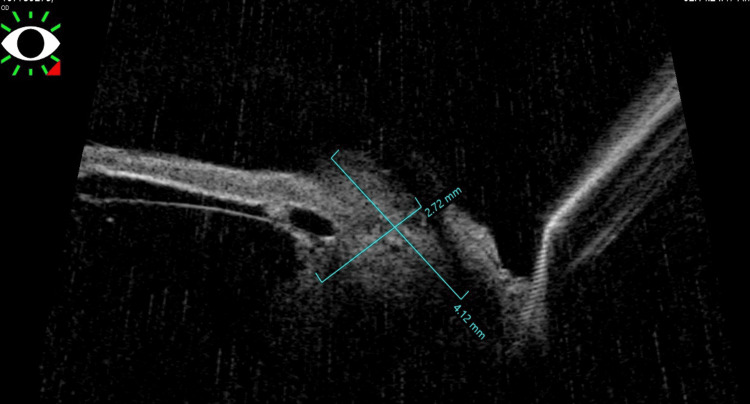 Figure 3
Figure 3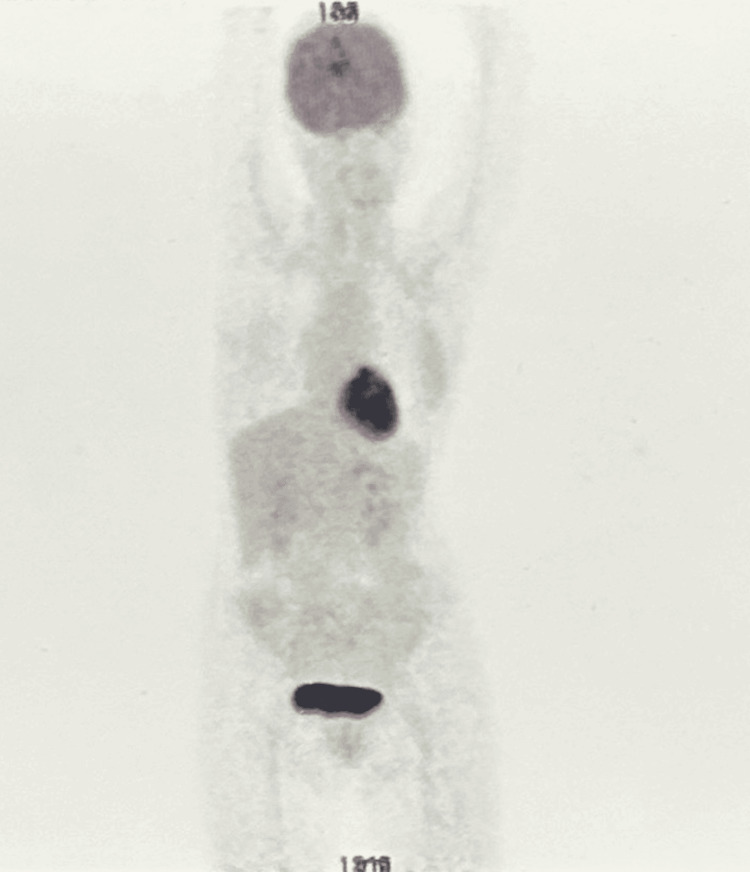 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Oncology and Treatments · Corneal Surgery and Treatments · Ocular Infections and Treatments
Introduction
Tumors of the anterior segment of the eye, including iris, iridociliary body, and corneal or conjunctival malignancies, represent a small but clinically significant portion of intraocular and ocular surface neoplasms. Their location in the anterior chamber, often in close proximity to delicate structures such as the cornea, lens, and angle, presents unique challenges in management. Enucleation has traditionally been the treatment of choice for extensive anterior segment tumors, particularly when there is concern for extraocular extension or vision-threatening complications [1]. However, with earlier detection and advances in ocular oncology, globe-sparing therapies have increasingly become feasible for small- to medium-sized lesions [1-3].
Plaque brachytherapy has emerged as an effective treatment modality for selected intraocular tumors, including those involving the anterior segment. This technique involves placing a radioactive source, commonly an iodine-125 or ruthenium-106 plaque, in close proximity to the tumor to deliver localized radiation while minimizing systemic exposure [4]. While it is well-established for posterior segment tumors such as choroidal melanoma, its application in anterior segment tumors requires significant technical modification. Plaques for anterior lesions are often sutured over the cornea and limbus, which differs markedly from their placement on the sclera in posterior segment treatments [5,6].
One of the significant drawbacks of anterior plaque placement is the high risk of ocular surface complications. The direct contact of the plaque with the cornea may lead to persistent epithelial defects, corneal edema, keratitis, and, in some cases, ulceration. The pressure, friction, and radiation exposure to the epithelium contribute to this complication profile. In a study by Semenova et al., up to 41.3% of patients undergoing epicorneal plaque brachytherapy with amniotic membrane grafts (AMGs) developed corneal complications, including epithelial breakdown and edema [7]. While AMGs provide some degree of surface protection, their mechanical durability during plaque application is limited, and they may degrade or shift over time.
To mitigate such complications, the present report introduces a novel technique: the interposition of a bandage contact lens (BCL) between the radioactive plaque and the corneal surface. BCLs are thin, transparent, and biocompatible devices commonly used in clinical ophthalmology to promote epithelial healing, reduce pain, and protect the cornea from mechanical trauma [8]. With a thickness of approximately 0.07 mm, these lenses offer a simple, cost-effective buffer without interfering with surgical visualization or significantly altering plaque dosimetry when accounted for during radiation planning.
This case report describes the successful use of BCL-assisted plaque brachytherapy in a patient with iridociliary melanoma, with no corneal complications observed over a seven-month follow-up period. The technique was further applied in two additional patients with favorable outcomes. We propose this method as a safer alternative to AMGs for anterior segment brachytherapy, particularly when epicorneal plaque placement is necessary.
Case presentation
A 48-year-old female presented with a six-month history of painless diminution of vision in the right eye. She also reported noticing a pigmented area in the superior part of the eye. There was no history of trauma, systemic malignancy, or ocular surgery. On examination, her best-corrected visual acuity was 6/60 in the right eye and 6/6 in the left eye. Intraocular pressure was 14 mm Hg in both eyes.
Anterior segment examination of the right eye revealed a pigmented lesion extending from the 12 o’clock to 2 o’clock position on the superior iris. Adjacent scleral pigmentation was also noted in the corresponding superior quadrant. The lesion appeared to extend posteriorly, raising suspicion for involvement of the ciliary body. The left eye examination was unremarkable (Figure 1).
Slit-lamp image of the right eye showing a pigmented lesion on the superior iris, along with pigmentation of the superior sclera
Ultrasound biomicroscopy (UBM) of the right eye confirmed the lesion to be iridociliary in origin. The mass measured approximately 2.75 mm in thickness and 4.12 mm in basal diameter (Figure 2). A contrast-enhanced MRI scan of the orbit was performed for further evaluation. The lesion appeared hyperintense on T1-weighted images and hypointense on T2-weighted images, consistent with the radiologic characteristics of melanoma (Figure 3). The lesion was localized to the iridociliary apparatus, with no evidence of extrascleral extension or orbital involvement.
CEMRI of the brain and orbit showing coronal and axial cuts with a hyperintense lesion in the superior aspect of the right orbita: Coronal section of CEMRI showing a hyperintense lesion in the superior quadrant of the right eye highlighted with a yellow arrow. b: Axial section of CEMRI showing a hyperintense lesion in the right eye highlighted with a yellow arrow.CEMRI: contrast-enhanced magnetic resonance imaging
UBM image showing an iridociliary lesion measuring 2.72 × 4.12 cmUBM: ultrasound biomicroscopy
Based on the clinical, imaging, and UBM findings, a diagnosis of iridociliary melanoma was made. A PET scan was performed to rule out metastasis (Figure 4). After a multidisciplinary discussion and patient counseling regarding treatment options, the decision was made to proceed with globe-salvaging plaque brachytherapy using ruthenium-106 (Video 1).
Whole-body PET scan showing no obvious FDG-avid lesions, thereby ruling out metastasisPET: positron emission tomography, FDG: fluorodeoxyglucose
BCL-assisted plaque brachytherapy
Treatment planning included the use of a P01 applicator, with a physical outer diameter of 12 mm and an active core diameter of 9.55 mm. A total radiation dose of 80 gray (Gy) was prescribed to a depth of 3.7 mm from the plaque surface, with a scleral surface dose of 244 Gy. The calculated duration of radiation delivery was 91 hours.
The patient underwent surgery under local anesthesia. A superior conjunctival peritomy was performed to expose the pigmented scleral region. Under direct visualization, a dummy plaque was positioned to confirm appropriate coverage of the iris and adjacent scleral lesion. Once accurate placement was confirmed, the dummy plaque was replaced with the radioactive plaque, which was sutured in place using 5-0 Ethibond sutures.
To minimize mechanical trauma and radiation-induced corneal epithelial damage, a BCL was inserted between the radioactive plaque and the corneal surface. The contact lens acted as a buffer, reducing direct plaque-corneal contact. A temporary tarsorrhaphy was then performed using 4-0 silk sutures to maintain plaque stability and minimize eyelid movement.
After 91 hours, the plaque was removed. Throughout the treatment period, the plaque remained well-positioned with no evidence of displacement. Notably, there were no signs of corneal epithelial defects, ulceration, or discomfort. The patient tolerated the procedure well, and no complications were observed postoperatively.
Discussion
Anterior segment tumors such as iridociliary melanoma present a therapeutic challenge due to their proximity to critical ocular structures and their potential for local invasion. Globe-sparing treatment options, particularly plaque brachytherapy, are effective for small to medium-sized tumors but require technical adaptations when lesions involve the anterior segment. Unlike posterior uveal melanomas, where the plaque is secured over the sclera, anterior segment tumors necessitate plaque placement over the cornea or limbus. This positioning increases the risk of radiation-induced or mechanical corneal complications, including epitheliopathy, edema, and ulceration [1,2].
Various strategies have been developed to reduce these complications, the most common being the use of AMGs. AMG has anti-inflammatory, anti-scarring, and epithelial-promoting properties, making it a valuable adjunct in ocular surface reconstruction [1]. Semenova et al. reported that despite using AMG during epicorneal plaque placement, 41.3% of patients developed corneal complications, indicating that while AMG may offer biological benefits, it does not provide robust mechanical protection [7]. The biologic nature of AMG also poses limitations: it may degrade during the plaque treatment period, shift from its intended position, or fail to uniformly cover the corneal surface, especially in mobile or blinking eyes.
In contrast, BCLs offer a mechanical barrier that remains stable throughout plaque placement. These lenses are designed to protect the corneal epithelium from friction and shear forces, promote epithelial healing, and reduce patient discomfort [8]. In our case, a BCL of 0.07 mm thickness was used; its presence was accounted for during radiation dosimetry planning. The BCL created a uniform interface between the radioactive plaque and the corneal epithelium, ensuring that no part of the plaque directly abutted the ocular surface. Over a 91-hour treatment period, the patient exhibited no epithelial defect, discomfort, or signs of corneal toxicity. This finding was replicated in two additional cases, all of which demonstrated plaque stability and intact corneal surfaces at follow-up.
BCLs also offer practical advantages. They are inexpensive, easy to apply, widely available, and do not require special storage or preparation. Unlike AMG, they do not involve biologic material, reducing the risk of immunologic reactions or graft failure. Additionally, BCLs allow for better control of plaque-to-corneal contact geometry, which can be consistently accounted for in treatment planning. These features make BCLs a particularly attractive alternative to AMG for plaque protection in anterior segment tumors [8].
Although early results are promising, limitations include the small number of patients and short follow-up duration. Long-term studies comparing BCLs and AMG directly in controlled settings are needed to validate their relative efficacy. However, this case series supports the use of BCLs as a safer, more stable mechanical buffer during anterior segment plaque brachytherapy.
Conclusions
Anterior segment plaque brachytherapy presents unique challenges due to the need for epicorneal plaque placement, which poses a risk of corneal epithelial damage. This case highlights a novel and practical approach using a BCL as a mechanical barrier between the radioactive plaque and the corneal surface. Compared to AMGs, BCLs offer consistent, stable protection without degradation or displacement over time. In our experience, this technique effectively preserved corneal integrity and provided excellent plaque stability without compromising tumor control. BCL-assisted plaque placement may serve as a simple, safe, and effective alternative for corneal protection in anterior segment radiotherapy. Further studies with larger cohorts and long-term follow-up are warranted to validate these findings and to establish standardized guidelines for this technique.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anterior plaque brachytherapy placement for treatment of iris and iridociliary melanomas - surgical procedure and institutional experience Indian J Ophthalmol Pike S Engelhard SB Greig LC Woods K Jennelle RL Berry JL 9129157220243818936610.4103/IJO.IJO_824_23PMC 11232867 · doi ↗ · pubmed ↗
- 2Disinsert, retract and rotate technique of plaque brachytherapy Indian J Ophthalmol Lomi N Chawla B Das D 30372202410.4103/IJO.IJO_2213_23PMC 1094191638273698 · doi ↗ · pubmed ↗
- 3Inferior oblique sparing brachytherapy plaque placement for juxtafoveal peripapillary choroidal melanoma Indian J Ophthalmol Lomi N Das D Chawla B Herle A 3033047320253985314510.4103/IJO.IJO_2207_23PMC 11991557 · doi ↗ · pubmed ↗
- 4Corneoscleral necrosis after episcleral Au-198 brachytherapy of uveal melanoma Retina Chaudhry IA Liu M Shamsi FA Arat YO Shetlar DJ Boniuk M 73792920091872861710.1097/IAE.0b 013e 3181863 f 7c · doi ↗ · pubmed ↗
- 5Plaque radiation therapy for malignant melanoma of the iris and ciliary body Am J Ophthalmol Finger PT 32833513220011153004410.1016/s 0002-9394(01)01007-8 · doi ↗ · pubmed ↗
- 6Ruthenium-106 brachytherapy for iris and iridociliary melanomas Br J Ophthalmol Marinkovic M Horeweg N Laman MS 1154115910220182912282410.1136/bjophthalmol-2017-310688 · doi ↗ · pubmed ↗
- 7Amniotic membrane corneal buffering during plaque radiation therapy for anterior uveal melanoma Ophthalmic Surg Lasers Imaging Retina Semenova E Finger PT 4774824420132404471110.3928/23258160-20130909-10 · doi ↗ · pubmed ↗
- 8Contact lenses for the treatment of ocular surface diseases Indian J Ophthalmol Sharma N Sah R Priyadarshini K Titiyal JS 113511417120233702624510.4103/IJO.IJO_17_23PMC 10276751 · doi ↗ · pubmed ↗