Mapping data on access to and use of medicines among migrants in Flanders
Loes Meukens, Saleh Aljadeeah, Cheng Chow, Loes Meukens, Loes Meukens, Yu par Khin, Loes Meukens, Loes Meukens, Alejandro Gil-Salmerón, Loes Meukens, Loes Meukens

TL;DR
This paper describes a data mapping initiative to improve access to and use of medicines among migrants in Flanders, Belgium.
Contribution
The study introduces a framework for identifying and evaluating datasets on migrant medicine access in Flanders.
Findings
A focused review will map datasets on migrant medicine access and use.
Ethical and legal challenges in using these datasets will be analyzed.
Recommendations for data retrieval and risk mitigation will be provided.
Abstract
Migration is a social determinant of health, and migrants often face health inequalities compared to host populations. Migrants are underrepresented in health research in many European countries, including Belgium, which is concerning. The World Health Organization (WHO) developed a comprehensive framework aimed at guiding research on migration and health within the WHO European Region. This initiative supports evidence-based policymaking among European member states by providing a foundational structure for examining various strategies and methodologies. The framework serves as a catalyst for discussion and critical analysis, contributing to the formulation of a global research agenda on migration and health under WHO’s leadership. Additionally, it outlines key research priorities and offers strategic recommendations to enhance the understanding and response to health issues related to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
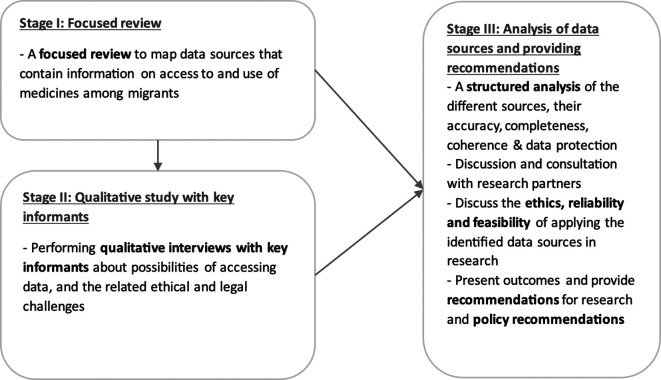 Figure 1
Figure 1| Stages | Research objectives | Research questions | Methods and data sources |
|---|---|---|---|
|
|
To map secondary data sources that contain information on access to and use of medicines among migrants. | Which sources/organizations in Flanders gather data on access to and use of medicines among migrants in Flanders? | A focused review to map datasets used for reporting access to and use of medicines among migrants |
|
|
To understand how these different data sources can be accessed, deidentified and curated, and identify the methodological and ethical challenges related to accessing and using these data. | What are the challenges and facilitators of ethically accessing data on medicines access/use among migrants in Flanders? | Qualitative interviews with key informants
|
|
|
To discuss the reliability and feasibility of applying the identified data sources in research studies that aim of evaluating the access to/use of medicines among migrants population in Flanders. | How can these data be used in future research studies that aim of evaluating the access to/use of medicines among the migrants population in Flanders? | Content description and evaluation of the different identified data sources, including discussion and consultation with research partners |
- —ITM Datahub (funded by the Department of Economy, Science & Innovation, Flanders)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigration, Health and Trauma · Global Health Workforce Issues · Migration, Identity, and Health
1. Introduction
1.1 Background
Migration is a longstanding and growing phenomenon. ^ 1 ^ The number of people living outside their countries of origin today is higher than at any time before. ^ 2 ^ Migration is a social determinant of health, and migrants often face health inequalities compared to host populations. ^ 3, 4 ^ Migrants are underrepresented in health research in many European countries, including Belgium, which is concerning. ^ 5 ^ In 2018, The UCL–Lancet Commission on Migration and Health called for more research into migration and health ^ 6 ^ as there is an increasing need for data that can reflect the diversity of migrant populations and their diverse health needs. ^ 5, 7 ^ Data are collected by different organisations, with different mandates (healthcare facilities, health insurance companies, NGOs, and -perhaps less frequently- research institutes). These data are very scattered.
Globally, the use of medicines stands as the most common used healthcare intervention and is fundamental to preventing, treating, and managing diseases. ^ 8 ^ Ensuring fair and consistent access to essential medicines is a critical measure of a nation’s advancement toward achieving Universal Health Coverage. ^ 9 ^ However, migrants across various European countries often encounter numerous barriers in their access to medicines. ^ 10 ^ Historically, healthcare providers in humanitarian contexts have attempted to overcome these challenges without established systems for managing patient health records. ^ 11 ^ This absence of formal medical record systems significantly limits researchers’ ability to systematically assess the quality and access to healthcare services available to migrant populations. Studies exploring the impact of electronic health record (EHR) systems in aiding displaced communities highlight their potential to enhance access to medicines, improve health outcomes, and foster better adherence to medicines. ^ 11 ^
1.2 Rationale
The WHO presented a framework for migration and health research in the WHO European Region as part of its remit to support evidence-based decision-making in its member states in Europe. ^ 12 ^ This framework was designed as a starting point for debating and analysing a broad range of options and approaches to help inform a WHO-led global research agenda on migration and health. The framework offers several recommendations for research, including a call to “maximise the use of existing data from research and routinely collected data in health information systems”. ^ 12 ^
Health information systems across Europe often lack comprehensive data on migrant populations, resulting in coverage gap in the data for this populations. ^ 13 ^ This issue is not due to limitations in existing knowledge or technological capacity but is primarily shaped by political and ethical considerations. ^ 13 ^ A major concern is that categorizing health data by migration status could potentially lead to discrimination against migrant groups. Additionally, collecting and disaggregating data on migrants is viewed as highly sensitive, raising ethical concerns aligned with established guidelines and the European Union’s General Data Protection Regulation (GDPR). ^ 13, 14 ^ Nevertheless, the GDPR permits the processing of sensitive data under specific conditions, provided there are legitimate reasons and sufficient protective measures in place. EU data protection regulations do not prohibit the collection and analysis of personal or health data for vulnerable populations, such as migrants, ^ 13, 15 ^ Instead, they offer frameworks to mitigate risks related to privacy and confidentiality.
Disaggregating and analyzing health data of migrant populations is essential for gaining a deeper understanding of their distinct healthcare needs and the challenges they face. Without utilizing these data in research, there is a risk of continuing the neglect of migrants’ unique health needs, resulting in inadequate healthcare responses and worsening disparities in access to health services, including essential medicines. ^ 13, 16– 19 ^ However, before such data can be effectively used, it is critical to thoroughly consider the ethical implications related to data collection, deidentification, processing, storage, analysis, and dissemination. Implementing strong pseudonymization or anonymization practices, along with secure systems to prevent patient re-identification, is vital to protecting the privacy of migrant populations. Ensuring data protection is particularly important to prevent the misuse of health data for non-health-related purposes, such as immigration enforcement. ^ 13, 15, 17 ^
In short, there is a need of a) mapping the different datasets that may include data about migrants’ access to and use of medicines; b) understanding how the different datasets can be deidentified and curated to ensure data protection, accuracy, completeness and coherence, as well as comparability across datasets; and c) identifying the methodological and ethical challenges related to accessing and using these datasets, and addressing these challenges with the ultimate aim of prioritizing the wellbeing and security of migrants. To address these needs, we will use the case of datasets that may contain direct or indirect information about access to medicine for migrants in Flanders, Belgium.
2. Study objectives
The overarching aim of this proposal is to map the available sources of data about access to and use of medicines among migrant populations in Flanders, Belgium, and assess if and under which conditions they can be used in M&E or research. It is important to recognize that this project does not aim to actually access data, but get information and guidance on how to access and curate data in a scientifically and ethically sound way. Any future plan to access and analyse datasets will be the object of a separate protocol.
The specific objectives are:
- a)To map sources of data that contain information on access to and use of medicines among migrants.
- b)To understand how different quantitative and/or qualitative data sources can be de-identified, curated, and assessed for accuracy, completeness and coherence, as well as comparability across datasets, for being used for M&E or research.
- c)To identify and describe the challenges related to accessing and using these data, including ethical and legal challenges, and to develop and describe viable strategies and recommendations for deidentification, data curation and risk mitigation.
- d)To assess the reliability and feasibility of applying the sources of data identified by this study in future research studies that aim at evaluating the access of/use of medicines among the diverse migrants population.
3. Study design
This project includes three separate stages ( Figure 1). During stage I, a focused review will be performed to collect information on different data sources that were used in published literature and reports in the relevant field. The outcome of a recently completed scoping review “Access to medicines among asylum seekers, refugees, and undocumented migrants across the migratory cycle in the European Union, European Economic Area, Switzerland and the UK: a scoping review” ^ 20 ^ led by the PI, which focused on access to medicines among migrants in Europe, will inform the focused review. Stage II will consist of qualitative interviews of key-informants in Flanders to discuss the possibilities of accessing, deidentifying and curating data, and of the ethical and legal challenges related to accessing and using these data. Key informants are a) those who are working in the collection, management and processing of datasets related access to or use of medicine (we will refer to them as data gatekeepers), and b) members of migrant communities. With stage III, we will discuss the reliability and feasibility of applying the identified data sources in scientifically and ethically sound research. This stage will imply triangulating the outcomes of Stage I and II, and formulating policy recommendations as well as recommendations for further research.
The overall sequential design of the research study, fractionated in three stages.
4. Methods
4.1 Procedures
4.1.1 Focused review:
We will perform a focused review to identify data sources that have been used in research and grey literature to report on access to medicine among migrants in Belgium. For this focused review we will follow the following steps:
- a. Defining the scope and objectives: We will search for studies and grey literature sources that reported on access to medicine among migrants in two regions of Belgium: Flanders and Brussels.
- b. Defining eligibility criteria: We will include studies and grey literature sources that have reported on access to and use of medicines among migrant populations in English and Dutch and was published after 2010.
- c. Defining data Sources: We will also conduct our search on PubMed, Google Search, and websites of relevant governmental and non-governmental organisations, e.g. WHO, Médecins Sans Frontières, Médecins du Monde, Sciensano, FOD Volksgezondheid, Vlaams Agentschap Zorg en Gezondheid.
- d. Screening and selecting materials: We will screen titles and abstracts against our inclusion criteria to identify potentially relevant documents. This will be followed by full text screening.
- e. Data Extraction and Synthesis: We will extract data on the sources of data used in the studies and reports. In addition, we will extract the information about the challenges related to accessing, collecting and using these data for research. The identified common sources of data will be used for shaping the qualitative interviews in stage II.
4.1.2 Qualitative study:
Qualitative interviews will be conducted with key informants, i.e. data gatekeepers and migrant community members. Details are separately explained in chapters 4.2-4.4.
4.1.3 Triangulation of the outcomes of the first two steps:
We will compare the outcomes of the focused review (stage I) with the results of the qualitative interviews (stage II) highlighting areas of convergence, divergence, or expansion. The compared and contrasted outcomes of both studies will be presented and discussed with a research advisory group, comprising a group of researchers from the ITM (Karina Kielmann, Joris Michielsen, Houssynatou Sy, Mira Schneider, and Marie Meudec) and from Boston University (Veronika Wirtz), to broaden the understanding of the outcomes and formulate recommendations for further research. Table 1 lists a summary of the different stages that will take place during the study and the respective methods for data collection. More details are explained in chapter 4.
4.2 Study population
During stage II, qualitative interviews will be performed in order to obtain insights from community members and data gatekeepers in the use of data sources regarding access to and use of medicines among migrants in Flanders.
4.2.1 Inclusion criteria:
- •Adult (≥ 18 years).
- • Community members: migrants who have been living in Belgium for over 5 years and are active members of the community. These include individuals with migration background who are in leadership roles within community organizations and social clubs.
- • Data gatekeepers: representatives of NGOs that provide care for migrants, staff of insurance companies, administrative and health staff in healthcare facilities (hospitals, outpatient clinics, pharmacies) in charge of collecting or processing data regarding access to or use of medicines, and other categories potentially identified through snowballing.
- •Willing and able to provide written informed consent.
4.2.2 Exclusion criteria:
- •Eligible persons who decline to consent to participation.
- •Minors.
4.2.3 Recruitment and sampling:
Contacts from the social and professional network of the principal investigator (PI), co-investigators and scientific advisors will be purposively sampled, aiming at enrolling a diverse group with a broad range of experiences and perspectives. Snowball sampling will be used to identify other potential participants, for reaching out to more isolated groups. Given the diversity of the data sources, we will likely interview a higher number of the data gatekeepers in order to improve balance in including different groups of participants.
4.3 Data collection
Data will be collected by the Principal Investigator (SA) or co-investigator (LM) remotely via GDPR-compliant online platforms, or -preferably- by face-to-face interviews. Data will be collected through semi-structured qualitative interviews, conducted in English or Dutch, based on the preference of the participant.
It is estimated that approx. 10-20 participants will be needed. However, the exact sample size will depend on the quality and diversity of the data; recruitment will continue and data will be collected until saturation. Topic guides by categories are being developed. A draft version is submitted, which will be finalized in line with the findings of the mapping in Stage I. ^ 22 ^
Remote interviews will be conducted via European General Data Protection Regulation (GDPR)-compliant platforms (e.g. Teams), and according to participant’s preference. Face-to-face interviews will be conducted in a secure setting proposed by/agreed with the interviewee. The interview sessions (remote and in-person) will be audio-recorded, if the participant explicitly agrees to be recorded; otherwise, hand notes will be taken by the Principal Investigator or co-investigator.
4.4 Qualitative data analysis
The recordings will be transcribed, and translated into English when needed. Recordings will be deleted once transcription and cleaning are completed. No direct personal identifiers will be transcribed, including the name of the employer or names of third parties who could be mentioned during the interview. Word will be used for data transcription. Following the thematic content analysis approach suggested by Braun and Clarke, ^ 21 ^ data will be coded and categorized and themes will be identified. This will involve collating codes into potential themes and gathering all data relevant to each potential theme.
5. Results
A study report will be shared with study participants through the same channels that were used to conduct the interviews with them, if they agreed to be further contacted by email for this scope. The study findings will form the basis for one or more open-access scientific publication(s) in a peer-reviewed journal. The outcomes will be also disseminated by means of a policy brief, conference presentations and meetings of NGOs active in assistance to migrants in Flanders or other relevant stakeholders who are involved in migrant assistance, healthcare or administrative affairs in Flanders. The policy briefs and dissemination to stakeholders are key for maximizing the social value of the study, and the likelihood that findings may provide useful guidance to improve the collection and use in research of data on migrants health.
Authors’ contributions
SA contributed to conceptualisation of the study, article selection, data collection through semi-structured qualitative interviews, data analysis, protocol drafting and critical revisions. LM contributed to article selection, data collection through semi-structured qualitative interviews, data analysis, protocol drafting and critical revisions.
Ethics review
The protocol was submitted for formal review and approval to the Institutional Review Board (IRB) of the Institute of Tropical Medicine [Approval number 1767/24; Date of approval 02/05/2024].
The study will be carried out according to the principles stated in the Declaration of Helsinki (2013 and any further revisions).
Informed Consent (IC) was obtained prior to interviews. Study participants (adults only) were informed that participation in the study is completely voluntary and that the participant can withdraw from the study at any time without any negative consequences.
The interviewer provided all the information about the study, and went through the Participant Information Sheet together with the participant in advance. The Data Protection Officer contact details were included in the ICF for questions about personal data processing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Organization for Migration (IOM): World Migration Report 2022. 2022. Reference Source
- 2United Nations (UN): Peace, dignity and equality on a healthy planet 2020. Reference Source
- 3World Health Organization (WHO): Refugee and migrant health 2020. Reference Source
- 4Roura M Dias S Le Master JW : Participatory health research with migrants: Opportunities, challenges, and way forwards. Health Expect. 2021;24(2):188–197. [published Online First: 2 February 2021]. 10.1111/hex.13201 33528082 PMC 8077110 · doi ↗ · pubmed ↗
- 5Aljadeeah S : Are Refugees (Really) a Hard-to-Survey Group? Fieldwork Experience with Syrian Refugees in Germany. J. Refug. Stud. 2022;35(3):1405–1409. 10.1093/jrs/feac 025 · doi ↗
- 6Orcutt M Spiegel P Kumar B : Lancet Migration: global collaboration to advance migration health. Lancet. 2020;395(10221):317–319. 10.1016/S 0140-6736(20)30107-0 32007150 · doi ↗ · pubmed ↗
- 7Biddle L Menold N Bentner M : Health monitoring among asylum seekers and refugees: a state-wide, cross-sectional, population-based study in Germany. Emerg. Themes Epidemiol. 2019;16:3. [published Online First: 7 July 2019]. 10.1186/s 12982-019-0085-2 31316579 PMC 6613239 · doi ↗ · pubmed ↗
- 8Royal Pharmaceutical Society: Medicines Optimisation: Helping patients to make the most of medicines 2013. 2016. Reference Source