Trichuriasis in Differential Diagnosis: A Case of Colonoscopic Identification
Ping He, Ankoor H. Patel, Anish Vinit Patel, Ellen Stein

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
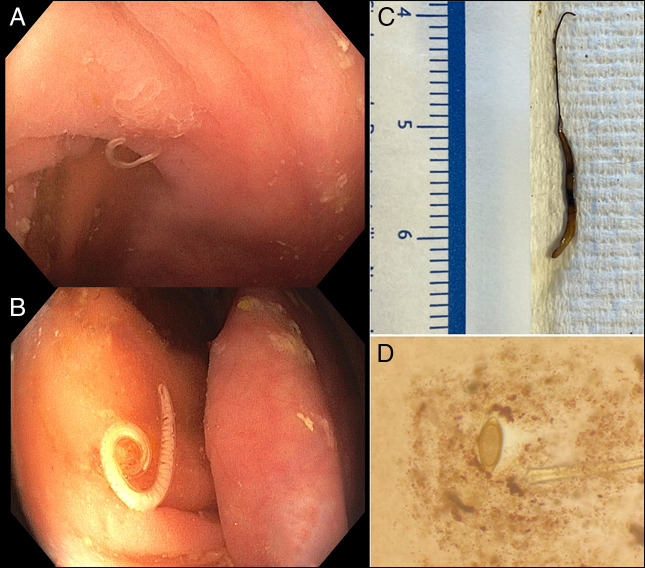 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Helminth infection and control · Parasite Biology and Host Interactions
CASE REPORT
Trichuris trichiura, the whipworm, is a soil-transmitted helminth that can infect the gastrointestinal tract and cause symptoms including vague gastrointestinal complaints, anemia, and eosinophilia. Globally, approximately 465 million people are infected in 2010.^1^ Heavy infections (≥800 worms) pose a substantial risk of anemia, with estimated blood loss of 0.005 mL per worm per day.^2^ We report a patient with iron deficiency anemia, irregular bowel habits, and eosinophilia, where T. trichiura infection was diagnosed by colonoscopy.
A 40-year-old woman with a history of hyperlipidemia presented with abdominal pain for 1 year. She described an intermittent, sharp pain in the left upper quadrant radiating to her back lasting 2 days and believed her symptoms associated with her menstrual cycles. She reported taking ibuprofen daily for 3 months. She reported irregular bowel habits alternating between constipation and diarrhea. She took oral iron for longstanding anemia, previously attributed to menorrhagia. She emigrated from Honduras 3 years ago. She denied any pertinent family history or prior endoscopic evaluations. Bloodwork revealed an iron deficiency anemia (Hemoglobin 11.4 g/dL; Iron 22 μg/dL, Iron Saturation 5%, TIBC 424 μg/dL) with peripheral eosinophilia (11.7%; 0.9 × 10^3^/µL). From prior emergency department visit, an ultrasound revealed cholelithiasis and a CT showed distended food-filled stomach and colonic stool burden.
Upper endoscopy revealed atrophic gastritis and duodenitis with biopsies showing increased intraepithelial lymphocytes without flat villi. Colonoscopy showed live intestinal worms at the cecum (Video, Figure 1). Fluid aspiration in the cecum for ova and parasites returned positive for Trichuris trichiura (Figure 1). She completed a 3-day course of albendazole, and eradication was confirmed by repeat testing. Evaluation for autoimmune atrophic gastritis and celiac disease was performed. This case underscores the importance of considering parasitic infections in the differential and recognizing associated endoscopic findings, especially in patients originating from endemic regions.
(A) Endoscopic image of Trichuris trichiura in its typical location in the cecum, seen next to the appendiceal orifice to the bottom left. (B) Near-focus image of female whipworm next to the ileocecal valve. (C) Pathology sample of the whipworm from (B), extracted endoscopically, with the characteristic “whip-like” anterior end. (D) Whipworm ova seen on stool O&P showing barrel-shaped, thick-shelled characteristics and possess a pair of polar “plugs” at each end.
DISCLOSURES
Author contributions: All authors worked in all 4 aspects of authorship as per ICMJE guidelines, including drafting, reviewing, investigating, and conceptualization.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pullan RL Smith JL Jasrasaria R Brooker SJ. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors. 2014;7:37.24447578 10.1186/1756-3305-7-37PMC 3905661 · doi ↗ · pubmed ↗
- 2Layrisse M Aparcedo L Martinez-Torres C Roche M. Blood loss due to infection with Trichuris trichiura. Am J Trop Med Hyg. 1967;16(5):613–9.6060065 10.4269/ajtmh.1967.16.613 · doi ↗ · pubmed ↗