A retrospective study on beta-blocker use and outcomes in hematopoietic stem cell transplant patients
Matthew A. Bergens, John T. Bokman, Ernaya J. Johnson, Matthew L. Braun, Yan Li, Amy T. Bush, Lauren Hill, Jolien Van Opstal, Alessandro Racioppi, Rebecca Fan, Sejal Kaushik, Edwin Alyea, Nelson Chao, Taewoong Choi, Cristina Gasparetto, Mitchell Horwitz, Richard Lopez

TL;DR
This study examined if beta-blockers improve outcomes in stem cell transplant patients but found limited evidence to support their routine use.
Contribution
The study provides new insights into the potential role of beta-blockers in allogeneic hematopoietic stem cell transplant outcomes.
Findings
Patients on beta-blockers had a lower incidence of acute GVHD, though not significant in multivariate analysis.
Non-selective beta-blockers were linked to lower post-transplant weight, and vasodilating beta-blockers showed a trend toward shorter hospital stays.
Abstract
Recent studies have linked beta-blocker (BB) use in critical care settings with improved survival outcomes, potentially due to beta-adrenergic receptor (β-AR) blockade and associated anti-inflammatory effects. Given the immune system’s role in the development of graft-versus-host disease (GVHD)—a major complication of allogeneic hematopoietic stem cell transplant (allo-HCT)—we conducted a single-center retrospective review to assess the impact of BB use on acute GVHD (aGVHD) and other survival outcomes in patients undergoing their first allo-HCT. We analyzed 10 years of data (January 2010 to May 2020), including 105 patients who received a BB for more than four days before and after HCT, and 669 control patients who did not receive a BB. Patients on BBs had a lower incidence of aGVHD (55.2% vs. 65.8%, p = 0.036); however, this difference was not statistically significant in multivariate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
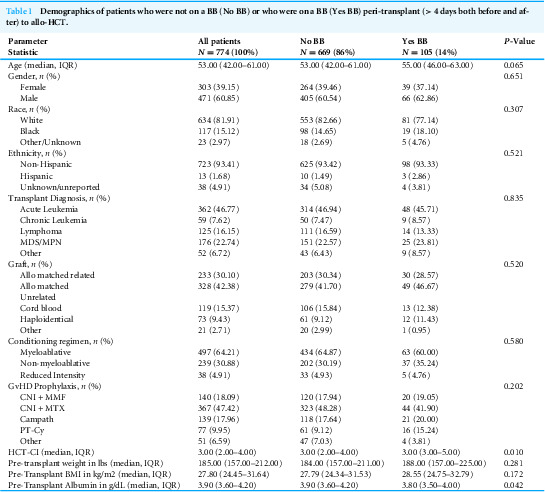 Figure 1
Figure 1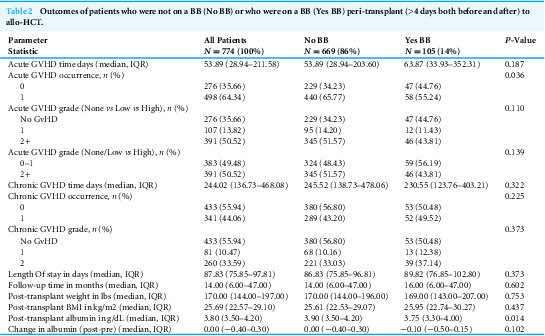 Figure 2
Figure 2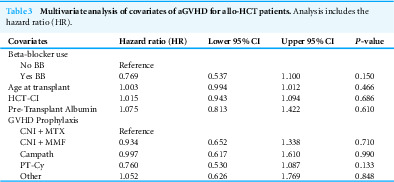 Figure 3
Figure 3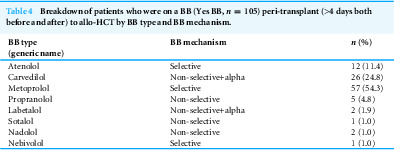 Figure 4
Figure 4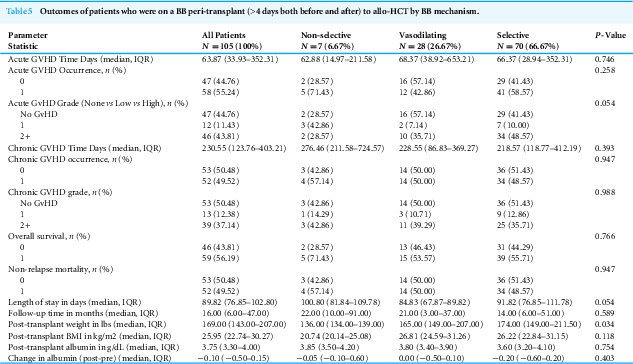 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Stress, Anesthesia, and Immune Response · Pediatric Pain Management Techniques · Family and Patient Care in Intensive Care Units
Introduction
Allogeneic hematopoietic stem cell transplant (allo-HCT) is an effective treatment for hematological malignancies, but its success is often complicated by graft-versus-host disease (GVHD). GVHD arises from a dysregulated immune response, where donor T cells attack host tissues. It is intricately connected to a cascade of pro-inflammatory signals through both cytokine release and immune cell activation, which leads to sustained tissue damage and inflammation (Ferrara, Cooke & Teshima, 2003; Holler, 2002; Piper & Drobyski, 2019; Jankovic et al., 2013). Approximately 30–60% of allo-HCT recipients develop acute GVHD (aGVHD) and the Center for International Blood and Marrow Transplant Research (CIBMTR) estimated that 12–14% of all deaths among HLA-matched allo-HCT recipients from 2018–2020 were due to GVHD (Bolon et al., 2022). In severe cases, patients with a grade III–IV acute GVHD (aGVHD) suffered a 29% transplant-related mortality rate (Jagasia et al., 2012; Khoury et al., 2017). Beyond its impact on mortality, aGVHD is also associated with increased hospital length of stay (LOS) and overall healthcare costs (Yu et al., 2019). Current first-line treatment for GVHD consists of immunosuppression with corticosteroids; however, this approach is only effective in 55–65% of cases, particularly with patients with severe GVHD (Flowers & Martin, 2015; Axt et al., 2019; Calmettes et al., 2015). Given the significant impact GVHD has on patients and the lack of a more reliable treatment, there is a need for improved prophylaxis to mitigate GVHD severity or incidence.
Beta-blockers (BB) are pharmacologically safe medications commonly used clinically for cardioprotection by modulating the beta-adrenergic receptor (b-AR) (Gorre & Vandekerckhove, 2010; Oliver, Mayor Jr & D’Ocon, 2019). However, recent research has highlighted their immunomodulatory effects in various clinical settings, including critical illness (Wilson et al., 2013; Morelli et al., 2013), burn injury (Herndon et al., 2001; Kopel et al., 2021) and cancer (Grytli et al., 2014; Hochberg, Cairo & Friedman, 2014; Jansen et al., 2014; Wang et al., 2013; Hwa et al., 2017). BB use in critically ill patients is associated with improved outcomes due to reduced systemic inflammation and attenuation of excessive immune activation (Wilson et al., 2013; Morelli et al., 2013). In oncology, BBs are associated with improved outcomes in various solid tumors and hematologic malignancies, including overall survival and disease-specific mortality, potentially due to mechanisms related to immune surveillance and inflammatory signaling (Grytli et al., 2014; Hochberg, Cairo & Friedman, 2014; Jansen et al., 2014; Wang et al., 2013; Hwa et al., 2017). These findings suggest that BBs may play a role in regulating inflammatory responses, which are central to GVHD pathogenesis.
BBs have previously been investigated in the setting of allo-HCT. One study on propranolol demonstrated a potential survival benefit, as well as underscored its feasibility and tolerability in allo-HCT patients (Knight et al., 2018). Another phase two randomized controlled trial found that propranolol inhibited stress-related pathways, suggesting potential benefits in reducing relapse and improving disease-free survival (Knight et al., 2020). Different b-AR receptor subtypes may have distinct role in modulating immune responses. In previous studies, B1-selective BBs have shown protection against catecholamine-induced injury in critical illness (Kuo et al., 2021; Heliste et al., 2022), while b2-AR has been implicated in enhancing the graft-versus-tumor (GVT) effect (Mohammadpour et al., 2018), and b3-AR is involved in modulating oxidative stress in hematopoetic stem cell redox homeostasis (Pasha, Calvani & Favre, 2021).
Since b-AR signaling impacts a wide variety of immune responses, including pro-inflammatory pathways (Ferrara, Cooke & Teshima, 2003; Holler, 2002; Piper & Drobyski, 2019; Jankovic et al., 2013; Powell et al., 2013), hematopoesis (Maestroni, 2020; Méndez-Ferrer, Battista & Frenette, 2010), and hematopoietic reconstitution after allo-HCT (Wang & Cao, 2019), BBs may have a beneficial role in allo-HCT. Blockade of b-AR signaling and the associated pro-inflammatory pathway could be a promising strategy to mitigate GVHD and improve post-HCT outcomes. Thus, we hypothesize that BB use prior to allo-HCT may be associated with decreased GVHD and improved survival outcomes.
Methods
Study design
This is a single center retrospective study that investigated a potential relationship between BB use and survival outcomes during allo-HCT. Patient data was pulled from the electronic health records (EHR) and then reviewed manually to ensure accuracy. A retrospective study design was chosen due to the availability of patient data in the Duke Adult Bone Marrow Transplant (ABMT) database, allowing for a sufficiently large sample size. This study allowed us to analyze real-world data without the time and resource constraints of a prospective trial. However, we recognize the limitations of a retrospective approach, such as potential selection bias, reliance on accurate documentation in medical records, and the inability to establish causation. Approval for exemption was obtained from the Duke University institutional review board (Pro00103818).
Patient population and data collection
All patients who received their first allo-HCT between January 2010 and May 2020 at the Duke ABMT clinic were included in this retrospective analysis. This timeframe was selected to maximize sample size while attempting to minimize variation in treatment regimen and inconsistencies from older charts. Demographic data including age, gender, transplant type, conditioning regimen, underlying hematological malignancy, and Hematopoietic Cell Transplantation-specific Comorbidity Index (HCT-CI) score before transplantation, were collected from the Duke ABMT database. Pre-transplant data was collected at D-10 and post-transplant data was collected at D+90. Outcomes such as GVHD occurrence and grade, length of stay (LOS), non-relapse mortality (NRM), relapse occurrence, overall survival (OS), and cause of death, were abstracted from the Duke ABMT Database.
All patients were chart reviewed to confirm their exposure to BB as well as record the specific BB administered. Patients were included in the BB group if they had exposure to a BB both before and after transplantation (peri-HCT). Due to limitations in record availability (2010–2020), precise duration of BB use could not always be determined. Additionally, the relationship between dose, plasma concentration, and clinical effect is variable among both individuals and different BBs, thus there is no universally accepted dose or duration that defines clinically significant beta-blocker exposure (Kendall, 1997; Heidenreich et al., 2022). Consequently, we selected an inclusion criterion requiring at least four consecutive days of BB use both before and after HCT, consistent with previous studies (Wijeysundera et al., 2014). This threshold was chosen to focus on patients with sustained BB exposure likely to exert meaningful physiologic impact, while excluding patients who initiated but quickly discontinued BBs due to intolerance or other medical concerns. Patients who had received a BB were then subdivided by the common clinical subdivisions of BB mechanism (selective BBs, non-selective BBs, and vasodilating BBs) to explore potential differences in outcomes based on pharmacologic properties (Oliver, Mayor Jr & D’Ocon, 2019).
Statistical analysis
The primary outcome endpoints included both aGVHD occurrence-rate and grade. Other secondary outcomes include chronic GVHD (cGVHD) occurrence-rate and grade and OS, NRM, relapse occurence, and LOS. For OS, the event is defined as all-cause death, and censured at last follow up. For NRM, the event is defined as date of relapse, and censured at last follow up. LOS is defined as number of days between transplant date and discharge from peri-HCT care, back to the patient’s local oncologist. Comparisons of patient characteristics were performed using Chi-squared test or Fisher’s exact test for categorical variables, and the analysis of variance or Wilcoxon Rank Sum test for continuous variables, respectively. The survival analyses were performed using the Kaplan–Meier method. The log-rank test was applied to detect overall group differences in outcome endpoints. Multivariate analysis (MVA) with the Cox proportional hazard model was used to evaluate the association of covariates and the aGVHD-free rates. The response variable of interest for the MVA was the occurrence of aGVHD, and the covariates include the variables that had significant effects in univariate analyses.
Results
Demographics were compared between patients who were on a BB before and after allo-HCT (Yes BB) (n = 105) and those who were not (No BB) (n = 669). The Yes BB group had a greater proportion of participants with an HCT-CI of 4 or greater (p = 0.010). However, there were no significant differences between the two cohorts by race, sex, median age, conditioning regimen, or donor type (all p > 0.05) (Table 1).
Table 1: Demographics of patients who were not on a BB (No BB) or who were on a BB (Yes BB) peri-transplant (> 4 days both before and after) to allo-HCT.
Patients in the Yes BB group had a significantly lower incidence of acute GVHD (55.2% vs. 65.8%, p = 0.036) (Table 2). Median albumin levels were lower in the Yes BB group at D-10 (p = 0.042) and D+90 (p = 0.014) than in the No BB group; however, the change in Albumin between D-10 and D+90 was not significant (p = 0.101). There were no observed differences in cGVHD occurrence or grade or other survival outcomes such as OS, NRM, relapse occurrence, and LOS (all p > 0.05) (Table 2, Figs. S1A–S1E). We performed multivariate analysis to further examine associations between BB use and other co-variates on aGVHD (Table 3). We included covariates that were associated with aGVHD on univariate analysis, as well as age at transplant and type of GVHD prophylaxis. Albumin at D+90 was excluded from MVA to avoid post-hoc confounding since aGVHD commonly occurs before D+90. None were statistically significant (Table 3).
Table 2: Outcomes of patients who were not on a BB (No BB) or who were on a BB (Yes BB) peri-transplant (>4 days both before and after) to allo-HCT.
Table 3: Multivariate analysis of covariates of aGVHD for allo-HCT patients.Analysis includes the hazard ratio (HR).
Additionally, we subdivided the Yes BB group by BB Mechanism (Table 4). Use of a non-selective BB (propranolol, sotalol, nadolol) was associated with lower pre-transplant weight compared to vasodilating BB (carvedilol, labetalol) and selective BB (atenolol, metoprolol, nebivolol) (136 lbs vs. 165 lbs vs. 174 lbs, respectively, p = 0.034). The use of vasodilating BB trended towards reduced LOS, however this just missed the cut-off for statistical significance (p = 0.054). There were no other significant differences in either primary or secondary outcomes for the mechanism-based subgroups (all p > 0.05) (Table 5).
Table 4: Breakdown of patients who were on a BB (Yes BB, n = 105) peri-transplant (>4 days both before and after) to allo-HCT by BB type and BB mechanism.
Table 5: Outcomes of patients who were on a BB peri-transplant (>4 days both before and after) to allo-HCT by BB mechanism.
Discussion
Our study found an association with decreased incidence of aGVHD in allo-HCT patients that had peri-transplant BB exposure on univariate analysis (p = 0.036); though this association did not remain significant on multivariate analysis (p = 0.150), suggesting that other factors may contribute to this trend, or that covariates may have overshadowed the BB effect. Therefore, we are hesitant to fully support a role for BBs as a prophylactic intervention to prevent aGVHD. One clinical study evaluated the risk of developing cGVHD for patients on a non-selective BB during the time of allo-HCT. While their results trended towards significance, that BBs were protective against cGVHD, they lacked sufficient power to detect a definitive difference. In our study, we found no association between BB and cGVHD occurrence (p = 0.947) or severity (p = 0.988). However, it is possible that a few days of peri-transplant BB exposure was insufficient to exert a lasting impact on this long-term outcome, given the median time to onset of cGVHD was 244 days (approximately 7.7 months) in our cohort. Future studies should include BB dosage and duration to better examine the impact of BB intake on long-term outcome evaluation of survival outcomes, including cGVHD.
The broader literature supports BB use as a potential adjunct in the care of cancer patients (Jansen et al., 2014; Wang et al., 2013; Hwa et al., 2017; Heliste et al., 2022; Patel et al., 2023; Tan et al., 2019). Additionally, previous studies have documented the role of b-AR signaling in influencing proinflammatory pathways and immune cell function (Ferrara, Cooke & Teshima, 2003; Holler, 2002; Piper & Drobyski, 2019; Jankovic et al., 2013; Knight et al., 2020; Kuo et al., 2021; Heliste et al., 2022; Mohammadpour et al., 2018; Pasha, Calvani & Favre, 2021; Powell et al., 2013; Maestroni, 2020; Méndez-Ferrer, Battista & Frenette, 2010; Wang & Cao, 2019). Recent laboratory studies in murine models have explored the b-AR role in GVHD modulation, specifically b2-AR signaling, in the modulation of GVHD from allo-HCT. A single study demonstrated that b2-AR activation ameliorated aGVHD, which opposes our hypothesis (Mohammadpour et al., 2020). The same team found that blockade of b2-AR improved GVT without impacting GVHD (Mohammadpour et al., 2018). Another team demonstrated that cold stress increased norepinephrine production, leading to excessive b-AR signaling and suppression of GVHD, which was reversed with b2-AR antagonists, supporting a role of b2-AR signaling in modulating GVHD severity (Leigh et al., 2015). Thus, there exists some data that there is potential impact in the allo-HCT population by modulating the adrenergic receptor; however, our results would not support the use of BB for survival benefits in allo-HCT. Possible explanations for the discrepancy between our findings and prior studies include differences in sample size, patient population, or BB dosing regimens. Additionally, variations in cGVHD diagnostic criteria and clinical management strategies across institutions may contribute to differing results. It is important to note that the lack of statistical significance in survival outcomes suggests neither benefit nor harm from BBs, consistent with current data on their pharmacological safety.
While BB use did not impact post-HCT weight overall (p = 0.753), subgroup analysis revealed that patients receiving non-selective BBs were associated with lower post-HCT weight compared to vasodilating and selective BBs (p = 0.034). The use of vasodilating BB trended towards reduced LOS (p = 0.054). Vasodilating BBs have been shown to reduce LOS in heart failure patients and those undergoing cardiothoracic surgery, likely due to their effects on hemodynamic stability and adrenergic modulation (Butler et al., 2006; Coleman et al., 2004; Fowler et al., 2001; Packer et al., 2002). While this relationship between BBs and LOS has not been explored in all HCT patients, our preliminary findings from our subgroup analysis suggest that BB types might variably impact a patient’s weight, and possibly LOS, during the peri-HCT period. Although further studies would need to substantiate these results and elucidate the underlying mechanism.
Several limitations of our study must be acknowledged. Our study is limited by the retrospective nature of the data collection. There are also underlying differences between the Yes BB and No BB groups, especially since the reasoning for being on a BB prior to allo-HCT is generally a co-morbidity that would increase HCT-CI and the potential risk of adverse events. While balanced in terms of demographics (except for HCT-CI), the Yes BB and No BB groups were unbalanced in terms of sample size, which could have contributed to the lack of statistical power to see a difference in additional outcome measures. While we attempted to control for confounding variables through multivariate analysis, residual confounding cannot be entirely excluded. Another limitation is the change in the use of cyclophosphamide during our cohort, where GVHD outcomes drastically improved, which could diminish the overall power we are able to detect. Lastly, the limited sample sizes in our subgroup analysis reduced the statistical power to detect differences, underscoring the need for larger prospective or randomized studies to strength any inference.
In conclusion, our study suggests that BB use does not significantly affect outcomes in allo-HCT patients, including aGVHD; however, subgroup analysis suggest that BB type may differentially affect post-HCT weight. While our study demonstrates that BBs remain pharmacologically safe in this population, our results do not support their routine use for modification of allo-HCT outcomes. Future prospective studies are necessary to substantiate these preliminary findings and explore the role of BBs in peri-HCT management to better understand their clinical implications and therapeutic potential.
Supplemental Information
10.7717/peerj.19822/supp-1Supplemental Information 1Overall survivalKaplan–Meier curves of (A) overall survival, (B) non-relapse mortality (NRM)-related rate, (C) acute GvHD-free rate, (D) chronic GvHD-free rate, and (E) relapse-free rate for treatment groups defined based on whether patients had at least four consecutive days of BB use both before and after transplantation (peri-HCT): patients who did not receive a beta blocker (No BB; blue) and patients who received a beta blocker (Yes BB; red). Overall group differences were evaluated using log-rank tests.
10.7717/peerj.19822/supp-2Supplemental Information 2Non-relapse mortalityKaplan–Meier curves of (A) overall survival, (B) non-relapse mortality (NRM)-related rate, (C) acute GvHD-free rate, (D) chronic GvHD-free rate, and (E) relapse-free rate for treatment groups defined based on whether patients had at least four consecutive days of BB use both before and after transplantation (peri-HCT): patients who did not receive a beta blocker (No BB; blue) and patients who received a beta blocker (Yes BB; red). Overall group differences were evaluated using log-rank tests.
10.7717/peerj.19822/supp-3Supplemental Information 3Acute GvHD-free rateKaplan–Meier curves of (A) overall survival, (B) non-relapse mortality (NRM)-related rate, (C) acute GvHD-free rate, (D) chronic GvHD-free rate, and (E) relapse-free rate for treatment groups defined based on whether patients had at least four consecutive days of BB use both before and after transplantation (peri-HCT): patients who did not receive a beta blocker (No BB; blue) and patients who received a beta blocker (Yes BB; red). Overall group differences were evaluated using log-rank tests.
10.7717/peerj.19822/supp-4Supplemental Information 4Chronic GvHD-free rateKaplan–Meier curves of (A) overall survival, (B) non-relapse mortality (NRM)-related rate, (C) acute GvHD-free rate, (D) chronic GvHD-free rate, and (E) relapse-free rate for treatment groups defined based on whether patients had at least four consecutive days of BB use both before and after transplantation (peri-HCT): patients who did not receive a beta blocker (No BB; blue) and patients who received a beta blocker (Yes BB; red). Overall group differences were evaluated using log-rank tests.
10.7717/peerj.19822/supp-5Supplemental Information 5Relapse-free rateKaplan–Meier curves of (A) overall survival, (B) non-relapse mortality (NRM)-related rate, (C) acute GvHD-free rate, (D) chronic GvHD-free rate, and (E) relapse-free rate for treatment groups defined based on whether patients had at least four consecutive days of BB use both before and after transplantation (peri-HCT): patients who did not receive a beta blocker (No BB; blue) and patients who received a beta blocker (Yes BB; red). Overall group differences were evaluated using log-rank tests.
10.7717/peerj.19822/supp-6Supplemental Information 6Raw data for the BB cohort
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Axt L Naumann A Toennies J Haen SP Vogel W Schneidawind D Wirths S Moehle R Faul C Kanz L Axt S Bethge WA 2019 Retrospective single center analysis of outcome, risk factors and therapy in steroid refractory graft-versus-host disease after allogeneic hematopoietic cell transplantation Bone Marrow Transplantation 54111805181410.1038/s 41409-019-0544-y 31089279 · doi ↗ · pubmed ↗
- 2Bolon YTAR Allbee-Johnson M Estrada-Merly N Lee SJ 2022 Current use and outcome of hematopoietic stem cell transplantation: CIBMTR summary slides 07 January 2024 https://cibmtr.org/CIBMTR/Resources/Summary-Slides-Reports
- 3Butler J Young JB Abraham WT Bourge RC Adams Jr KF Clare R O’Connor C 2006 Beta-blocker use and outcomes among hospitalized heart failure patients Journal of the American College of Cardiology 47122462246910.1016/j.jacc.2006.03.03016781374 · doi ↗ · pubmed ↗
- 4Calmettes C Vigouroux S Labopin M Tabrizi R Turlure P Lafarge X Marit G Pigneux A Leguay T Bouabdallah K Dilhuydy MS Duclos C Mohr C Lascaux A Dumas PY Dimicoli-Salazar S Saint-Lézer A Milpied N 2015 Risk factors for steroid-refractory acute graft-versus-host disease after allogeneic stem cell transplantation from matched related or unrelated donors Biology of Blood and Marrow Transplantation 21586086510.1016/j.bbmt.2015.01.01625617807 · doi ↗ · pubmed ↗
- 5Coleman CI Perkerson KA Gillespie EL Kluger J Gallagher R Horowitz S White CM 2004 Impact of prophylactic postoperative beta-blockade on post-cardiothoracic surgery length of stay and atrial fibrillation Annals of Pharmacotherapy 38122012201610.1345/aph.1E 31015507494 · doi ↗ · pubmed ↗
- 6Ferrara JL Cooke KR Teshima T 2003 The pathophysiology of acute graft-versus-host disease International Journal of Hematology 78318118710.1007/BF 0298379314604275 · doi ↗ · pubmed ↗
- 7Flowers MED Martin PJ 2015 How we treat chronic graft-versus-host disease Blood 125460661510.1182/blood-2014-08-55199425398933 PMC 4304105 · doi ↗ · pubmed ↗
- 8Fowler MB Vera-Llonch M Oster G Bristow MR Cohn JN Colucci WS Gilbert EM Lukas MA Lacey MJ Richner R Young ST Packer M 2001 Influence of carvedilol on hospitalizations in heart failure: incidence, resource utilization and costs. US Carvedilol Heart Failure Study Group Journal of the American College of Cardiology 3761692169910.1016/S 0735-1097(01)01190-111345386 · doi ↗ · pubmed ↗