A Systematic Review of Attributes Influencing Preferences for Treatments and Interventions in People With Amyotrophic Lateral Sclerosis (ALS)
A. Clift, D. Rowen, L. Knox, A. W. Griffiths, C. J. McDermott

TL;DR
This study reviews what matters most to people with ALS when choosing treatments, highlighting factors like ease of use, autonomy, and safety to improve patient-centered care.
Contribution
The study systematically synthesizes 44 preference-based studies to identify key factors influencing treatment preferences in ALS patients.
Findings
Five key factors influencing preferences are ease of use, accessibility, autonomy, and safety/reliability.
Preferences can inform healthcare policy and drug development through integration into target product profiles.
Patient-centered care improves satisfaction and treatment effectiveness in ALS.
Abstract
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease that has no cure, and treatments predominantly focus on improving quality of life. Patient‐centred care is central to bringing about meaningful improvements to quality of life. This review addresses the lack of consolidated evidence on what matters most to people with ALS (pwALS) by synthesizing 44 preference‐based studies covering six different treatment and intervention categories. Data‐based convergent synthesis identified five overarching factors influencing preferences: ease of use, accessibility, making life easier, autonomy, and safety/reliability. Simplifying and enhancing accessibility of treatment delivery across disease stages aligns with the nature of neurodegenerative disorders such as ALS, where function declines as the disease progresses. The value in perceived and real control reflects the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
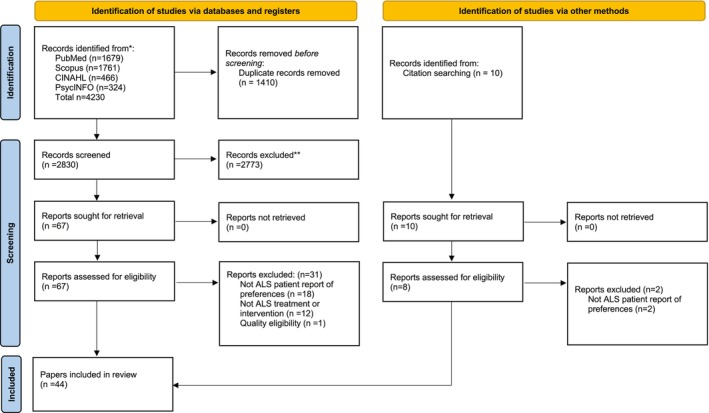 FIGURE 1
FIGURE 1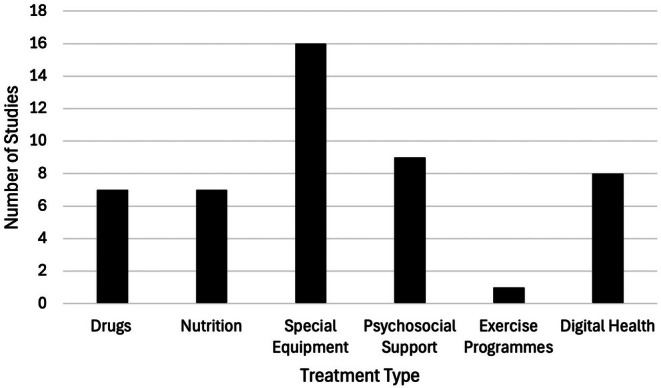 FIGURE 2
FIGURE 2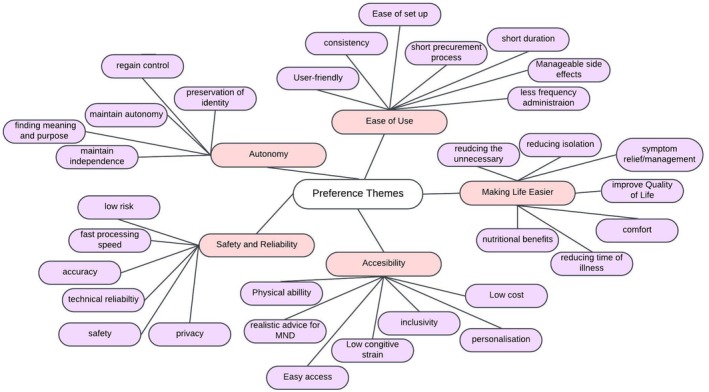 FIGURE 3
FIGURE 3| Author | Preference assessment | First order participant quotes/primary data from the studies. | Second order codes | Preference theme |
|---|---|---|---|---|
| Ludolf et al. [ | Patient Preference Survey (PPS) |
Low risk of choking and underdosing. Easier mode of delivery |
Low risk Ease of administration |
Safety/Reliability Ease of Use |
| Seo et al. [ | Discrete choice experiment |
The risk of device failure. Shorter overall durations and less frequent administration |
Low risk Less disruptive administration |
Safety/Reliability Ease of Use |
| Lunette et al. [ | Observational assessment | 22 patients voluntarily suspended from the burden of the duration and route of administration. |
Shorter duration Easier route of administration | Ease of Use |
| Zubair et al. [ | Semi structured Interviews |
“It would be good to have a standard syringe, because otherwise, you have to learn every time.” “The cost poses a barrier |
Easier administration Cost |
Ease of Use Accessibility |
| Quinn et al. [ | Patient report recorded by carers | The main reasons for not taking were discomfort from the gastrointestinal side effects 17/29 (58.6%) and from the taste of the drug 8/29 (29.6%). |
Side effects Taste | Ease of Use |
| Meyer et al. [ | Net Promoter Score (NPS), Treatment satisfaction questionnaire (TSQM‐9) |
10/32 found it difficult to use. 5/32 found it inconvenient or very inconvenient to use. | Ease of Use | Ease of Use |
| Jia et al. [ | Questionnaire then Interviews |
“at least it doesn't have so many side effects” “Riluzole is too expensive. If it is cheaper, I would try it” |
Side effects Cost |
Ease of use Accessibility |
| Author | Preference assessment | First order participant quotes/primary data from the studies. | Second order codes | Preference theme |
|---|---|---|---|---|
| Labra et al. [ | Interviews and analysis of physical function |
“I am thinking that it will help me because you can still go out” “I can use PEG to keep up my nutrition” |
Maintaining independence Nutritional benefit |
Autonomy # Making life easier |
| Guillemin et al. [ | Survey |
“It is difficult to use knives and other utensils” 6/10 (60%) had weight loss concerns. |
Ease in food preparation Nutritional benefit | Making life easier |
| Starvoulakis et al. [ | Semi structured interviews 3 months post PEG |
“Swallowing was becoming more difficult, “That's when she said, ‘Let's get it done”. |
Prolonged, tiring and effortful meals Choking and aspiration | Making life easier |
| van Eenennaam et al. [ | Semi structured Interviews | “I also wanted to continue to eat independently, no matter how difficult it was”. | Feeling of control | Autonomy |
| Hogden, Labra and Power [ | Semi structured interviews | “My main reason for getting the PEG was my swallowing” | Optimizing quality of life | Making life easier |
| Author | Preference assessment | First order participant quotes/primary data from the studies | Second order codes | Preference theme |
|---|---|---|---|---|
| Greenaway et al. [ | Semi structured interviews |
“As far as I'm concerned it's my life, what's left” “Yeah, it's the worry that it'll get infected” |
Perceptions of choice and control Aspects of fear |
Autonomy Safety and Reliability |
| Martin et al. [ | Interviews and beliefs about medicine questionnaire (BMQ) | More pleasure in eating were more likely to have refused an intervention | Control over illness | Autonomy |
| Ando et al. [ | Semi structured interviews |
“I wouldn't want it to be all of the time and not have any life” “claustrophobia – I just don't want it.” |
Preservation of the self Negative perceptions of mask |
Autonomy Safety and Reliability |
| Baxter et al. [ | Semi structured interviews in first month of NIV |
“I can get the mask on…but I can't, it's the clips.” “leaks just from the mask” “that mask on my face” |
Ease of set up Mask dysfunction Negative perceptions of the mask. |
Ease of Use Safety and Reliability |
| Siewers, Holmoy & Frich, [ | Interviews |
“it's not very complicated either. I think that will be important”. “So knowing that it is there |
Ease of Use Comfort in reliability |
Ease of Use Safety and Reliability |
| Huggins, Wren & Gruis, [ | Survey using 1–10 scale | Accuracy followed by simplicity as most important. Appearance was least important | Accuracy | Safety and Reliability |
| Geronimo et al. [ | 10 min demonstration then survey | 38/42 (90.5%) of ppts would like 90% accuracy and 50% required at least 80%. | Accuracy | Safety and Reliability |
| Eicher et al. [ | Semi structured interviews |
“It would be great if could also disburden somebody” patient was afraid…it might fall off the ceiling and hit him |
Maintain and retrieve autonomy Safety |
Autonomy Safety and Reliability |
| Creemers et al. [ | Survey | Long duration of application process, paperwork, knowledge and errors by supplier | Delays in procurement process | Ease of Use |
| Riera‐Punet et al. [ | Intervention for 3 months then questionnaire |
The main reason for not using it was discomfort. Difficulty making an impression to make the mold due to MND |
Comfort Physical barriers |
Ease of Use Accessibility |
| Spears et al. [ | Online Survey |
“Too uncomfortable” (51%) and “too restricting” (44%) led to users not wearing. (96%) want the collar to be well fitting. | Comfort | Ease of Use |
| Mackenzie et al. [ | Survey with closed and open questions |
“Since my hands ceased being able to move, I have been isolated from this”. “MND stops a person being independent, but with a computer (she) was able to communicate”. |
Lack of physical ability Reduce isolation |
Accessibility Making life easier |
| Peters, O'Brien & Fried‐Oken, [ | Questionnaire |
high cost due to insurance co‐payments. Concerns about using the device and it not working well |
Cost Risk of device failure |
Accessibility Safety and Reliability |
| Caligari et al. [ | Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) |
Side effects of bloodshot eyes from use. Regaining autonomy in personal life choices |
Side effects Regained autonomy |
Ease of Use Autonomy |
| Cave and Bloch, [ | Interviews |
“The voice helps me retain something of me.” “It's about control” |
Preserving identity Control | Autonomy |
| Spittel et al. [ | User experience survey | Issues included the unsuitability of the device 16/53 (30.2%) followed by rejection by the health care insurance 15/53 (28.3%) |
Adaptability to MND Cost | Accessibility |
| Author | Preference assessment | First order participant quotes/primary data from the studies. | Second order codes | Preference theme |
|---|---|---|---|---|
| Weeks et al. [ | Individual semi structured interviews then discussion groups |
“Having a therapist coming home would be very useful” “can't physically communicate | Adaptability to MND. | Accessibility |
| Pinto et al. [ | Think aloud interviews then intervention for 6 weeks then in‐depth interviews. |
More appropriate I think to people with motor neuron” Taking some control over what is happening to them. |
Realistic advice for MND Regaining control |
Accessibility Autonomy |
| Hardy, Castle & Jackson, [ | Survey with 5‐point Likert scale | Value the availability of psychiatric services even when have no symptoms | Accessibility | Accessibility |
| Marconi et al. [ | Weekly meditation for 8 weeks followed by interviews |
It was difficult for us to organize transportation” “wasn't easy to do exercises at home” |
Transportation Continuity | Accessibility |
| Bentley et al. [ | Dignity therapy followed by feedback questionnaire | Positive improvements in continuity of self and role preservation. | Preservation of identity | Autonomy |
| Sommers‐Spijkerman et al. [ | Survey and Interviews |
“Thanks to this app I think ‘What positive things happened today?’” Participants struggled to integrate the intervention into everyday life 10/13 (63%). |
Positive shift in attention Continuity |
Making life easier Accessibility |
| Wu et al. [ | Interviews |
Readjusting and them re‐learning” “wouldn't want them to bathe her” |
Consistency Privacy |
Ease of Use Autonomy |
| Author | Preference assessment | First order participant quotes/primary data from the studies. | Second order codes | Preference theme |
|---|---|---|---|---|
| Maier et al. [ | 5‐ and 11‐point Likert scale, Net Promoter Score (NPS) and interviews |
Key impacts include a sense of achievement (67%), reduced immobility (61%), and improved well‐being (55%). Symptom relief with reduced limb rigidity (63%) and muscle stiffness (52%). |
Improved quality of life Symptom relief | Making life easier |
| Author | Preference assessment | First order participant quotes/primary data from the studies. | Second order codes | Preference theme |
|---|---|---|---|---|
| Fidelix et al. [ | Teleconsultation followed by questionnaire |
4/36 (11%) patients disagreed that it was easy to set up The convenience of receiving assistance and maintenance of multidisciplinary care at home. |
Ease of set up Continuity of care |
Ease of Use Accessibility |
| Helleman et al. [ | Survey then interviews |
““Logging in is difficult with the digital ID” “You don't feel you are going for no good reason” Positive about receiving personalized feedback and information |
Log in issues Reducing the unnecessary Personalisation |
Ease of Use Making life easier Accessibility |
| James et al. [ | Survey then interviews | “It wouldn't take so much energy out of my life and I think my day would be a bit better” | Reducing the unnecessary | Making life easier |
| Hobson et al. [ | Questionnaire then interviews |
“Anything that makes life's journey, when necessary, better” 9/12 said they would use technology with the appropriate equipment and training. |
Making life easier Accessibility |
Making life easier Accessibility |
| Ando et al. [ | Telemonitoring for NIV for 24 weeks then interviews |
“It saves a lot of money as well as you know because I won't need to keep going to hospital” “The keyboard is that frustrating. I just couldn't be bothered trying to get it to work because it wouldn't.” |
Reducing the unnecessary Technical challenges |
Making life easier Safety and reliability |
| Helleman et al. [ | Survey |
86.1% were willing to record at least monthly and 60.7% at least weekly. Concerns with privacy, data security and data being sold to third parties. |
Low cognitive burden Technical reliability |
Accessibility Safety and reliability |
| Tattersall et al. [ | At home assessments via webcam then a survey |
Difficulty from mobility and speech issues Reducing the number of clinic visits was valuable in 24/25 of the pwALS |
Adaptability to MND Reducing appointments |
Accessibility Making life easier |
| Beswick et al. [ | Questionnaire |
Difficulty putting on the devices and faulty straps. Large size of the device affected their comfort Positive response that it meant less clinical appointments. |
Physical ability, Comfort Reducing appointments |
Ease of use Accessibility Making life easier |
- —National Institute for Health and Care Research10.13039/501100000272
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyotrophic Lateral Sclerosis Research · Neurogenetic and Muscular Disorders Research
Introduction
1
Understanding the preferences of patients towards treatments and interventions goes beyond assessing effectiveness; it evaluates the acceptability and desirability, revealing the underlying factors influencing adherence. Such insights can be used to adjust and tailor care to the wishes of the patient [1, 2]. Adopting this approach has consistently been shown to increase treatment satisfaction and adherence, and ultimately improve patients' quality of life [3].
In many conditions without a cure, the focus of care is improving quality of life. Patient‐centered care allows healthcare interventions to consider individual needs, bringing about meaningful improvements to life [4, 5]. The treatments for amyotrophic lateral sclerosis (ALS) encompass both disease‐modifying and symptomatic approaches [6]. Disease‐modifying drugs vary in efficacy, administration, side effects, and cost [7]. Global regulatory differences further complicate treatment availability [8]. As disease‐modifying treatments offer only modestly effective benefits in altering the disease's progression, optimizing quality of life remains central to ALS care [9, 10]. Beyond drug therapies, nutritional support, psychosocial care, physiotherapy, and assistive equipment (including communication aids and respiratory support) are crucial for managing symptoms and enhancing quality of life [11]. Digital health tools are also increasingly used to improve care accessibility and remote monitoring of the disease [12, 13].
It is particularly important to measure preferences in ALS as treatment and intervention options are complex and may require trade‐offs between quality of life and treatment burden [14]. As more treatments and interventions are developed, it becomes increasingly important to ensure the preferences of people with ALS (pwALS) are taken into account [15]. This review synthesizes existing evidence around what is important to pwALS for ALS treatments and interventions, and their characteristics.
Materials and Methods
2
Information Sources and Search Strategy
2.1
The study protocol was registered on PROSPERO [CRD42024526017].
The search strategy used free‐text and thesaurus search terms for:
(i) Motor Neuron(e) Disease and Amyotrophic Lateral Sclerosis (ii) Preferences, willingness to pay, attitudes towards, decision making, experiences, expectations, satisfaction, perceptions, perspectives (iii) Drug, medication, treatment, intervention, disease modification, symptom management, service, healthcare.
A single search was conducted in PubMed, Scopus, CINAHL and PsychINFO in which search terms (i), (ii) and (ii) were combined using “AND” to identify articles regarding preferences in people with ALS. Backward citation searching was also conducted. Initial searches were carried out in April 2024 and re‐run in September 2024. An information specialist supported the development of the search strategy and choice of databases.
Due to international inconsistency in terminology, searches have been conducted for both the terms motor neuron disease (MND) and amyotrophic lateral sclerosis (ALS). Searches were conducted from 2011 onwards to build on a previous review [16] and systematically search current literature that has not yet been synthesized. Full inclusion and exclusion criteria can be found in the Supporting Information (Table A1).
Data Collection Process
2.2
All references obtained from the various databases were uploaded and duplicates removed [17]. One author (AC) conducted a two‐stage screening process. First, titles and abstracts were assessed against the established inclusion/exclusion criteria. Second, the eligibility of relevant studies was determined by reading the full manuscripts. Any uncertainties were resolved by discussion among the authors. Rayyan was used as an online organizational tool, facilitating the sorting of citations. The stages of screening are reported in alignment with the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA 2020) statement [18]. Studies that met all aspects of full text screening were included for review for data extraction, synthesis, and critical review.
Data Extraction
2.3
Data extraction follows a framework and extracted data is displayed in tabular forms focusing on: (1) Publication details (2) Type of study (3) Study sample (4) Study characteristics and (5) study outcomes.
Data Synthesis
2.4
A mixed methods synthesis was conducted to integrate the findings from all the studies. Reflexive thematic analysis was conducted systematically and iteratively on the qualitative data [19]. Line‐by‐line open coding was conducted on the extracted data, identifying initial codes related to patient preferences (AC). The codes were then reviewed and grouped into broader categories, looking for patterns and relationships between them (all authors). This process involved multiple rounds of discussion and refinement, with each reviewer independently analyzing the coded data and then comparing their interpretations. Discrepancies were resolved through discussion until consensus was reached. Numerical quantitative data was extracted and then synthesized using a narrative summary approach due to the heterogeneity across studies in terms of outcome measures and study designs [20]. Where possible, numerical data on preferences were presented to highlight trends. Both qualitative and quantitative data from mixed‐methods studies were fully extracted using one of the above processes to ensure a comprehensive understanding of the preferences [21]. The integration of qualitative and quantitative findings was conducted using a data‐based convergent synthesis approach [22].
Quality Assessment
2.5
The quality of each study was assessed by AC using the Mixed Method Appraisal Tool (MMAT) [23]. The MMAT was used to assess the methodological quality of included studies, evaluating their research questions, data collection, analysis methods, no response bias (for quantitative studies) or rationale for the mixed methods approach (for mixed methods studies). A second reviewer (AWG) assessed 15.5% of the studies for inter‐rater reliability and to discuss any discrepancies. A sensitivity analysis was then performed.
Results
3
A total of 4240 papers were identified in searches across 4 databases and through backward citation searching. Of these, 77 papers were included after title/abstract screening, and 44 papers were included in the review (See Figure 1).
PRISMA showing the flow of papers during screening for the systematic review on the preferences of people with amyotrophic lateral sclerosis (ALS) towards ALS interventions.
A well‐defined categorization of treatments and interventions in ALS includes drug treatments, nutrition, special equipment, psychosocial support, physiotherapy, exercise programmes, and mobility aids [11]. This framework was used to classify studies and, within each category, subcategories were created to further explore findings. This resulted in the following: (1) drug treatments (symptom management and disease modifying) (2) nutrition, (3) special equipment, (4) psychosocial support, (5) exercise programmes. Additionally, a sixth intervention type was introduced: (6) digital health, encompassing telehealth, telecare, and telemonitoring.
The number of articles published per treatment type shows the highest number of studies were of specialist equipment (n = 16). Two papers report on both nutrition (percutaneous endoscopic gastrostomy (PEG)) and respiration (non‐invasive ventilation (NIV)) studies within a single paper [24, 25] (See Figure 2). There were 19 quantitative studies, 15 qualitative studies, and 10 mixed methods studies. Studies were conducted across seven countries in Europe (n = 25), two countries in North America (n = 9), across two countries in Australasia (n = 1) and in South America (n = 1) and Asia (n = 1). Some studies were conducted across multiple locations. Details regarding the characteristics of the studies can be found in the Supporting Information (Table A2).
Number of articles published per category of intervention.
Eight quantitative studies did not achieve a representative sample of the target MND population, due to a small sample, only recruiting from one ALS clinic and/or only including participants who had accepted/refused a treatmentt [25, 26, 27, 28, 29, 30, 31, 32]. There are concerns about generalization to a wider MND population due to the limited diversity in characteristics of participants. Nine studies had unjustified low response rates, risking non‐response bias due to potential systematic differences between participants and non‐participants [27, 28, 30, 31, 32, 33, 34, 35, 36]. For more details and the complete MMAT see Supporting Information (Table A3).
The results are presented by treatment/intervention categories: drugs, nutrition, special equipment, psychosocial support, exercise programmes, and digital health. Findings from the review are described under these categories using the themes/subthemes extracted from thematic analysis (See Figure 3). Not all themes/subthemes apply to each treatment/intervention as their relevance reflects the treatment/intervention goals.
Thematic analysis map of the identified preferences across treatment categories.
Drugs
3.1
Ease of Use
3.1.1
Most pwALS recruited from four European countries faced challenges in swallowing riluzole that led to treatment delays or omissions (Table 1). These people had the strongest preference for a new formulation with an easier mode of delivery that dissolved quickly on the tongue and had convenient/portable packaging [37]. Similarly, an implanted drug delivery device (IDDD) was considered to be a preferred alternative to a lumbar puncture for intrathecal therapy by pwALS in multiple clinical settings in the US and Europe, due to it being perceived as an easier mode of delivery [38]. PwALS valued a shorter duration and less frequent administration of the treatment [38]. Despite a general acceptance of edaravone, 22/331 (6.6%) participants voluntarily suspended this potential disease‐modifying drug treatment due to the burden of the intravenous route of administration [33].
Difficulties were expressed with the range of syringes available for the injection of methylcobalamin, a form of vitamin B12 with limited evidence of potential slowing of functional decline in ALS. It was reported “It would be good to have a standard syringe, because otherwise, you have to learn every time” [39]. A single ALS centre observed the use of PB‐TURSO, a combination of sodium phenylbutyrate (PB) and taurursodiol (TURSO) for the disease modification of ALS. The study observed a high discontinuation rate due to gastrointestinal side effects 17/29 (58.6%) and the drug's taste 8/29 (27.6%) [34].
The ease of administration is also important to pwALS when receiving drug treatments to manage the symptoms of their ALS. Almost all people with ALS were satisfied with the effectiveness of tetrahydrocannabinol and cannabidiol (THC:CBD) for treating symptoms of spasticity, but a third reported issues with the ease of administration of the oromucosal spray, highlighting the way this restricts usability [40].
Accessibility
3.1.2
PwALS express the importance of affordability in deciding whether to start or continue a drug treatment. “Riluzole is too expensive. If it is cheaper, I would try it” [41]. Similar concerns were expressed regarding vitamin B12 injections, where “The cost poses a barrier to how often I take the [vitamin B12] shots now.29”.
Safety/Reliability
3.1.3
Almost all pwALS reported a low risk of choking as the leading factor when choosing a drug formulation [37]. For the intrathecal delivery of drugs, pwALS valued a low risk from the drug administration and low frequency of administration. There was a preference for an IDDD compared to a lumbar puncture, although participants in this survey were only willing to accept a low risk of device failure to be able to switch from lumbar puncture to an IDDD [38].
Nutrition
3.2
Autonomy
3.2.1
Five studies found the loss of control and social enjoyment at mealtimes formed barriers to accepting PEG [24, 25, 42, 43, 44] (Table 2). One participant “wanted to continue to eat independently, no matter how difficult it was.” [25].
Making Life Easier
3.2.2
When food preparation [45] and eating [42, 43] became challenging and less enjoyable, individuals were more inclined to accept PEG to simplify life. One participant explained, “My main reason for getting the PEG was my swallowing,” highlighting issues with choking and aspiration as key factors in the decision, along with the belief that it would improve quality of life [46].
Special Equipment
3.3
Ease of Use
3.3.1
When receiving non‐invasive ventilation (NIV) the sensation of air being blown into the mask at high pressure was described as “too powerful” and difficulties were reported with wearing glasses or maintaining physical closeness with partners [47] (Table 3). Participants highlighted challenges with mask adjustment, particularly with clips, stating, “I can get the mask on… but I can't, it's the clips” [47]. In contrast, the simplicity of using a cough assist was positively anticipated: “It is not very complicated either. I think that will be important” [26].
Keeping hospital admission to a minimum was important when considering a brain computer interface, as 44/61 (72%) would accept surgically implanted electrodes with outpatient surgery, but willingness decreased to 25/61 (41%) if it involved a hospital stay [27]. This finding underscores a strong preference for procedures that are minimally disruptive to day‐toto‐day life.
Accessibility
3.3.2
The lack of adaptability of many assistive technologies to the specific needs of ALS was a barrier to use [50]. 89/179 (49.7%) pwALS report the application process for assistive technology and home adaptations as a key barrier [51]. Among users of augmentative and alternative communication (AAC) devices, high insurance co‐payments prevented 5/174 (2.9%) of pwALS from using these devices [29].
Autonomy
3.3.3
Many pwALS expressed a preference for low dependence on non‐invasive ventilation (NIV). One participant explained “I wouldn't want it to be all of the time and not have any life” [48]. However, as this sample included only participants who had declined NIV, these preferences may reflect unique perspectives on autonomy among this group. Assistive home devices were valued due to their ability to maintain and retrieve autonomy as “it would be great if it could also disburden somebody” and allow for more independence [50]. Voice banking was a preferred means of preserving personal identity and retaining autonomy in personal life choices [53, 54]. Additionally, communication aids were favored for their role in reducing isolation and supporting independent communication [52].
Safety/Reliability
3.3.4
PwALS expressed a preference for NIV masks that function reliably: “It leaks just from the mask, it's not very good” [47]. Some participants said that the enclosed design of the mask could feel restrictive and potentially unsafe [48]. Cough assist devices were particularly valued for their reliability with one participant expressing “knowing that it is there” provided a sense of security for unpredictable needs [26]. PwALS desired eye‐tracking technology and brain‐computer interfaces (BCIs) to be both accurate and reliable [27, 29, 49]. One BCI paper showed 21/42 (50%) participants required there to be at least 80% accuracy while 38/42 (90.5%) would like the device to have 90% or higher accuracy [49]. PwALS showed little concern for the appearance of these devices [27]. There were safety concerns for home assistive devices, particularly regarding secure installation with one participant fearing that a ceiling‐mounted system might fall, and they would be unable to move to safety due to their ALS [50].
Psychosocial Support
3.4
Ease of Use
3.4.1
PwALS expressed a desire for continuity in care providers in respite care, emphasizing that frequent transitions required constant “readjusting and [caregivers] re‐learning,” which detract from the ease and enjoyment of the intervention [55] (Table 4).
Accessibility
3.4.2
Accessibility is a key preference in psychosocial support particularly inclusivity of the varied needs associated with ALS such as communication difficulties [56, 57]. Participants suggested practical improvements such as “having a therapist coming home would be very useful” and “text reminders, and written information” [56]. Ensuring the continued availability of psychological interventions at home following in‐person services is important as many participants struggled to integrate these interventions into their daily lives [59], with one noting, “At the beginning, it wasn't easy to do exercises at home exactly the way trainers taught us” [58].
Autonomy
3.4.3
Preserving independence and maintaining privacy was highly valued by individuals with ALS. This has been shown to exempt close families, with one participant explaining during respite care “I have trouble asking other people besides my husband to do things for me” [55]. Dignity therapy was positively received for its support of autonomy and found positive reports from the continuity of self, acceptance and role preservation [32].
Exercise Programmes
3.5
Making Life Easier
3.5.1
PwALS value exercise programs that enhance daily life such as through a sense of achievement, reduced immobility, and improved well‐being. Symptom relief was also significant, with reduced limb rigidity and muscle stiffness, along with improvements in flexibility, muscle preservation, sleep quality, and strength as key factors [60] (Table 5).
Digital Health Tools
3.6
Ease of Use
3.6.1
PwALS expressed a willingness to use teleconsultations and home monitoring but wanted these digital health tools to be straightforward and easy to operate [6, 36, 61] (Table 6).
Accessibility
3.6.2
PwALS appreciated having continued access to telehealth interventions as “If you've got a problem, no matter what time it is, you can type it in.” [65]. Simplified interfaces were preferred, as frustration and low usage were linked to difficulties using the messaging system and on‐screen keyboard of a telecommunication device, primarily due to reduced fine motor skills [64, 65]. Most participants reported a willingness to use the technology if it had appropriate adaptive equipment [64]. Additionally, 277/322 (86.1%) of participants were willing to record data at least monthly, with 195/322 (60.7%) willing to do so weekly, emphasizing the need for low‐burden tools that accommodate cognitive demands [66].
Making Life Easier
3.6.3
PwALS positively perceive digital health tools including videoconferencing and telemonitoring of NIV that reduces in person clinical appointments and thus avoids unnecessary costs [66]. This was a “life saver” [64] and participants found the convenience of digital tools beneficial for everyday life [61, 63, 64, 65, 67]. However, while these tools were appreciated, it was also acknowledged that pwALS may not want to become “trapped in the house” highlighting the importance of balancing remote care with opportunities for social engagement and mobility [63]. It was suggested to have initial face‐to‐face contact with the ALS clinic that is later changed to being delivered remotely.
Safety and Reliability
3.6.4
Although generally positive about movement‐evaluating devices, some people with ALS experienced charging problems that hindered use [61]. A preference for trustworthy technology was indicated as pwALS expressed concerns about privacy, data security, and the potential sale of personal data [66].
Discussion
4
Across six treatment and intervention categories, five overarching factors influenced preferences: ease of use, accessibility, making life easier, autonomy, and safety/reliability. Not all treatments addressed every theme or subtheme, likely reflecting the number of studies or the priorities of pwALS.
Ease of use is key for drug treatments in which the method and frequency of delivery were of greatest importance. PwALS showed an openness towards exploring and accepting new drugs and drug delivery methods even when effectiveness is unclear [37, 38, 40]. Similar findings are observed in Huntington's Disease (HD) and spinocerebellar ataxia (SCA) where the mode and frequency of administration significantly influenced preferences. For instance, respondents favored a single operation over repeated lumbar punctures [68] as was reported for the intrathecal delivery of ALS drugs [38]. There is increasing recognition of the value in involving views of people living with a disease or condition throughout the decision making of drug treatments development lifecycle [69]. Building on the attributes of ease of use, accessibility, and safety/reliability identified in this review, specific to drug studies, quantitative methods of preference elicitation, such as discrete choice experiments (DCEs), can be conducted. These methods can elicit preference data regarding specific levels of the attributes—for example, the preferred frequency of drug administration. These preferences can then be integrated into target product profiles (TPPs) to align drug development with the needs and values of pwALS.
The preference for ease of use extends beyond drug treatment to interventions such as communication aids [29, 52] and is closely linked to accessibility, both physically and cognitively. Accessibility is particularly important for pwALS and other progressive neurodegenerative diseases in whom mobility and function can rapidly decline and make traditional care difficult to implement [70]. Prioritizing both ease of use and accessibility ensures effective and continued care throughout disease progression.
Safety and reliability are important factors for pwALS and are recognized as fundamental requirements for quality healthcare [71]. The preference for safety is observed in multiple sclerosis (MS) clinics where patients taking injectable treatments placed the most concern on the risk of serious infection [72]. In contrast, a study investigating preferences for methods of delivering disease‐modifying drugs for HD and SCA found associated risks did not influence the preference for intrathecal drug delivery [68]. This suggests safety and reliability do not universally affect decision making in all neurodegenerative diseases and may be particularly important in ALS due to the fast progression and increased vulnerability of individuals. Reliable interventions are therefore critical to ensuring continuity of care and minimizing disruptions that could threaten life, independence, and increase caregiver burden.
This review builds on a previous systematic review on perceptions and preferences to services and care in ALS [16]. Both reviews highlight a consistent emphasis on the importance of continuity and accessibility in care, alongside interventions designed to preserve autonomy and support independence. These priorities have been particularly evident over time in the use of augmented and assisted communication (AAC) aids and home adaptations to facilitate daily living. A key distinction of this review is the broader range of treatment categories, including the preferences of pwALS for drug treatments, particularly disease‐modifying drugs. Available or experimental disease‐modifying drugs are constantly evolving, and it is important to understand patients' preferences and incorporate them into the development process. Collating these preferences will have significant implications for policy making and drug development and aid in the alignment of treatments with the needs and expectations of those living with ALS. This review also examines digital health tools and advanced methods like brain‐computer interfaces, highlighting the importance of technological reliability and accuracy in these novel interventions [27, 49, 61, 62]. The previous review shows most studies emanating from Europe and North America [16]. Whilst this remains true, underscoring a continued overreliance on the views of white, western populations, this review includes more global distribution, with research from Europe, North America, Australasia, and some studies from South America and Asia. This wider geographic scope suggests a broader effort to understand ALS treatment preferences across diverse populations.
Different healthcare systems offer varying levels of access to diagnosis, treatment, supportive care, and end‐of‐life services for people with ALS due to differences in resources, regulatory bodies, and the configurations of healthcare systems [73]. Financial factors often influence treatment decisions, sometimes leading to cost‐driven choices or non‐adherence. This impact is greater in market‐based systems like those in the USA [41], China [40], and Germany [30] compared to systems like the UKs, where care is free at the point of access. However, some pwALS may choose cheaper treatment options due to insufficient information provided by health care professionals (HCPs) regarding the availability of patient assistance programs and other mechanisms to reduce out‐of‐pocket drug costs. Increased access to this information could in turn broaden treatment choices. Similarly, differences in understanding of treatment implications can influence preferences. For example, while HCPs understand that introducing a PEG doesn't necessarily prevent pleasure from oral intake of food, some patients still report “wanting to eat independently, no matter how difficult” as a reason to avoid having a PEG [25]. This difference may stem from insufficient support for patients in understanding the consequences of their treatment choices.
Limitations
4.1
The review lacks comparative data of preferences within treatment and intervention types, limiting the reliability of findings. Some studies had biased sampling, focusing on participants with similar views e.g., all who accepted or declined an intervention before a user experience assessment [25, 29, 48]. This excludes views from differing perspectives, potentially reducing the generalisability of the results.
The preferences of pwALS reported in this review reflect the context of treatment at the time of data collection. Given the rapid evolution of ALS interventions, some preferences may no longer reflect current treatment realities. For example, while intravenous administration was a key reason for edaravone discontinuation, the more recent approval of an oral formulation may invalidate this. Similarly, PB‐TURSO discontinuation due to gastrointestinal side effects and taste is no longer applicable as the drug has been withdrawn from the US and Canadian markets and was never approved in Europe. However, these results still emphasize the preference of pwALS for less invasive modes of delivery and fewer disruptive side effects, and show consistencies that can be applied across different treatments.
Future Directions
4.2
The themes identified in this review can inform the attributes of discrete choice experiments (DCEs) to be used in the development of future preference‐based measures. Systematically varying the levels of these attributes in a DCE elicits quantitative measures of preferences. This approach enables a deeper understanding of the relative importances of different treatment characteristics and the trade‐offs pwALS are willing to make. Importantly, this can inform health care policy of the specific values of pwALS to optimize resource allocation and tailor clinical practice.
Conclusions
5
This systematic review across six intervention categories—drug treatments, nutritional support, special equipment, psychosocial support, exercise programmes, and digital health—revealed the key factors influencing preference decisions as: ease of use, accessibility, making life easier, autonomy, and safety/reliability. While not every theme emerged in every category, reflecting the distinct goals of different interventions (e.g., symptom management vs. disease progression), the consistent emergence of these themes across varied treatment types suggests fundamental, underlying values in ALS care that transcend specific treatment goals and modalities. These findings provide researchers, clinicians, and policymakers with evidence to inform practical, patient‐centered decisions regarding ALS treatments and interventions. Integrating patient preferences in clinical practice promotes patient‐centered care, which increases patient satisfaction and treatment effectiveness [74].
Author Contributions
A. Clift: investigation, writing – original draft, methodology, writing – review and editing, formal analysis. D. Rowen: conceptualization, funding acquisition, investigation, methodology, formal analysis, supervision, writing – review and editing. L. Knox: investigation, methodology, supervision, formal analysis, writing – review and editing. A. W. Griffiths: investigation, methodology, supervision, formal analysis, writing – review and editing. C. J. McDermott: conceptualization, investigation, funding acquisition, methodology, supervision, writing – review and editing.
Ethics Statement
We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. F. P. Bridges , E. W. de Bekker‐Grob , B. Hauber , et al., “A Roadmap for Increasing the Usefulness and Impact of Patient‐Preference Studies in Decision Making in Health: A Good Practices Report of an ISPOR Task Force,” Value in Health 26, no. 2 (2023): 153–162, 10.1016/j.jval.2022.12.004.36754539 · doi ↗ · pubmed ↗
- 2M. Tringale , G. Stephen , A. M. Boylan , and C. Heneghan , “Integrating Patient Values and Preferences in Healthcare: A Systematic Review of Qualitative Evidence,” BMJ Open 12, no. 11 (2022): e 067268, 10.1136/bmjopen-2022-067268.PMC 967701436400731 · doi ↗ · pubmed ↗
- 3Y. Bombard , G. R. Baker , E. Orlando , et al., “Engaging Patients to Improve Quality of Care: A Systematic Review,” Implementation Science 13, no. 1 (2018): 98, 10.1186/s 13012-018-0784-z.30045735 PMC 6060529 · doi ↗ · pubmed ↗
- 4K. Megari , “Quality of Life in Chronic Disease Patients,” Health Psychology Research 1, no. 3 (2013): e 27, 10.4081/hpr.2013.e 27.26973912 PMC 4768563 · doi ↗ · pubmed ↗
- 5F. Riecke , L. Bauer , H. Polzer , et al., “Effects of Medical Interventions on Health‐Related Quality of Life in Chronic Disease—Systematic Review and Meta‐Analysis of the 19 Most Common Diagnoses,” Frontiers in Public Health 12 (2024): 1313685, 10.3389/fpubh.2024.1313685.38379671 PMC 10878130 · doi ↗ · pubmed ↗
- 6C. J. Mc Dermott and P. J. Shaw , “Diagnosis and Management of Motor Neurone Disease,” British Medical Journal 336, no. 7645 (2008): 658–662, 10.1136/bmj.39493.511759.BE.18356234 PMC 2270983 · doi ↗ · pubmed ↗
- 7E. Harvey , “Motor Neurone Disease: Management of Common Symptoms,” Pharmaceutical Journal 14 (2019): 34, 10.1211/pj.2019.20205952. · doi ↗
- 8A. Chiò , L. Mazzini , and G. Mora , “Disease‐Modifying Therapies in Amyotrophic Lateral Sclerosis,” Neuropharmacology 167 (2020): 107986, 10.1016/j.neuropharm.2020.107986.32062193 · doi ↗ · pubmed ↗