Translation and cross-cultural adaptation of the Brazilian version of the Boston Residue and Clearance Scale (BR-BRACS)
Giulia Beatriz Pozena Scaranelo, Suely Mayumi Motonaga Onofri, Leandro de Araújo Pernambuco, Roberta Gonçalves da Silva, Giulia Beatriz Pozena Scaranelo, Suely Mayumi Motonaga Onofri, Leandro de Araújo Pernambuco, Roberta Gonçalves da Silva

TL;DR
This study translated and adapted the Boston Residue and Clearance Scale into Brazilian Portuguese and validated its image content for evaluating swallowing.
Contribution
The paper provides a validated Brazilian Portuguese version of the BR-BRACS scale with culturally adapted images for pharyngeal residue assessment.
Findings
The translation and cross-cultural adaptation of BR-BRACS was successfully completed with content validity evidence.
Images for the scale showed near-perfect agreement among judges in visual-perceptual evaluation.
Discrepancies in translation were resolved through consensus, ensuring equivalence with the original version.
Abstract
This study aimed to translate and cross-culturally adapt The Boston Residue and Clearance Scale (BR-BRACS) into Brazilian Portuguese and validate the image selection content for the scale. The project was approved by the Institution’s Ethics Committee under number 67715717.6.0000.5406. The process involved translating the scale into the target language, synthesizing the translations, and back-translating it into the original language. A literature review was conducted to define the concept of pharyngeal residue and ensure the content validity of the images representing the scale. Then, 50 fiberoptic endoscopic evaluations of swallowing were analyzed and submitted to three judges for visual-perceptual evaluation. Agreement among the judges was analyzed using Fleiss' Kappa test with a 95% confidence interval. Discrepancies in lexical and syntactic contexts were identified during…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
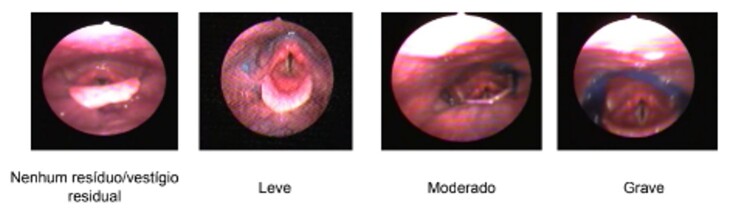 Figure 1
Figure 1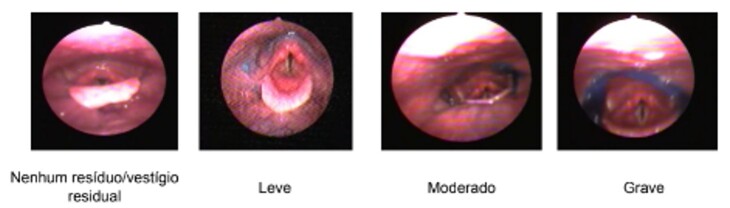 Figure 2
Figure 2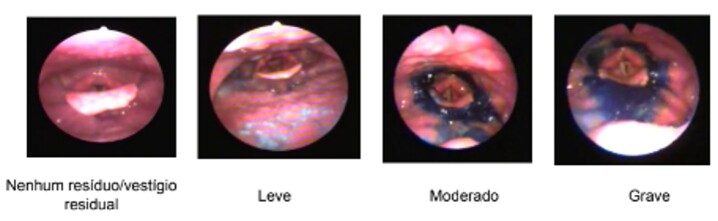 Figure 3
Figure 3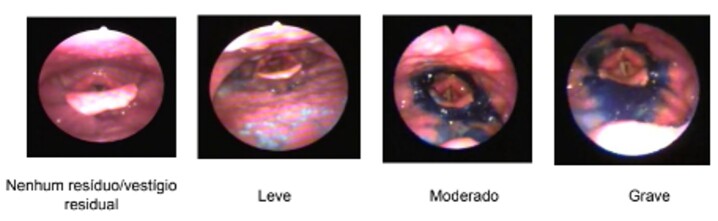 Figure 4
Figure 4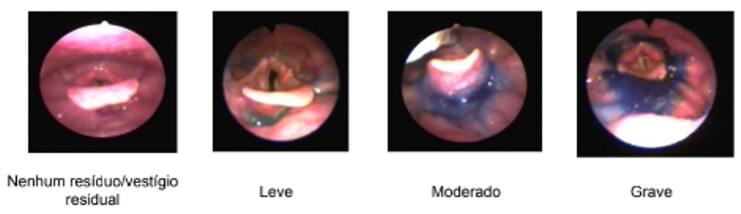 Figure 5
Figure 5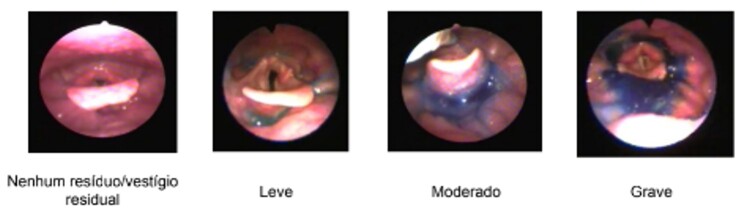 Figure 6
Figure 6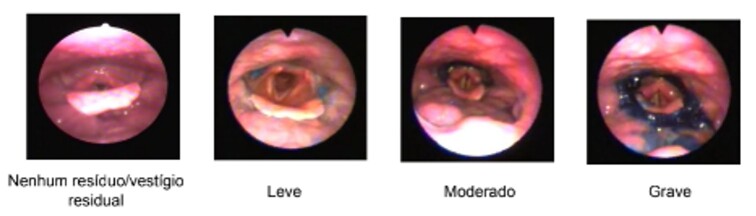 Figure 7
Figure 7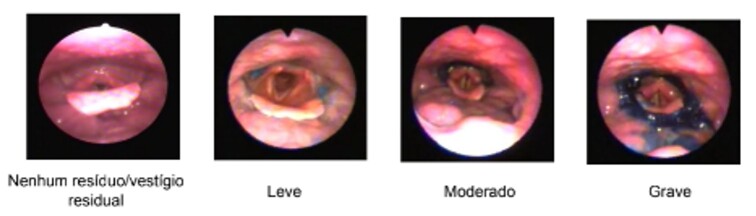 Figure 8
Figure 8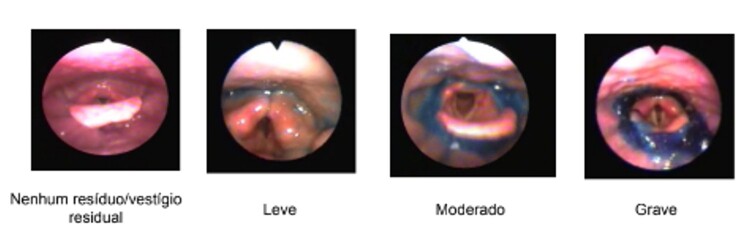 Figure 9
Figure 9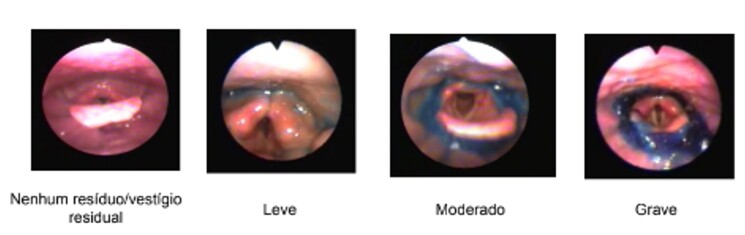 Figure 10
Figure 10| BRACS | T1 | T2 | T1/T2 |
|---|---|---|---|
|
| Localização e quantidade de | Localização e quantidade de | Localização e quantidade de resíduos |
|
| Marque todos os locais que se aplicam | ||
|
| E, em seguida, indique a pior pontuação obtida em cada um deles | ||
|
|
|
| Região 1 |
|
| Parede lateral da faringe | Parede lateral da faringe | Parede lateral da faringe |
|
| Parede posterior da faringe | Parede posterior da faringe | Parede posterior da faringe |
|
| Base da língua | Base da língua | Base da língua |
|
| Valéculas | Valéculas | Valéculas |
|
| Ponta da epiglote | Ponta da epiglote | Ponta da epiglote |
|
|
|
| Região 2 |
|
| Canal lateral esquerdo e recesso piriforme esquerdo | Canal lateral esquerdo e recesso piriforme esquerdo | Canal lateral esquerdo e recesso piriforme esquerdo |
|
| Canal lateral direito e recesso piriforme direito | Canal lateral direito e recesso piriforme direito | Canal lateral direito e recesso piriforme direito |
|
| Região pós-cricóidea | Região pós-cricóidea | Região pós-cricóidea |
|
|
|
| Bolus alimentar 1 |
|
| Nenhum/ | Nenhum | Nenhum resíduo/vestígio residual |
|
|
|
| Leve |
|
| Moderado | Moderado | Moderado |
|
|
|
| Grave |
| PARAGRAPH | T1 | T2 | T1/T2 |
|---|---|---|---|
|
| A BRACS é uma escala ordinal de 11 pontos | A BRACS é uma escala ordinal de 11 pontos | A BRACS é uma escala ordinal de 11 pontos que mensura o grau de comprometimento de resíduos faríngeos |
|
| Essa escala | A escala | A escala determina, em específico, a quantidade de resíduos faríngeos |
|
| Nenhum resíduo/vestígio residual | Nenhum resíduo/vestígio residual | Nenhum resíduo/vestígio residual |
|
| Leve = | Leve = | Leve = resíduos cobrindo/preenchendo <1/3 do local |
|
| Moderado = | Moderado = | Moderado = Resíduos cobrindo/preenchendo 1/3 – 2/3 do local |
|
| Grave = | Grave = | Grave = resíduos cobrindo/preenchendo >2/3 do local |
|
| A quantidade de resíduos é pontuada | A quantidade de resíduos é pontuada em 12 | A quantidade de resíduos é pontuada considerando 12 locais na laringofaringe |
|
|
|
| Se houver resíduos em quatro ou mais regiões anatômicas, adicione um ponto à somatória |
|
|
|
| Se houver resíduos no interior do vestíbulo, colocando o indivíduo em maior risco de aspiração após a deglutição, adicione um ponto à somatória |
|
| Se | Se | Se houver resíduos e o indivíduo não manifestar deglutições espontâneas, adicione um ponto à somatória, considerando que, aparentemente, existe a falta de sensação faríngea |
|
|
|
| Por fim, as deglutições espontâneas ou estimuladas são, então, julgadas quanto a sua eficiência |
|
| Sim ( | Sim = | Sim = limpeza de 80-100% dos resíduos |
|
| Parcialmente | Parcialmente = | Parcialmente = limpeza de 20-80% dos resíduos |
|
| Não ( | Não = | Não = limpeza de 0-20% dos resíduos |
| BRACS | B1 | B2 | B1/B2 |
|---|---|---|---|
| 1.Localização e quantidade de resíduos |
|
|
|
| 2.Marque todos os locais que se aplicam |
|
|
|
| 3.e, em seguida, indique a pior pontuação obtida em cada um deles |
|
|
|
| 4.Região 1 |
|
|
|
| 5.Parede lateral da faringe |
|
|
|
| 6.Parede posterior da faringe |
|
|
|
| 7.Base da língua |
|
|
|
| 8.Valéculas |
|
|
|
| 9.Ponta da epiglote |
|
|
|
| 10.Região 2 |
|
|
|
| 11.Canal lateral esquerdo e recesso piriforme esquerdo |
|
|
|
| 12.Canal lateral direito e recesso piriforme direito |
|
|
|
| 13.Região pós- cricóide |
|
|
|
| 14.Bolus alimentar 1 |
|
|
|
| 15.Nenhum resíduo/vestígio residual |
|
|
|
| 16.Leve |
|
|
|
| 17.Moderado |
|
|
|
| 18.Grave |
|
|
|
| PARAGRAPH | B1 | B2 | B1/B2 |
|---|---|---|---|
| 1.A BRACS é uma escala ordinal de 11 pontos que mensura o grau de comprometimento de resíduos faríngeos |
|
|
|
| 2.A escala determina, em específico, a quantidade de resíduos faríngeos |
|
|
|
| 3.Nenhum resíduo/vestígio residual |
|
|
|
| 4.Leve = resíduos cobrindo/preenchendo <1/3 do local |
|
|
|
| 5.Moderado = Resíduos cobrindo/preenchendo 1/3 – 2/3 do local |
|
|
|
| 6.Grave = resíduos cobrindo/preenchendo >2/3 do local |
|
|
|
| 7.A quantidade de resíduos é pontuada considerando 12 locais da laringofaringe |
|
|
|
| 8.Se houver resíduos em quatro ou mais regiões anatômicas, adicione um ponto à somatória |
|
|
|
| 9.Se houver resíduos no interior do vestíbulo, colocando o indivíduo em maior risco de aspiração após a deglutição, adicione um ponto à somatória |
|
|
|
| 10.Se houver resíduos e o indivíduo não manifestar deglutições espontâneas, adicione um ponto à somatória, considerando que, aparentemente, existe a falta de sensação faríngea |
|
|
|
| 11.Por fim, as deglutições espontâneas ou estimuladas são, então, julgadas quanto a sua eficiência |
|
|
|
| 12.Sim = limpeza de 80-100% dos resíduos |
|
|
|
| 13.Parcialmente = limpeza de 20-80% dos resíduos |
|
|
|
| 14.Não = limpeza de 0-20% dos resíduos |
|
|
|
- —CAPES
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDysphagia Assessment and Management · Stuttering Research and Treatment · Child Nutrition and Feeding Issues
INTRODUCTION
Healthcare assessment, whether clinical or through various examinations, requires reliable procedures, protocols, and scales with diagnostic accuracy. Regarding the diagnosis of swallowing disorders, assessment instruments with scales that measure the degree of impairment are important for understanding the levels of dysfunction in swallowing biomechanics and analyzing the nature and prognosis of the condition at any point during patient care. These instruments, whether clinical evaluations or instrumental exams, are complementary and provide excellent feedback tools for families and patients. Additionally, they are part of a set of markers that assist professionals in clinical decision-making^(1,2)^.
Pharyngeal residues (PR) in oropharyngeal dysphagia are a risk marker for laryngotracheal aspiration. Although various scales exist for analyzing PR, they were predominantly published in American English and are mostly designed to classify PR in videofluoroscopic swallowing studies (VFSS)^(3-5)^. Only a few scales are available for analysis using fiberoptic endoscopic evaluation of swallowing (FEES)^(6-8)^. The Boston Residue and Clearance Scale (BRACS) is one of the scales available to enhance PR analysis via FEES – an excellent instrumental examination for evaluating this finding – and measure the levels of impairment associated with PR.
Translating and adapting PR classification scales into Brazilian Portuguese is essential to enhance diagnosis and clinical decision-making based on internationally recognized markers. Thus, this study aimed to translate and cross-culturally adapt the BR-BRACS into Brazilian Portuguese and validate the image selection content for the scale.
METHODS
This study was approved by the Research Ethics Committee (CEP) under protocol number 67715717.6.0000.5406. To initiate the study, the primary author of the instrument was contacted via email and granted authorization for its use. The BRACS is an 11-point ordinal scale divided into 12 locations with four classifications of residue quantity (none/coating, mild, moderate, and severe). The identified residue locations are divided into two regions: Region 1 includes the lateral pharyngeal wall, posterior pharyngeal wall, base of tongue, valleculae, and tip of epiglottis; Region 2 includes the left lateral channel and left piriform recess, right lateral channel and right piriform recess, and the postcricoid region. The scale's scoring is based on the presence of residue in one or more locations and ultimately classifies swallowing efficiency based on stimulated or spontaneous swallows to clear the residue^(7)^.
BR-BRACS’ translation and cross-cultural adaptation followed the six-stage method by Beaton et al.^(9)^. This study phase carried out the first three stages – (1) Translation into the target language, Brazilian Portuguese; (2) Synthesis of the translations; and (3) Back-translation into the original language, American English, as described below:
Stage 1 – Translation into the target language: Brazilian Portuguese
Two translators experienced in scientific healthcare translations, including other oropharyngeal dysphagia instruments, translated the scale from its original language (American English) into Brazilian Portuguese. The selection criteria for the translators were being native Brazilian speakers, fluent in the original language of the instrument, and experienced in healthcare translations. The translators had an average of 9 years of experience in the field and met all criteria. After being contacted, they were sent the file containing an instruction paragraph and the BRACS via email, with a 1-week deadline for translation. Each translator completed the translation independently, resulting in two versions (T1 and T2).
The instruction paragraph for using and scoring the BRACS was translated as part of the process. This paragraph was extracted from the original article and divided into 14 segments, sent to the translators for them to translate. After completing the translations, the paragraph and the scale proceeded to Stage 2.
Stage 2 – Synthesis of the translations
The research committee, comprising the authors (with an average of 15 years of experience in the field of the translated instrument) and the two translators from Stage 1, held an online meeting to resolve lexical and syntactic discrepancies and create a consensus version (T1+T2) in Brazilian Portuguese. The meeting, held via Google Meet, was the first time the translators reviewed their translations together. Adjustments were made by consensus among the translators and the study authors, comparing the consensus version with the original text to identify the best equivalent terms commonly used in the specialty field in Brazilian Portuguese.
Stage 3 – Back-translation into the original language (North American English) and cross-cultural adaptation
Two native English-speaking translators fluent in Brazilian Portuguese back-translated the Brazilian Portuguese consensus version (T1+T2) into the instrument’s original language (American English). After this process, any discrepancies in the back-translated version were discussed in a consensus meeting between the translators and researchers, resulting in the final version.
At the end of the stage, it was decided to compare the consensus version with the original version based on the translators’ and study authors’ suggestions, finding no disagreements.
The authors defined the following concepts for results analysis: syntactic adaptation as the set of rules allowing different word options and associations to form sentences – i.e., how the terms in a sentence relate to one another; semantic adaptation as the equivalence of same-meaning words in American English and Brazilian Portuguese; and grammatical adaptation as the set of rules for the correct use of written and spoken language.
Three procedures were performed for the content validity evidence of the images selected to represent the original scale’s levels, following the recommendations of the Standards for Educational and Psychological Testing (2014)^(10)^. The initial procedure was a literature review to establish the operational definition of the term “pharyngeal residue.”
The second procedure was a visual-perceptual evaluation of 50 examinations of individuals with neurological etiologies from an image database at a reference center for the diagnosis of oropharyngeal dysphagia. These exams were randomly analyzed by the author of this study. From this analysis, 24 images were selected to represent six PR locations, divided into Region 1 (lateral pharyngeal wall, posterior pharyngeal wall, base of tongue, valleculae, and tip of epiglottis) and Region 2 (left lateral channel and left piriform recess, right lateral channel and right piriform recess, and postcricoid region). The images were also categorized into four levels of severity (no residue/residual coating; mild; moderate; and severe).
The third procedure was the visual-perceptual evaluation by three additional judges experienced with the examination. They answered a structured questionnaire indicating whether they “agreed,” “disagreed,” or had any suggestions for each selected image and location. The agreement among the judges was analyzed using Fleiss' Kappa test with a 95% confidence interval (95% CI).
RESULTS
The results were presented in three stages. The first stage (S1) focused on the translation process and the instructions for using the scale, the second stage (S2) addressed the back-translation process, and the third stage (S3) covered the content validity of the images.
In S1, the 18 BRACS segments were divided for analysis. Nine had been translated identically, and nine diverged between T1 and T2. The consensus version maintained one of the nine discrepant segments as in T1, five as in T2, and the remaining ones were adjusted by consensus between the translators. The adjustments were made by comparing with the original version, aiming for the best equivalent term commonly used in Brazilian Portuguese. The results are detailed in Table 1.
Also, in S1, only one of the 14 segments in the instruction paragraph was translated identically between T1 and T2, while the other 13 diverged. These discrepancies were categorized as a) semantic, b) syntactic, and c) grammatical and were resolved by consensus, as shown in column 3 of Table 1.
In S2, Table 2 presents the BRACS translation, detailing the translation of 18 segments from American English into Brazilian Portuguese.
In the BRACS back-translation stage, 18 segments were back-translated from Brazilian Portuguese to American English, as shown in Table 3. Of the total segments, 11 were translated in agreement between B1 and B2, while seven diverged. One of the latter was adjusted to align with B1, and six were adjusted to align with B2. Discrepancies were resolved in the consensus version, as shown in the same table.
The back-translation of the instruction paragraph had the same number of agreements and discrepancies as in the translation. B1 and B2 agreed in only one segment and diverged in the remaining 13, as shown in Table 4. Discrepancies were resolved in the consensus version, shown in the same table.
After completing this stage, following the translators' suggestions and the study authors' decision, the back-translated BRACS was compared with the original version to confirm the equivalencies. This process was carried out in an online meeting, discussing semantic and grammatical issues related to the anatomy of the regions in question; no discrepancies were found.
Lastly, S3 addressed the content validity results for the selection of images. The agreement among the judges was 0.958, with a confidence interval of 0.051 and 0.036, suggesting almost perfect agreement between them. The judges had three discrepancies in Regions 1 and 2 concerning the locations and severity levels, as follows: Lateral pharyngeal wall and posterior pharyngeal wall – Mild; Valleculae and the tip of epiglottis – Moderate; Postcricoid region – Moderate.
Regarding the first location discrepancy, one judge suggested that the chosen image represented the lateral pharyngeal wall, rather than both the lateral and posterior pharyngeal walls. In the second location discrepancy, valleculae and the tip of epiglottis, another judge recommended including more images of the tip of epiglottis to better differentiate severity levels (mild and severe). Lastly, the judges commented on the difficulty in assessing the severity level from the static postcricoid image, leading to uncertainty between moderate and severe. The authors considered the discrepancies and maintained by consensus the selected images as representative of the severity levels.
The images agreed on to represent each region and level as previously proposed in the BR-BRACS are displayed in Appendix A.
DISCUSSION
A simple literature review can easily detect the scarcity of tools to assess and classify the degree of impairment in oropharyngeal dysphagia with evidence of validity and developed in Brazilian Portuguese. The translation and adaptation of an instrument available in another language is often a solution to this problem, provided it follows an appropriate method^(11)^. Moreover, the translation process varies considerably in guidelines and recommendations, and many authors adapt the stages by combining one or more methods^(12-15)^.
Semantic and syntactic divergences in translation and back-translation are common. In the case of the BR-BRACS, they were more frequent in the translation of the instruction paragraph than in the scale itself. This issue is easily understood when compared with other translations of scales based on anatomical regions, as discrepancies are rarely found in human anatomy terms^(16-18)^. Translations of longer sentences are more likely to present divergences, as also noted in other translation studies, whose authors reported difficulties in analyzing semantic, idiomatic, conceptual, linguistic, and contextual discrepancies^(19-25)^.
In addition to sentence length and its impact on translations with syntactic divergences, there were semantic issues related to the correct healthcare terms. This technical aspect of translations, as highlighted in other studies, often arises due to cross-cultural adaptation – e.g., translating “cookie” as “bolacha recheada” (“sandwich cookie”)^(12)^ – and difficulties with items that lack an approximate translation in the target language with the same meaning intended by the original author^(20)^.
The discussion on translations, particularly the synthesis of translations involving the study authors, points out the fact that few analyzed articles reported the original scale authors’ participation in translation synthesis and joint analysis with the translators. On the other hand, they emphasized the importance of training and/or years of experience in translation or work on the topic at hand^(24-26)^.
The translators in this study had an average of over 5 years of experience in translation. Following the steps described by Beaton et al.^(9)^, one of the translators responsible for the first stage was familiar with the technical concepts of the instrument, demonstrating expertise in the field. The results of the translation and back-translation stages were as expected, yielding a translation that reflected the language and its semantic, syntactic, and grammatical aspects. Lastly, it is understood that translation and back-translation alone do not provide sufficient evidence of validity. In other words, although the final translation model resulted in a translated and back-translated scale suitable for clinical application, much further evidence is necessary to ensure the instrument’s validity and reliability for its intended purpose^(15)^.
Furthermore, the original version of the scale did not include representative images to facilitate training for the professionals administering it. Hence, it was necessary to verify content validity evidence for the selection and inclusion of images and thus proceed with the investigation of validity evidence for this scale. This step was crucial to enable its reliable future use by both researchers and clinicians.
The discrepancies cited in the results highlighted various factors that complicated the selection of images for the translated instrument. There was greater difficulty in regions encompassing more than one location, such as “Lateral and posterior pharyngeal wall” and “Valleculae and tip of epiglottis,” as many of the analyzed exams did not show both structures with residue. The judges also cited the evaluation of static images, such as that of the “Postcricoid region.” According to one of the judges, the image would be challenging to classify due to potential interference from the posterior pharyngeal wall, leading to uncertainty when distinguishing between the “moderate” and “severe” grades.
The BRACS assesses PR in different regions of the pharynx, including the efficiency of the clearance mechanism (i.e., residue removal), which sets it apart from other scales^(6,8)^. Moreover, it offers clear PR level markers, making it a strong instrument to support clinical decision-making in oropharyngeal dysphagia, alongside other clinical and instrumental findings.
On the other hand, the absence of images in the original BRACS hinders the precise understanding of the original authors' expectations regarding the visual elements necessary for training and applying the scale. This allowed us to advance and propose images that could facilitate this process.
Other PR scales^(6,8)^ have often used visual representation with selected static images to depict swallowing findings and classify impairment levels. Although the images are static, PR regards the volume and anatomical markers of the regions involved, indicating differences between levels. However, it is important to emphasize that every qualitative and quantitative swallowing analysis method always requires training for the evaluator to minimize analysis subjectivity and ensure instrument reliability.
Hence, this stage of the process has been completed, and it is necessary to proceed to confirm the instrument’s advantages and disadvantages in measuring PR in FEES. Therefore, new steps will be taken towards future contributions to this diagnostic method for classifying PR in oropharyngeal dysphagia.
CONCLUSION
The process of translating and cross-culturally adapting the scale has been completed, and the selection of images for the visual-perceptual evaluation of PR in the BR-BRACS has been concluded with evidence of content validity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Langmore SE History of fiberoptic endoscopic evaluation of swallowing for evaluation and management of pharyngeal dysphagia: changes over the years Dysphagia 2017321273810.1007/s 00455-016-9775-x 28101663 · doi ↗ · pubmed ↗
- 2Ansari NN Tarameshlu M Ghelichi L Dysphagia in multiple sclerosis patients: diagnostic and evaluation strategies Degener Neurol Neuromuscul Dis 202010152810.2147/DNND.S 19865932273788 PMC 7114936 · doi ↗ · pubmed ↗
- 3Dyer JC Leslie P Drinnan MJ Objective computer-based assessment of valleculae residue: is it useful?Dysphagia 200823171510.1007/s 00455-007-9088-117593433 · doi ↗ · pubmed ↗
- 4Pearson WG Jr Molfenter SM Smith ZM Steele CM Medição baseada em imagem de resíduos pós-deglutição: escala de razão de resíduos normalizada Disfagia 20132816717710.1007/s 00455-012-9426-923089830 PMC 3584199 · doi ↗ · pubmed ↗
- 5Rommel N Hamdy S Oropharyngeal dysphagia: manifestations and diagnosis Nat Rev Gastroenterol Hepatol 2016131495910.1038/nrgastro.2015.19926627547 · doi ↗ · pubmed ↗
- 6Murray J Langmore SE Ginsberg S Dostie A The significance of accumulated oropharyngeal secretions and swallowing frequency in predicting aspiration Dysphagia 19961129910310.1007/BF 004178988721067 · doi ↗ · pubmed ↗
- 7Kaneoka AS Langmore SE Krisciunas GP Field K Scheel R Mc Nally E et al The Boston Residue and Clearance Scale: preliminary reliability and validity testing Folia Phoniatr Logop 201465631231710.1159/00036500625033761 · doi ↗ · pubmed ↗
- 8Neubauer PD Rademaker AW Leder SB The Yale pharyngeal residue severity rating scale: an anatomically defined and image-based tool Dysphagia 201530552152810.1007/s 00455-015-9631-426050238 · doi ↗ · pubmed ↗