Prolonged and Recurrent De Quervain’s Thyroiditis After Thyroid Fine Needle Aspiration
Kyrstin Lane, Brendan Pelikh, Jianyu Rao, Dianne S Cheung

TL;DR
A 75-year-old man experienced prolonged thyroid inflammation after a thyroid fine needle aspiration, suggesting the procedure may worsen De Quervain’s thyroiditis.
Contribution
This case report highlights a rare complication of thyroid FNA in patients with De Quervain’s thyroiditis.
Findings
Thyroid FNA may contribute to prolonged inflammation in patients with De Quervain’s thyroiditis.
Serial thyroid ultrasounds may help avoid unnecessary FNA in such cases.
Clinical distinction between De Quervain’s thyroiditis and other thyroid conditions is crucial.
Abstract
De Quervain’s thyroiditis (subacute thyroiditis) is a self-limited inflammation of the thyroid gland. It is diagnosed based on clinical history, physical examination, labs, and thyroid imaging. Thyroid fine needle aspiration (FNA) is typically not recommended unless the diagnosis is unclear or there are clinical signs concerning for malignancy. We present the case of a 75-year-old male who presented with symptoms of De Quervain’s thyroiditis and an inflammatory thyroid nodule. He had a thyroid FNA for further evaluation of the thyroid nodule. Ultimately, his clinical course was prolonged after he had a thyroid FNA, which was presumed to have contributed to further thyroid inflammation. This case highlights the importance of distinguishing De Quervain’s thyroiditis from other causes of thyroid pain, as well as the use of serial thyroid ultrasounds, as it may help avoid unnecessary FNA.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
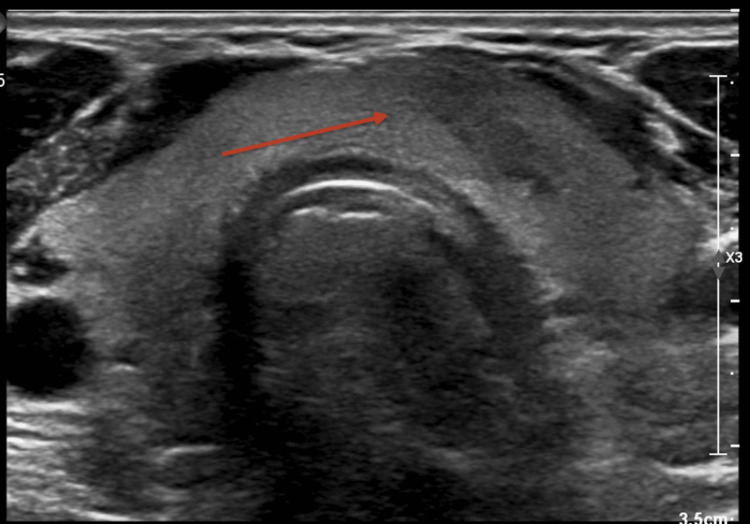 Figure 1
Figure 1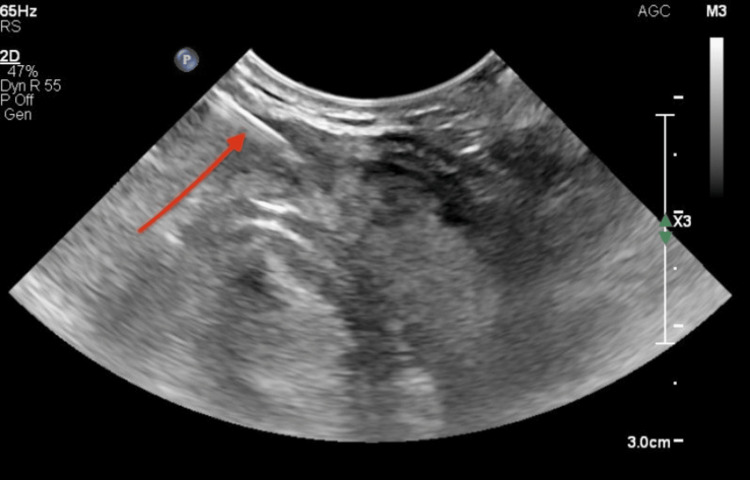 Figure 2
Figure 2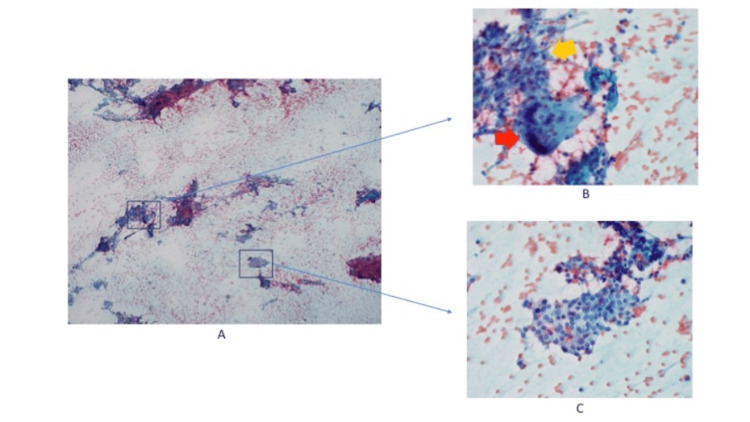 Figure 3
Figure 3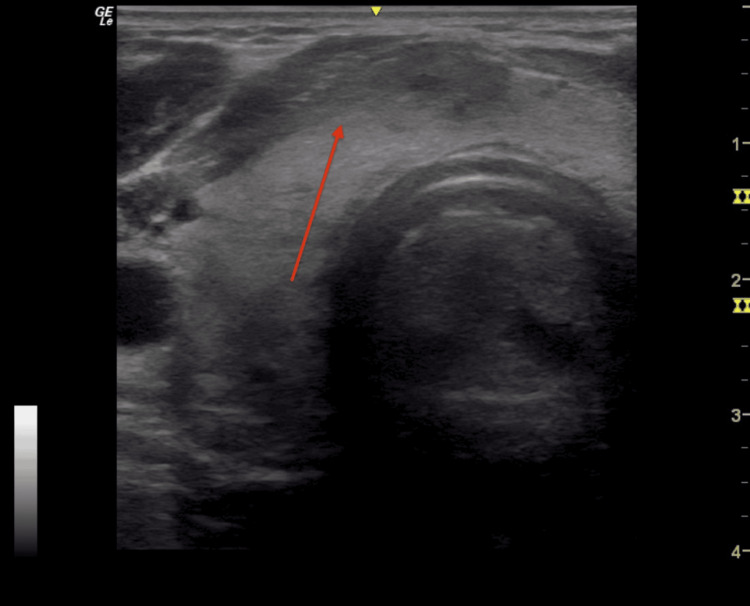 Figure 4
Figure 4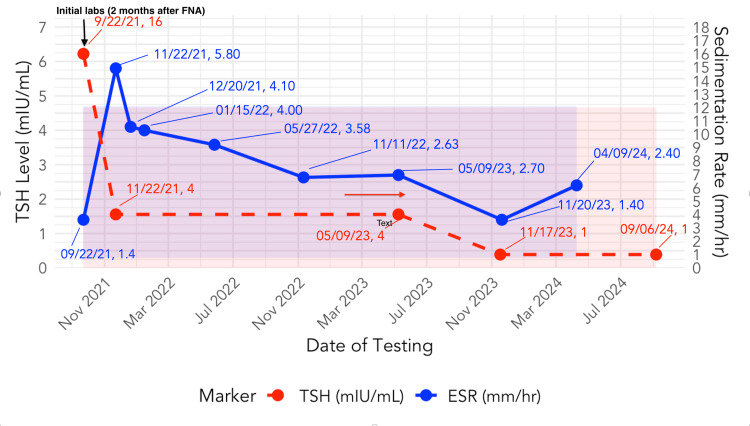 Figure 5
Figure 5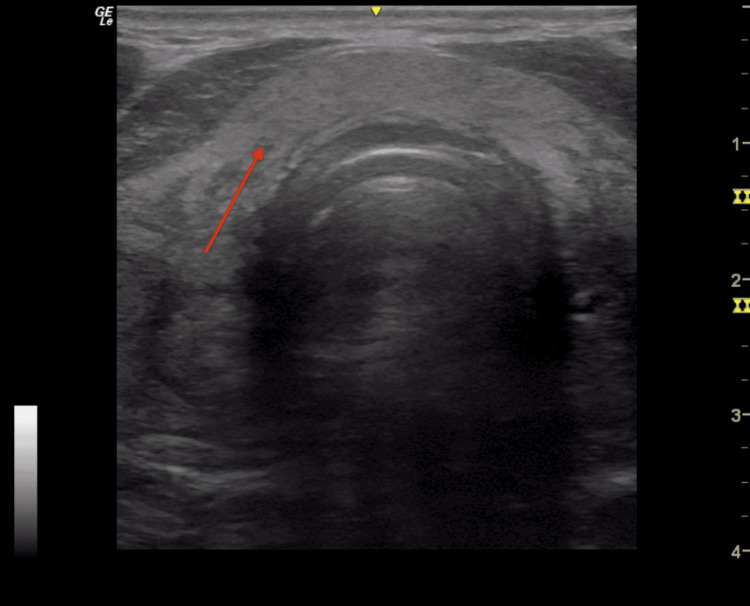 Figure 6
Figure 6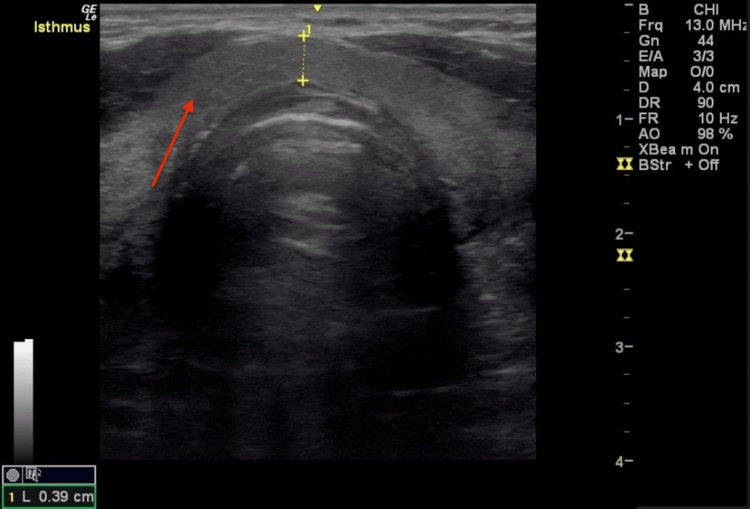 Figure 7
Figure 7| Laboratory Study | Initial presentation | One month post-FNA | Two months post-FNA | Four months post-FNA | Five months post-FNA | 11 months post-FNA | Reference range |
| TSH | 1.4 mcIU/mL | 5.8 mcIU/mL | 4.1 mcIU/mL | 0.3-4.7 | |||
| FT4 | - | 1.00 ng/dL | 1.00 ng/dL | 0.8-1.7 | |||
| FT4 index | 6.7 | - | - | 4.5-10.5 | |||
| FT3 | - | 282 pg/dL | 318 pg/dL | 222-383 | |||
| FT3 index | 91.8 | - | - | 78.0-162.0 | |||
| ESR | 16 mm/hr | 4 mm/hr | 2 mm/hr* | ≤ 12 mm/hr | |||
| (*≤ 20 mm/h on Westergren assay) | |||||||
| Thyroid ultrasound | 16 mm solid hypoechoic nodule versus heterogeneity in the isthmus | Hypoechoic region in the right lower isthmus consistent with needle trauma; no thyroid nodule | No thyroid nodule; post-biopsy inflammation is resolving | No thyroid nodule; post-biopsy inflammation has resolved |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Anomalies · Thyroid Cancer Diagnosis and Treatment · Clinical Reasoning and Diagnostic Skills
Introduction
De Quervain’s thyroiditis (DQT), also known as subacute thyroiditis (SAT), is an inflammatory disorder of the thyroid gland that is self-limited and thought to be triggered by viral upper respiratory tract infections (URIs) [1]. The reported incidence is 12.1 cases per 100,000/year [2]. It typically presents with acute, unilateral thyroid pain that may radiate to the ears as well as the jaw. Systemic symptoms such as fatigue, fever, and pharyngitis are frequently reported in the prodromal phase. Hyperthyroidism symptoms may be present, and there is low radioactive iodine uptake while hyperthyroidism is present. Physical examination is typically notable for a firm, tender, and mildly to moderately enlarged thyroid [1].
De Quervain’s thyroiditis can present diagnostic challenges due to its overlap with other thyroid pathologies, including potentially life-threatening conditions such as suppurative thyroiditis or thyroid malignancies. These may share similar clinical features, including visible thyroid enlargement and localized pain. While thyroid fine needle aspiration (FNA) is generally not indicated for DQT, it is sometimes performed if the diagnosis is unclear [1].
Cytological findings in DQT typically reveal multinucleated giant cells, epithelioid histiocytes, inflammatory infiltrates, and disrupted follicular cells within a granulomatous background [3]. Although FNA can aid in differentiating DQT from other thyroid conditions, such as malignancies, it carries the risk of exacerbating the inflammatory process. Some complications of thyroid FNA that have been reported include local hematoma formation, pain, swelling, infection, recurrent laryngeal nerve or tracheal injury, and thyrotoxicosis [4].
This case study examines a 75-year-old male patient with DQT in whom FNA was performed due to concerns for malignancy. The biopsy was thought to have resulted in a marked exacerbation of his thyroid pain and swelling as well as prolonging his recovery. This case illustrates an important complication of thyroid FNA, which, to our knowledge, has not been previously reported in the literature.
This case was presented as a poster in May 2025 by author Brendan Pelikh for the University of California, Los Angeles (UCLA) Undergraduate Research Week.
Case presentation
A 75-year-old male with no history of thyroid dysfunction presented to the ear, nose, and throat (ENT) specialist with a three-week history of anterior neck pain localized to the thyroid region. He reported initially experiencing a URI approximately two weeks before the onset of anterior neck pain, palpitations, and fatigue. He had no difficulty breathing, hoarseness, fever, night sweats, or weight loss. On examination, the ENT specialist noted thyroid gland enlargement. There were no labs collected, and no radioactive iodine uptake scan was completed at this time. Thyroid ultrasound (Figure 1) demonstrated a 16 mm solid isthmus hypoechoic lesion, which the radiologist interpreted to be a nodule versus focal heterogeneity. The ENT ordered a thyroid FNA to rule out malignancy. The radiologist completed thyroid FNA via a parallel (longitudinal) approach (Figure 2). Cytology (Figure 3) demonstrated a moderately cellular specimen with several sheets of benign reactive follicular cells, histiocytes, and mixed inflammatory cells, as well as some multinucleated giant cells, consistent with DQT.
Initial thyroid ultrasoundDemonstrates a 16 mm solid isthmus hypoechoic lesion (red arrow) thought to be a nodule versus focal heterogeneity.
Thyroid ultrasound performed during FNAThe needle used for the FNA appears as the white line (identified by the red arrow) entering the right of the thyroid nodule, which is located in the isthmus. FNA: Fine needle aspiration
Cytology from the thyroid FNAA: A low-power view shows a moderately cellular specimen with several sheets of benign reactive follicular cells, histiocytes, mixed inflammatory cells, as well as some multinucleated giant cells (4x). B: Histiocytes, mixed inflammatory cells, and multinucleated giant cells (40x) (red arrow: multinucleated giant cells, yellow arrow: histiocytes); C: Reactive follicular cells (40x)FNA: Fine needle aspiration
Initial treatment by the ENT specialist included a prednisone taper (initial dose of 60 mg daily was tapered over 16 days) and a course of azithromycin for a presumed acute bacterial URI. The pain initially subsided. The patient subsequently had a thyroid FNA. Following the thyroid FNA, the patient experienced a flare in symptoms, with increased neck pain and swelling. He was referred to endocrinology for further management.
At the initial endocrinology appointment, one month post-FNA, a thyroid ultrasound demonstrated a 16 mm hypoechoic region in the right lower isthmus, without calcifications, vascularity, or capsular invasion, which was consistent with trauma from the needle (Figure 4). There was no nodule at that time. The hypoechoic region noted on the initial ultrasound had resolved. The patient reported persistent pain described as coming in waves and tenderness to palpation over the thyroid. A second prednisone taper (initial dose of 40 mg daily) was prescribed, but his pain was only partially resolved after the two-week taper. Labs were ordered at that time and ultimately completed two months after the FNA, showing an elevated erythrocyte sedimentation rate (ESR) at 16 mm/hr (reference range is ≤12 mm/hr) but normal thyroid stimulating hormone (TSH), free thyroxine index (FT4 index), and free triiodothyronine index (FT3 index) (Figure 5).
Thyroid ultrasound at first endocrinology appointment (one month after the FNA)Demonstrated a 16 mm hypoechoic region (red arrow) in the right lower isthmus, without calcifications, vascularity, or capsular invasion, which was consistent with trauma from the needle. There was no nodule at that time. The hypoechoic region noted on the initial ultrasound had resolved.
The trend of TSH and ESR levels over timeThe reference range for TSH is 0.3-4.7 mcIU/mL, and for ESR is ≤ 12 mm/hr (≤ 20 mm/h on Westergren assay). No labs are available from the initial presentation to the ENT specialist. However, there is an elevation of the TSH four months after the FNA with subsequent normalization of the TSH. There is an elevated ESR two months after the FNA, with subsequent normalization of the ESR.FNA: Fine needle aspiration, TSH: Thyroid-stimulating hormone, ESR: Erythrocyte sedimentation rate
Three ultrasounds were performed over the next 12 months, which showed a gradual reduction and eventual resolution of the thyroid inflammation from the biopsy needle, as well as no signs of a thyroid nodule (Figures 6-7). Ongoing lab monitoring revealed a transient hypothyroid phase four months post-FNA with TSH 5.8 mIU/L (reference range 0.3-4.7), normal FT4, normal FT3, and normal ESR (Figure 5), and the patient was asymptomatic at the time. This was followed by normalization of thyroid function testing (Figure 5). Table 1 summarizes the thyroid function test results and ultrasounds over time. Over the subsequent three years, the patient experienced intermittent neck discomfort and tenderness in the thyroid region that would spontaneously resolve within days or weeks. The patient continues to be regularly monitored.
Thyroid ultrasound four months after the FNA No thyroid nodule present; the region of thyroid inflammation from the thyroid biopsy needle is resolving (arrow). The hypoechoic region noted on the initial ultrasound is not present. FNA: Fine needle aspiration
Thyroid ultrasound 11 months after the FNA The area of prior thyroid inflammation from the thyroid biopsy needle has resolved (arrow) and there are no thyroid nodules.FNA: Fine needle aspiration
Discussion
We present a unique case of prolonged and recurrent DQT presumed to be from thyroid FNA, a finding that has not previously been reported in the literature. Our case demonstrates the importance of correctly identifying the diagnosis of DQT based on its clinical presentation so that it can be appropriately managed. Patients with DQT often initially present with URI symptoms, followed by anterior neck pain, thyroid enlargement, and tenderness [1,2]. Labs initially demonstrate hyperthyroidism (typically with a ratio of T3 to T4 that is less than 20) lasting up to six weeks, followed by transient hypothyroidism seen in about 30% of individuals, and then most individuals ultimately become euthyroid [1,5]. Additional lab findings include elevated inflammatory markers (ESR, C-reactive protein), mild anemia, leukocytosis, and potentially low titers of thyroid autoantibodies [1]. In our patient, we presume the labs would have shown hyperthyroidism initially, but unfortunately labs were not drawn at the initial ENT appointment. Labs collected at two months post-FNA demonstrated an elevated ESR, and subclinical hypothyroidism was present at four months post-FNA, which ultimately resolved. Radioactive iodine uptake and scans typically demonstrate low uptake during the hyperthyroid phase. On ultrasound, the thyroid appears heterogenous with hypoechoic areas, and Doppler demonstrates reduced flow while in the hyperthyroid state, as seen in our patient. De Quervain’s thyroiditis should be distinguished from acute infectious (suppurative) thyroiditis, which presents as more severe neck pain (which can be localized) with fever and leukocytosis [2]. A minority of patients have hyperthyroidism or hypothyroidism [2]. Thyroid imaging (ultrasound or CT) is typically diagnostic, demonstrating hypoechoic regions, effacement of the border between the thyroid and surrounding tissue, as well as abscess formation [1,2]. These findings were not present in our patient.
Uncommonly, Graves' disease can present with thyroid pain due to capsule stretch, but typically has detectable thyroid autoantibodies, increased uptake on radioactive iodine uptake and scan, and thyroid ultrasound demonstrates hypervascularity [6]. Thyroid lymphoma or other malignancy is also a consideration, as it can present with neck pain and an elevated ESR [7]. Thyroid lymphoma has characteristic findings, including a quickly enlarging thyroid, obstructive symptoms (from compression of the trachea, esophagus, neck veins, and recurrent laryngeal nerve), systemic symptoms (fever, night sweats, and weight loss), signs of thyroid dysfunction, and a firm, immobile thyroid goiter with lymphadenopathy [8]. Thyroid ultrasound demonstrates multiple hypoechoic lesions, hypervascularity, and posterior echoes. If ultrasound findings are inconclusive or suggestive of lymphoma, then biopsy may be indicated [7,8]. Our patient did not have features suggestive of malignancy.
Our case highlights the role of serial thyroid ultrasound in cases of DQT, as this may help avoid unnecessary thyroid FNA. First, it is important to note that the American Thyroid Association (ATA) guidelines generally do not recommend FNA for evaluation of subacute thyroiditis, unless the diagnosis is unclear [1]. In our case, thyroid ultrasound also demonstrated a thyroid nodule described by radiology as thyroid imaging reporting and data system (TIRADS 4) because it was solid, hypoechoic, and had irregular margins but had no vascularity or calcifications. This would have been considered a high suspicion pattern based on the ATA criteria [9]. The initial thyroid ultrasound findings led to FNA, and serial ultrasounds showed resolution of the nodule. As the radiologist’s impression of the nodule is solely based upon the available images, it is important for clinicians to consider the clinical context when determining the necessity of FNA. Rather than immediately performing a thyroid FNA, the next step in this case should have been to obtain a TSH level [1,9]. It is also important for clinicians to understand the clinical course of thyroid nodules in patients with DQT. Observational studies have demonstrated various outcomes of thyroid nodules in individuals with DQT, ranging from some nodules resolving to instances of thyroid cancer being discovered [10,11]. Clinicians should consider waiting until the thyroiditis has improved to determine if ultrasound findings warrant doing a thyroid FNA.
Our case also demonstrates that while FNA is generally safe, there are potential risks. Thyroid FNA is generally considered a reliable, accessible, and low-cost diagnostic tool [4]. While complications following FNA are infrequently reported and are rarely associated with significant morbidity, it is important to be aware of the known complications, including procedural discomfort, hemorrhage/hematomas, thyroid swelling, thyroid infection, recurrent laryngeal nerve palsy, and vasovagal reactions [4]. Observational studies evaluating pain persisting following the procedure report persistent symptoms in less than 1% of patients [4]. However, the true incidence of more serious complications may be underrepresented in the literature due to potential reporting bias or concern over medico-legal complications [4].
Our case is unique in that the patient’s FNA was thought to have contributed to a complication of prolonged thyroid inflammation. To our knowledge, this has not been previously reported in the literature. De Quervain’s thyroiditis is a self-limited condition in which the inflammatory thyrotoxic phase typically resolves by six weeks. Our patient continued to demonstrate signs of thyroid inflammation months after the onset of symptoms. While the recurrence rate of subacute thyroiditis is generally estimated to be low in the literature (1% to 4%), our patient has also continued to experience flares over the subsequent three years [1]. This patient’s prolonged inflammation and recurrences were presumed to be due to irritation and inflammation caused by the FNA. It is therefore important to weigh the risks and benefits of FNA and individualize the decision for FNA on a case-by-case basis in nodules that meet FNA criteria.
Conclusions
This case highlights an uncommon prolonged course of DQT, with inflammation likely exacerbated by thyroid FNA. Important clinical features to consider when diagnosing DQT include the patient's symptoms, physical examination, serial ultrasound imaging, and thyroid function tests. Before performing an invasive procedure that could exacerbate DQT, clinicians must complete a thorough clinical assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis Thyroid Ross DS Burch HB Cooper DS 134314212620162752106710.1089/thy.2016.0229 · doi ↗ · pubmed ↗
- 2Acute and Subacute, and Riedel’s Thyroiditis Endotext (Internet). MD Text.com, Inc Majety P Hennessey JV Feingold KR South Dartmouth Endotext 2022 https://www.ncbi.nlm.nih.gov/books/NBK 285553/
- 3Subacute granulomatous (De Quervain's) thyroiditis: fine-needle aspiration cytology and ultrasonographic characteristics of 21 cases Cytojournal VuralÇ Paksoy N Gök ND Yazal K 91220152608583310.4103/1742-6413.157479 PMC 4453108 · doi ↗ · pubmed ↗
- 4Clinical complications following thyroid fine-needle biopsy: a systematic review Clin Endocrinol (Oxf) Polyzos SA Anastasilakis AD 1571657120091917071710.1111/j.1365-2265.2009.03522.x · doi ↗ · pubmed ↗
- 5De Quervain Thyroiditis Tabassom A Chippa V Edens MA Treasure Island Stat Pearls 2025 https://www.ncbi.nlm.nih.gov/books/NBK 526066/30252322 · pubmed ↗
- 6Subacute Thyroiditis Hennessey JV South Dartmouth Endotext 2000 https://pubmed.ncbi.nlm.nih.gov/25905310/
- 7New aspects in the pathogenesis and management of subacute thyroiditis Rev Endocr Metab Disord Stasiak M Lewiński A 102710392220213395040410.1007/s 11154-021-09648-y PMC 8096888 · doi ↗ · pubmed ↗
- 8Thyroid Lymphoma Kesireddy M Lasrado S Treasure Island Stat Pearls 2024 https://www.ncbi.nlm.nih.gov/books/NBK 544282/31335002 · pubmed ↗