Harmonization trial on ESR1 testing strategies in ER+/HER2- breast cancer patients: an Italian experience
Francesco Pepe, Gianluca Russo, Konstantinos Venetis, Claudia Scimone, Lucia Palumbo, Mariantonia Nacchio, Domenica di Giovanni, Claudia Sarracino, Ilaria Tomaiuolo, Elisabetta Zulato, Matteo Fassan, Daniela Righi, Giuseppe Perrone, Dario de Biase, Gabriele Casati, Fabio Pagni

TL;DR
This study evaluates testing methods for ESR1 mutations in breast cancer patients to improve detection consistency across labs in Italy.
Contribution
The study harmonizes ESR1 mutation detection strategies using reference samples and compares NGS and dPCR performance.
Findings
ESR1 p.D538G mutation was detected in 90% of samples A and B, and 80% of sample C.
NGS and dPCR showed similar performance in detecting low-frequency ESR1 mutations.
Harmonized ring trials can standardize procedures for better clinical stratification.
Abstract
To date, ESR1 activating mutations acts as key player to clinically stratify estrogen receptor (ER)+/HER2-advanced breast cancer (BC) patients eligible to novel new generation oral Selective Estrogen Receptor Degraders (SERD) relapsing after first line aromatase inhibitors. Liquid biopsy represents the most useful biological source to detect ESR1 activating mutations in clinical setting, but the lack of standardized pre-analytical and analytical procedures drastically impacts on detection rate of ESR1 mutations in diagnostic specimens. Here, we sought to harmonize technical procedures comparing technical performance of diagnostically available testing strategies on a series of three reference specimens (sample A, B, C) harboring ESR1 p.D538G mutation at different mutant allele fraction (MAF) (5.0 %, 1.0 %, 0.5 %) shared with n = 10 Italian referral institutions. A total of 10 μl of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
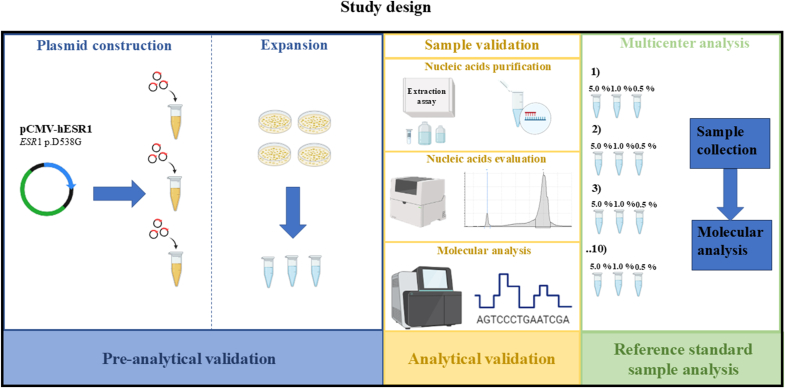 Figure 1
Figure 1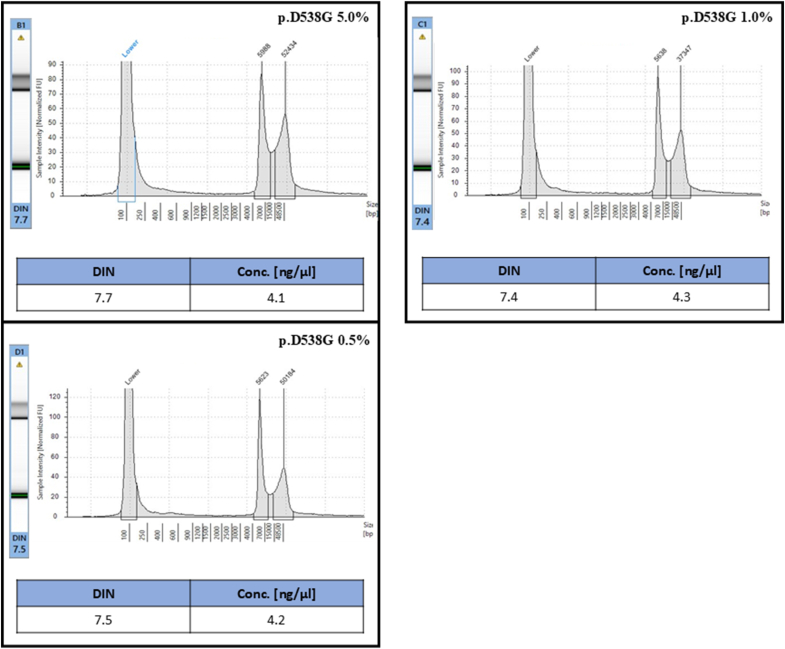 Figure 2
Figure 2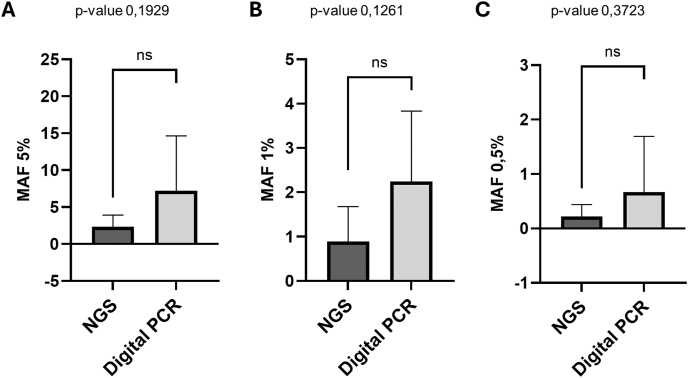 Figure 3
Figure 3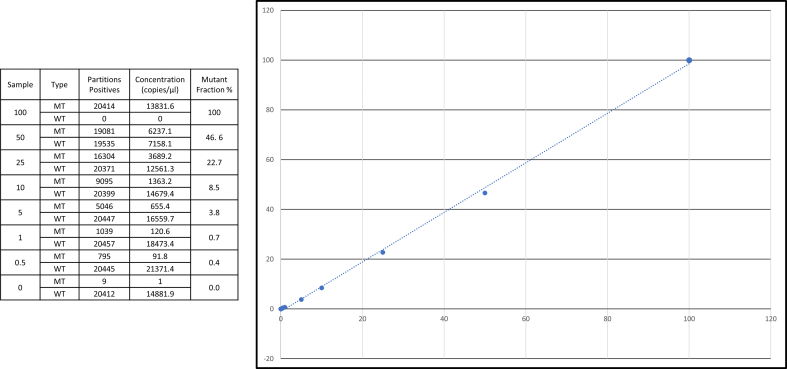 Figure 4
Figure 4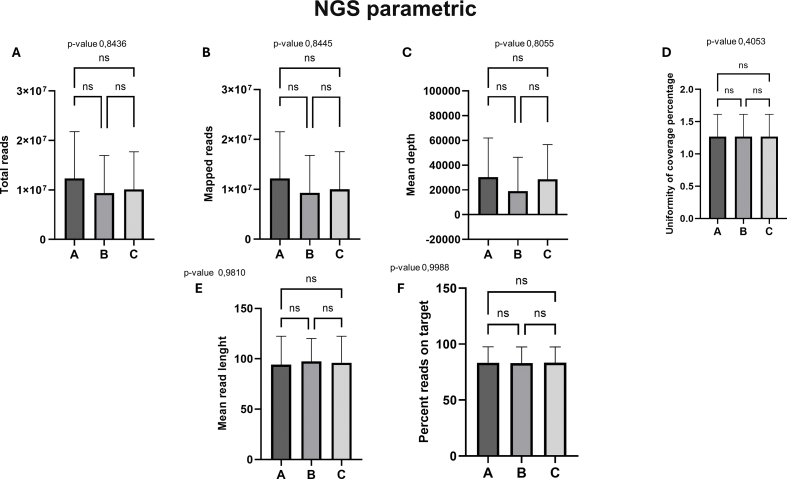 Figure 5
Figure 5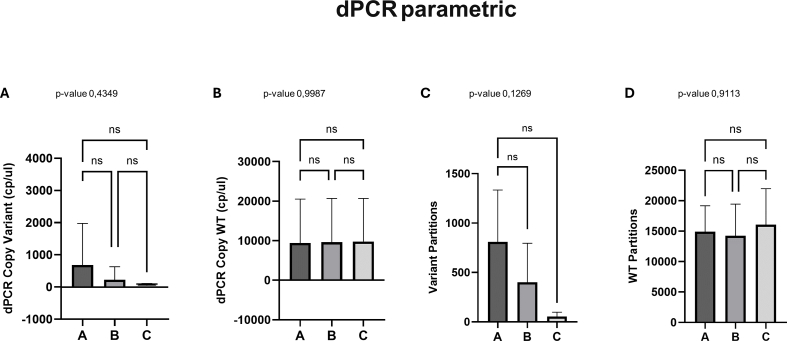 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · Advanced biosensing and bioanalysis techniques · Gene expression and cancer classification
Introduction
1
Nowadays, tailored options have shifted the clinical paradigm for breast cancer patients (BC). Firstly, Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha (PIK3CA) was approved by international societies for the clinical stratification of BC patients expressing specific receptor profile [hormone receptor (HR)+/HER2-] [1,2]. Recently, it has been established that estrogen receptor (ER) alpha (ESR1) activating mutations play a pivotal role in driving tumor progression in (HR)+/HER2- BC patients after first line of endocrine therapy (ET) [3,4]. Of note, ESR1 dependent resistant mechanisms occur in 40.0 % of metastatic (HR)+/HER2- BC patients relapsing from aromatase inhibitor (AI) plus endocrine regimen [5]. In this scenario, liquid biopsy emerged as the most promising biological source for recovering nucleic acids to test ESR1 in the diagnostic routine practice of HR+/HER2- BC patients. The clinical rationale derives from the clinical benefit guided by ESR1 mutations in (HR)+/HER2- BC patients treated with selective ER degraders (SERDs) and ER modulators (SERMs) compared with standard of care endocrine monotherapy [6,7]. Blood based ESR1 (bESR1) activating alterations were investigated in clinical trials where bESR1 mutant BC patients were elected to ER inhibitors after molecular profiling of liquid biopsy samples [8,9]. Phase III EMERALD trial (NCT03778931) demonstrated improving rate of progression-free survival (PFS), in randomized ER+/HER2–advanced BC patients harboring ESR1 activating mutations under elacestrant (oral SERD) in comparison with standard of care (SOC) [2,10]. In addition, the phase III PADA-1 trial (NCT03079011) prospectively investigated the clinical relevance of switching therapy in bESR1mut BC patients after first-line AI randomizing patients to fulvestrant or maintaining the same therapeutical scheme in accordance with bESR1 molecular assessment [11]. Phase 3trial SERENA-6 (NCT04964934) confirmed clinical efficacy of switching from AI to novel generation oral SERD (Camizestrant) detecting ESR1 mutations in liquid biopsy samples before clinical progression from standard of care [12]. Remarkably, distinct technological approaches were adopted in the aforementioned trials: the former was built on a comprehensive next generation sequencing (NGS) assay (Guardant360® CDx, GuardantHealth, CA, USA) able to simultaneously detect clinically informative molecular alterations across 55 cancer related genes from liquid biopsy specimens, including ESR1 activating mutations (310–547 codons); the latter on customized digital droplet PCR (ddPCR) assays to analyze four hotspot mutations covering 90.0 % of most frequent ESR1 actionable alterations [2,11]. Preclinical studies identified more than n = 60 hotspot molecular alterations in ligand-binding domain (LBD) impacting on the constitutive activation of signaling pathway. Given the heterogeneous distribution of ESR1 activating mutations and the impressive number of predictive biomarkers approved in clinical practice NGS platforms are recommended but a not negligible percentage of institutions addicted to molecular tests routinely adopt single-plex platforms [8,13,14].
Not surprisingly, each testing strategy harbors distinct technical parameters in terms of accuracy rate, reference range and turn-around time (TAT) impacting on standardization of analytical procedures [15,16]. On this basis, the lack of standardized processes could decrease the number of patients eligible for target therapy. To fill this gap, harmonized handling protocols increasing the detection rate of ESR1 hotspot mutations in BC patients are required. Hence, we designed a multicenter trial involving n = 10 highly experienced Italian Institutions in molecular testing to analyze a ESR1 activating mutation on a customized reference sample at different variant allele fraction (VAF). Then, concordance rates were evaluated by comparing the molecular results shared by each participating institution.
Methods
2
Study design
2.1
A series of three standard reference samples (sample A, B, C) harboring ESR1 p.D538G (NM_001291230.2) activating mutation at scalable VAF (5.0 %, 1.0 %, 0.5 %) were shared by the coordinator center with nationwide institutions involved in molecular tests. This series was able to cover mostly recurrent VAF levels in real-life molecular diagnosis of ESR1 positive ER+/HER2 BC patients [17]. Artificial control was built engineering pRP-CMV-hESR-WT plasmid with p.D538G ESR1 mutation. Before shipping standard reference samples to participating institutions, coordinator institution (University of Naples Federico II) internally validated sample set adopting both NGS platform and dPCR assay, in accordance with clinical trials of elacestrant [10]. Briefly, fragmentation rate of nucleic acids from pRP-CMV-hESR engineered samples was also evaluated by microfluidic platform validating quality/quantity of gDNA before molecular analysis on the most recommended platforms by international societies [18] After internal validation, a sample set grouping three ESR1 p.D538G engineering samples (5.0 %; 1.0 %; 0.5 % VAF) was sent to all participating institutions (n = 10). Each institution analyzed standard reference samples following its own routinely implemented diagnostic workflow. Finally, technical and molecular records on ESR1 molecular analysis were annotated in dedicated form and sent to the coordinator institution (Fig. 1). Biological material was managed under the authorization of Department of Public Health at the University of Naples Federico II, Naples.Fig. 1. Schematic representation of study design. Briefly, after internal validation of standard reference sample at University of Naples Federico II, a set of standard reference samples built to mimic ESR1 5.0 %, 1.0 % and 0.5 % p.D538G mutations were shared with n = 10 referral institutions after internal validation. Here, own diagnostic workflow (from Nucleic Acid extraction to molecular data interpretation) was approached. Data were shared with coordinator center. Abbreviations: CMV (cytomegalovirus promoter), ESR1 (Estrogen receptor-1).Fig. 1
Standard sample generation and validation
2.2
The plasmid vectors expressing the CDS contained in the hESR1 ORF [NM_001291230.2] under the control of the CMV promoter were custom-designed and generated at the VectorBuilder Inc. company (Chicago, IL, USA). The plasmid vectors used as positive controls express the CDS contained in the ORF NM_001291230.2 corresponding to hESR1-WT (pRP-CMV > hESR1-WT) and the corresponding CDS in which the GAC > GGC (pRP-CMV > hESR1-D538G). Each engineered sample was expanded following standardized procedures for bacterial clones [19]. Then, pRP-CMV > hESR1-D538G (100.0 % VAF) was mixed with wild type ESR1 samples (pRP-CMV-hESRWT) to arrange a longitudinal series of reference specimens covering seven experimental points ranging from 100.0 % to 0.5 % of VAF [10,11]. internally confirmed on a dPCR system (Supplementary Fig. 1).
Nucleic acids qualification
2.3
Focusing on three experimental points (pRP-CMV > hESR1-D538G 5.0.-0.5 % VAF), gDNA was evaluated on 4200 TapeStation system (Agilent Technologies, Santa Clara, California, USA), a fully automatized microfluidic platform, in terms of nucleic acids amount (ng/μl) and fragmentation index [2]. As regards, 1 μl of genomic DNA was manually combined with 10 μl of proprietary buffer and automatically loaded into a Genomic ScreenTape cartridge (Agilent Technologies, Santa Clara, California, USA). Then, nucleic acids were analyzed on 4200 TapeStation system (Agilent Technologies, Santa Clara, California, USA), in accordance with manufacturer protocol. Finally, DNA integrity number (DIN), scored between 0 (high-fragmented profile) and 10 (low-fragmented profile), was interpreted by using the TapeStation 4200 analysis software (Agilent Technologies, Santa Clara, California, USA).
Molecular analysis
2.4
QuantStudio Absolute Q Digital PCR System (Thermo Fisher Scientific, Waltham, Massachusetts, USA) was used in accordance with manufacturer instructions to test reference standard samples. Briefly, 1 μl of engineered gDNA was combined with Absolute Q™ DNA Digital PCR Master Mix 5X (Thermo Fisher Scientific, Waltham, Massachusetts, USA) and Custom SNP Genotyping product dPCR Assay (Thermo Fisher Scientifics, Waltham, Massachusetts, USA) covering n = 5 most common ESR1 activating mutations (exon 10 p.L536R, p.Y537C, p.Y537N, p.Y537S, p.D538G). Each well was complemented with QuantStudio™ Absolute Q™ Isolation Buffer (Thermo Fisher Scientifics, Waltham, Massachusetts, USA) supporting DNA fragments’ diffusion across wells on QuantStudio™ Absolute Q™ MAP16 Plate (Thermo Fisher Scientifics, Waltham, Massachusetts, USA). Thermal profile, partitioning procedure and signal detection were assessed on proprietary analysis software QuantStudio Absolute Q Digital PCR System Software (Thermo Fisher Scientifics, Waltham, Massachusetts, USA) maintaining standardized technical parameters. Positive signaling threshold was manually set at 5000 RFU for inspecting both mutant and wild-type signal. The total amount of copies/μl and matched MAF level were calculated by fractioning the number of positive partitions on the total valid partitions (based on Poisson distribution) in each well.
The fully integrated Genexus™ platform (Thermo Fisher Scientific, Waltham, Massachusetts, USA) was adopted on validation series of standard reference samples. As regards, libraries were generated adopting the Oncomine Precision Assay (OPA) panel, able to cover the most clinically informative molecular alterations across n = 50 reference genes (including ESR1 ligand binding domain), in accordance with the manufacturer’s instructions [5]. Each sample was manually diluted and immediately dispensed on a 96-well plate equipping technical platform. Sequencing was approached on GX5TM chip following manufacturer procedures. Briefly, data analysis was carried out by variant calling plug-in based on Oncomine Knowledgebase Reporter Software (Oncomine Reporter 5.0) integrated in Genexus software (v.1.0). In addition, BAM files were also visually inspected targeting ESR1 ligand binding domain (LBD) mutations on Golden Helix Genome Browser v.2.0.7 (Bozeman, MT, USA). Variants showing coverage ≥500X and mutated reads >10X were annotated.
Statistical analysis
2.5
Continuous data are presented as mean ± standard deviation. A statistical significance was set at a two-tailed p-value of 0.05. All statistical analyses, including Student’s t-test for comparisons between two groups and one-way or two-way ANOVA followed by Tukey’s post hoc test for multiple group comparisons, were conducted using Prism GraphPad software, version 10.0 for Windows (GraphPad Software, Boston, MA, USA; www.graphpad.com).
Results
3
Standard sample generation and validation
3.1
Overall, A, B, C samples highlighted 4.1 ng/μl, 4.3 ng/μl and 4.2 ng/μl, respectively. A DIN of 7.7, 7.4 and 7.5 were also inspected demonstrating high quality of DNA profile (Fig. 2). The sample series was successfully evaluated in duplicate adopting both NGS and dPCR systems (Supplementary Table 1). Particularly, NGS quality checks were satisfied for each engineered sample: a median number of 3168695.5, 1133152.0 and 1850359.0 total reads; mean read length of 106.0, 103.0 and 104.0; number of mapped reads of 3132220.0, 1112778.5 and 1823408.0, a percent reads on target of 72.2 %, 73.4 % and 75.0 %, a mean depth of 10292.0, 3612.5 and 6132.0 were inspected in samples A, B and C, respectively. Moreover, dPCR system reached a total of 9483.2, 69.8 and 20.9 copies/μl in sample A, B, and C, respectively, manually filtering threshold at 5000 RFU. Of note, NGS (median 4.4 %, 1.1 %, 0.3 %) and dPCR (4.8 %, 1.0 %, 0.6 %) confirmed VAF levels of ESR1 p.D538G activating mutation in reference standard sample set from two independent experimental set up (Table 1) (Supplementary Table 1)Fig. 2. Internal validation - nucleic acids quantifications and qualifications by using TapeStation4200 platform (Agilent, Santa Clara, CA, USA) on standard reference samples A, B, and C.Fig. 2. Table 1Molecular results from internal validation by coordinator institution on reference standard samples A-C adopting NGS and dPCR sysems (Thermofisher Scientifics).Table 1. TechnologyPlatformAssaySample A (5.0 %)Sample B (1.0 %)Sample C (0.5 %)NGSIonTorrent Genexus Integrated SequencerOncomine™ Precision Assay GX4.4 %0.8 %0.3 %4.4 %1.4 %0.3 %dPCRQuantStudio Absolute Q Digital PCRCustom Assay4.2 %1.0 %0.5 %5.3 %1.0 %0.6 %
Standard sample analysis
3.2
Overall, a sample set including aliquots (15 μl) from A-C engineered plasmids was successfully shared by coordinator institution with n = 10 participating laboratories. Technical data and molecular results were listed in a dedicated repository file and sent to coordinator institution within 60 working days. As suggested by experimental design, participating institutions adopted their own diagnostically available testing strategy to evaluate ESR1 activating mutations in standard reference samples. Particularly, 6 out of 10 (60.0 %) and 4 out of 10 (40.0 %) institutions adopted NGS and dPCR systems, respectively. Among NGS group, amplicon-based, and hybridization-based platforms were used in n = 3 (50.0 %) and n = 3 (50.0 %), respectively, to detect ESR1 p.DS538G hotspot mutation. Interestingly, a custom hybridization NGS assay was used in a single instance (ID#9). Given 4 out of 10 (40.0 %) institutions selected dPCR approach, a digital droplet PCR system (ddPCR) was used in 2 out of 4 (50.0 %) institutions, remaining cases (50.0 %) selected plate-based dPCR system for genotyping the ESR1 most common hotspot mutations (n = 5) (Table 2).Table 2. Technical approaches of each participating institutions evaluating p.D538G mutations in standard reference samples A-C.Table 2. CentreTechnologyPlatformAssay**#1ddPCRQX 200 BIO-RADddPCR Supermix for Probes#2NGSIonTorrent Genexus Integrated SequencerOncomine™ Precision Assay GX#3dPCRQuantStudio Absolute Q Digital PCRCustom Assay#4NGSIonTorrent Genexus Integrated SequencerOncomine™ Precision Assay GX#5NGSIllumina MiseqAmoy HRR NGS panel#6ddPCRQX 200 BIO-RADddPCR Supermix for Probes#7NGSIllumina MiseqAmoy HRR NGS panel#8NGSIonTorrent Genexus Integrated SequencerOncomine™ Precision Assay GX#9NGSIllumina MiseqCustom Assay#10**dPCRQuantStudio Absolute Q Digital PCRCustom Assay
Data analysis
3.3
Overall, standard reference samples were successfully analyzed in all instances (see Table 3a). Particularly, ESR1 p.D538G hotspot mutation was detected in 90.0 % of samples A, B whereas was identified in 8 out of 10 (80.0 %) sample C by participating institutions. Moreover, dPCR and NGS platforms detected p.D538G ESR1 mutation in 4 out of 4 (100 %) and 5 out of 6 (83.3 %); 4 out of 4 (100 %) and 5 out of 6 (83.3 %); and 4 out of 4(100 %) and 4 out of 6 (67.0 %) A, B, C samples, respectively. NGS-based testing strategies showed a median number of 10608723.7 total reads (ranging from 1845577.0 to 25284921.0), of 10497515.8 mapped reads (ranging from 1822160.0 to 24924523.0), a median read length of 95.9 (ranging from 44.0 to 110.0), a percentage reads on target of 83.2 % (ranging from 71.2 % to 99.6 %) an average mean depth of 26011.3 (ranging from 2916.0 to 81069.0). No significant variations in terms of NGS technical parameters were observed among longitudinal samples (p-value >0.05) (Supplementary Fig. 2). In addition, dPCR platforms identified a median of 683.9 cp/μl, (ranging from 0.2 to 2992.0), 228.7 cp/μl (ranging from 0.8 to 947.0) and 40. 3 cp/μl (ranging from 0.3 to 164.0) in A, B, and C samples (Table 3 A-B). Similarly, no statistically significant variations were identified comparing dPCR technical parameters across longitudinal samples (p-value >0.05) (Supplementary Fig. 3). Among institutions adopting NGS systems, amplicon and hybridization-based approaches demonstrated a comparable technical performance in detecting ESR1 p.D538G hotspot mutation in standard reference samples (3/3 amplicon-based and 2/3 hybridization-based strategies). Notably, a single participating institution (ID#5) failed to successfully detect p.D538G ESR1 alteration in shared samples. Under the supervision of coordinator institution, molecular analysis of standard reference samples was carried out. Particularly, institution ID#5 switching to orthogonal technology (dPCR), was able to successfully identify referenced mutations in engineered samples set (Table 4). Remarkably, the trained program achieved a detection rate of 100.0 % and 90.0 % for standard reference samples A-B and C (9 out of 10), respectively, involving all participating institutions. Finally, a median VAF level of 4.8 (ranging from 0.58 % to 20.0 %), 1.6 % (ranging from 0.3 % to 4.0 %) and 0.5 % (ranging from 0.1 % to 2.5 %) were identified. In addition, NGS and dPCR systems highlighted no significant variations in terms of VAF measurement across samples A-C: 2.3 % (ranging from 0.6 % to 4.5 %) and 7.2 % (from 1.6 to 20.0 %); 0.9 % (from 0.3 % to 2.2 %) and 2.2 % (from 0.8 % to 4.0 %); 0.3 % (from 0.1 to 0.5 %) and 0.7 % (from 0.1 to 0.2.5). (p-value >0.05) (Table 4)Table 3aTechnical parameters from NGS analysis performed by participant institutions on samples #A, #B, #C.Table 3aCentre ID/SampleTotal readsMapped readsMean depthUniformity of coverageMean read lenghtPercent reads on target**#2A2446707241053279211.4 %10275.1 %B1845577182216059451.4 %10374.0 %C2062012202911766891.4 %10374.7 %#4A2528492124924523810691.5 %10971.2 %B2070140020500036671021.5 %11071.4 %C2091121620700872676381.5 %11071.6 %#7A171382881707487668430.8 %4499.6 %B7343666730180729160.8 %5799.4 %C8334780829894033210.8 %4999.6 %#8A1279111212604425411441.4 %10772.3 %B129133291273454741811.4 %10872.1 %C1439459914227287477411.4 %10973.2 %#9A3981808394199014639NA10998.0 %B4106384406532015097NA10998.0 %C4875056482630517923NA10998.0 %Table 3bTechnical parameters from dPCR analysis performed by participant institutions on samples #A, #B, #C.Table 3bCentre ID/SampleCopy Variant (cp/ul)Copy WT (cp/ul)Variant PartitionsWT Partitions#1A51.03190.0668.014701.0B26.73000.0240.09866.0C6.54700.0104.018481.0#3A0.25.9NANAB0.848.8NANAC0.394.7NANA#5A2992.020091.0369.410740.0B947.020336.0110.012947.0C164.020074.018.79324.0#6A203.01015.0NANAB68.41753.8NANAC26.41056.0NANA#10A173.422839.01391.019269.0B100.722923.0851.019987.0C**4.122973.036.020418.0Table 4B. Molecular result of MAF measurement on standard reference samples engineered with p.D538G mutation and corrective procedures (∗) enabled successful detection of p.D538G mutations among institutions #3 and #5.Table 4. CentreSample A (5.0 %)Sample B (1.0 %)Sample C (0.5 %)#11.6 %0.9 %0.1 %#23.4 %2.2 %0.4 %#33.8 %1.6 %0.3 %#3∗NA0.7 %0.3 %#41.5 %0.3 %0.1 %#5FailedFailedFailed#5∗3.3 %0.8 %0.2 %#620.0 %3.9 %2.5 %#70.6 %0.6 %nd#81.7 %0.3 %0.1 %#94.5 %1.0 %0.5 %#107.2 %4.0 %0.2 %
Discussion
4
With the advent of the genomic era, the molecular landscape of advanced BC patients has been progressively improved revealing clinically significant predictive biomarkers able to shift the clinical paradigm for ER+/HER2- BC patients [20,21]. On this basis, challenging diagnostic specimens are controversial sources of nucleic acids to successfully perform genomic profile of clinically relevant predictive biomarkers due to scant diagnostic material [22,23]. Particularly, tissue biopsy may be affected by low quality nucleic acids depending on disharmonized preanalytical procedures [23]. Conversely, the low abundance of cfDNA in peripheral blood improves false negative rate in detecting druggable alterations in solid tumor patients [4], [24], [25]. On this basis, tissue and liquid biopsy samples became integrative tools in the clinical management of advanced BC patients identifying actionable alterations to guide therapeutic strategies [6], [26], [27]. Particularly, ESR1 activating mutations should be tested to elect (10.13039/501100014832HR)+/HER2- BC patients, relapsing after first line therapy with aromatase inhibitors, to novel oral SERD [12,28]. It has been ascertained that ESR1 actionable mutations are elicited as resistance mechanism of first line treatment supporting the central role of liquid biopsy to detect ESR1 hotspot mutations [29]. In this scenario, liquid biopsy emerged as a dynamic, less invasive and technically consistent biological source of nucleic acids investigating ESR1 mutations in first line resistant BC patients [30,31]. Behind the clinical implementation of liquid biopsy in clinical practice, several opening challenges drastically impact on ESR1 molecular analysis [30,32]. Firstly, the lack of harmonized preanalytical procedures (inadequate collection time, disharmonized cfDNA preservation and purification protocols) affects ESR1 detectability in diagnostic specimens. Secondly, analytical strategies are heterogeneous in terms of technical parameters (reference range, technical sensitivity) increasing inter variability among laboratories involved in ESR1 molecular testing [12,33,34]. Here, we sought to evaluate technical performance of diagnostic routine workflows in n = 10 Italian referral institutions for molecular testing sharing an ESR1 standard reference sample built to mimic VAF levels of real diagnostic samples. Being aligned with technical equipment of PADA-1 [11] and EMERALD [2] trials, both dPCR and NGS-based strategies were internally validated before the shipment of standard reference samples to participating institutions. Interestingly, dPCR systems require threshold set up because fluorescent signal also saturate empty wells in engineered samples. Conversely, NGS platforms were able to detect ESR1 p.D538G hotspot mutation with VAF <1.0 % optimizing the bioinformatic pipeline to detect low-frequency molecular alterations. On this basis, coordinator institutions visually inspect NGS data to properly identify VAF <1.0 % ESR1 alterations. These findings stress the need for harmonizing data interpretation procedures because molecular interpreting criteria, like the visual inspection of molecular records, could exclude ER+/HER2 BC patients from the best therapeutical strategy [33]. Additionally, molecular diagnosis of ESR1 <1.0 % from diagnostic samples require highly sensitive technical platforms (dPCRs and NGS) that allow to identify low abundant alterations electing ER+/HER2- BC patients for oral SERD [34,35]. Opening challenges in the handling procedures of ESR1 test on diagnostic routine samples significantly affect positivity rate suggesting that trained personnels act as key players to successfully administrate technical parts of molecular testing [3,6]. At the sight of this critical point, institution ID#2 inspected ESR1 p.D538G molecular alteration in standard reference samples set under the supervision of coordinator institution supporting entire handling and data interpretation phase. In the same scenario, ID#5 implemented an NGS based testing strategy to target referenced alterations in artificial samples failing to yield molecular results due to hard technical procedures. Here, an orthogonal technology (dPCR) was adopted after an in-site training properly identifying ESR1 p.D538G hotspot mutations in reference series. On this basis, diagnostic algorithm integrating orthogonal technologies should be implemented to adequately administrate diagnostic routine samples from BC patients ([7,8]). Sustaining this proof of concept, simultaneous analysis of standard reference samples was realized adopting a plate-based dPCR system and a BC tailored cfDNA based NGS panel in a single instance (ID#3). Interestingly, no statistically significant variations were identified comparing NGS and dPCR results on standard reference samples. (p-value >0.05) [36], [37], [38]. In addition, low technical intra-variability was observed in terms of technical parameters. In particular, VAF levels showed comparable results on sample A-C among participating institutions. (p-value >0.05) (Fig. 3). Our study shows some limitations, including the hard handling procedures to optimize technical analysis on engineered plasmid, the heterogeneous landscape of technical strategies to perform molecular tests across participating institutions and the lack of a more comprehensive standard reference series covering multiple ESR1 mutations >5.0 % [[39], [40], [41]]. Additionally, manual set up of dPCR threshold and visual inspection of NGS raw data may impact on VAF detectability across participating institutions; in particular below 1.0 % [41]. On this basis, harmonization ring trials investigating ESR1 testing procedures are insightful to check diagnostic workflow in diagnostic settings. Further investigations should be approached covering predictive biomarkers in ER+/HER2- BC patients also overviewing preanalytical handling procedures affecting molecular analysis of diagnostic samples.Fig. 3MAF levels comparison among participating institutions. Statistical analysis comparing VAF levels in standard reference samples (5.0 %, 1.0 %, 0.5 %) among the institutions (NGS or dPCR) was approached. Mean percentage ± SD of independent analysis (p-value >0.05) was calculated.Fig. 3
Patient consent for publication
Not applicable
Author contributions
Conceptualization, Francesco Pepe, Gianluca Russo, Giancarlo Troncone and Umberto Malapelle.; methodology, all the authors; software, Francesco Pepe, Gianluca Russo; validation, all the authors; formal analysis, all the authors; data curation, Francesco Pepe, Gianluca Russo and Umberto Malapelle.; writing—original draft preparation, Francesco Pepe, Gianluca Russo; writing—review and editing, Giancarlo Troncone and Umberto Malapelle.; visualization all the authors; supervision, Giancarlo Troncone, and Umberto Malapelle.; project administration, Giancarlo Troncone and Umberto Malapelle All authors have read and agreed to the published version of the manuscript.
Ethics approval
IRB approval is not required.
Data availability statement
Data are available on request to the corresponding author. All data relevant to the study are included in the article or uploaded as supplementary information All data that are publicly available and used in the writing of this article in the text and the reference list.
Funding
Monitoraggio ambientale, studio ed approfondimento della salute della popolazione residente in aree a rischio—In attuazione della D.G.R. Campanian.180/2019. POR Campania FESR 2014–2020 Progetto “Sviluppo di Approcci Terapeutici Innovativi per patologie Neoplastiche resistenti ai trattamenti—SATIN”. This work has been partly supported by a grant from the Italian Health Ministry’s research program (ID: NET-2016-02363853). National Center for Gene Therapy and Drugs based on RNA Technology MUR-CN3 CUP E63C22000940007 to DS.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Francesco Pepe has received personal fees as speaker bureau from Menarini, 10.13039/100004337Roche, Thermofisher for work performed outside of the current study. Konstantinos Venetis has received honoraria for speaker bureau from Merck Sharp & Dohme (MSD), Roche, and AstraZeneca. "Cristian Scatena reports speaker bureau for Astra Zeneca, 10.13039/501100022274Daiichi Sankyo, Cerca Biotech, 10.13039/100005564Gilead, MSD; advisory role for Astra Zeneca, 10.13039/501100022274Daiichi Sankyo, 10.13039/100030841Exact Sciences, Menarini; consulting for Astra Zeneca, 10.13039/501100022274Daiichi Sankyo, 10.13039/100005564Gilead, Menarini, MSD; research grants from 10.13039/100005564Gilead. Giancarlo Troncone reports personal fees (as speaker bureau or advisor) from 10.13039/100004337Roche, 10.13039/100030732MSD, 10.13039/100004319Pfizer, Boehringer Ingelheim, Eli Lilly, BMS, GSK, Menarini, 10.13039/100004325AstraZeneca, 10.13039/100002429Amgen and 10.13039/100004326Bayer, unrelated to the current work. Nicola Fusco has received honoraria for consulting, advisory role, speaker bureau, travel, and/or research grants from 10.13039/100009947Merck Sharp & Dohme (10.13039/100030732MSD), 10.13039/100004334Merck, 10.13039/100004336Novartis, 10.13039/100004325AstraZeneca, 10.13039/100004337Roche, 10.13039/501100014337Menarini Group, 10.13039/501100022274Daiichi Sankyo, 10.13039/100004330GlaxoSmithKline (GSK), 10.13039/100005564Gilead, 10.13039/100017981Sysmex, 10.13039/100008067Genomic Health, 10.13039/100018771Veracyte, Sakura, 10.13039/501100018828Leica Biosystems, Lilly, 10.13039/100004319Pfizer, ThermoFisher, Abbvie. Umberto Malapelle has received personal fees (as consultant and/or speaker bureau) from Boehringer Ingelheim, 10.13039/100004337Roche, 10.13039/100030732MSD, 10.13039/100002429Amgen, 10.13039/100011033Thermo Fisher Scientific, Eli Lilly, Diaceutics, GSK, 10.13039/100004334Merck and 10.13039/100004325AstraZeneca, Janssen, Diatech, 10.13039/100004336Novartis and Hedera unrelated to the current work. Umberto Malapelle is Editor in chief of Journal of Liquid Biopsy, Francesco Pepe and Nicola Fusco are member of Editorial Board of the Journal of Liquid Biopsy. No other competing interests to be declared for the remaining authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jeselsohn R.Yelensky R.Buchwalter G.Frampton G.Meric-Bernstam F.Gonzalez Angulo A.M.Emergence of constitutively active estrogen receptor-α mutation in pretreated advanced estrogen receptor-positive breast cancer Clin Cancer Res 202014175717672439804710.1158/1078-0432.CCR-13-2332 PMC 3998833 · doi ↗ · pubmed ↗
- 2Bidard F.-C.Kaklamani V.G.Neven P.Streich G.Montero A.J.Forget F.Elacestrant (oral selective estrogen receptor degrader) versus standard endocrine therapy for estrogen receptor-positive, human epidermal growth factor receptor 2–negative advanced breast cancer: results from the randomized phase III EMERALD trial J Clin Oncol 402022324632563558433610.1200/JCO.22.00338 PMC 9553388 · doi ↗ · pubmed ↗
- 3Mc Andrew N.P.Finn R.S.Clinical review on the management of hormone receptorpositive metastatic breast cancer JCO Oncol Pract 1820213193273463732310.1200/OP.21.00384 · doi ↗ · pubmed ↗
- 4Dustin D.Gu G.Fuqua S.A.W.ESR 1 mutations in breast cancer Cancer 1252019371437283131844010.1002/cncr.32345 PMC 6788940 · doi ↗ · pubmed ↗
- 5Lloyd M.R.Wander S.A.Hamilton E.Razavi P.Bardia A.Next-generation selective estrogen receptor degraders and other novel endocrine therapies for management of metastatic hormone receptor-positive breast cancer: current and emerging role Ther Adv Med Oncol 14202210.1177/17588359221113694 PMC 934090535923930 · doi ↗ · pubmed ↗
- 6Nagy Z.Jeselsohn R.ESR 1 fusions and therapeutic resistance in metastatic breast cancer Front Oncol 12202310.3389/fonc.2023.1155540 PMC 1002635836950546 · doi ↗ · pubmed ↗
- 7Betz M.Massard V.Gilson P.Witz A.Dardare J.HarléA.Merlin J.L.ESR 1 gene mutations and liquid biopsy in ER-positive breast cancers: a small step forward, a giant leap for personalization of endocrine therapy?Cancers (Basel)15202351693795834310.3390/cancers 15215169 PMC 10649433 · doi ↗ · pubmed ↗
- 8Grinshpun A.Chen V.Sandusky Z.M.Fanning S.W.Jeselsohn R.ESR 1 activating mutations: from structure to clinical application Biochim Biophys Acta Rev Cancer 1878202318883010.1016/j.bbcan.2022.18883036336145 · doi ↗ · pubmed ↗