Treatment With Phosphodiesterase 5 Inhibitors and Long‐Term Outcomes in Patients Undergoing Coronary Angiography and Cardiac Catheterization
Sumon Roy, Annette Min, Edward O. McFalls, Robert A. Perera, Fadi N. Salloum, Ion S. Jovin

TL;DR
This study found that using PDE5 inhibitors does not increase the risk of major cardiovascular events in patients undergoing heart procedures.
Contribution
The study provides new evidence on the long-term cardiovascular safety of PDE5 inhibitors in a clinical setting.
Findings
PDE5 inhibitor users had a lower MACE rate compared to non-users before matching.
After matching, no significant difference in MACE was found between the groups.
Multivariable analysis showed no significant association between PDE5 inhibitors and MACE.
Abstract
The effects of phosphodiesterase 5 (PDE5) inhibitors on the incidence of long‐term outcomes in patients with cardiovascular disease are not well understood. Objective: We studied the association between PDE5 inhibitor therapy and the incidence of adverse cardiovascular major adverse cardiovascular events (MACE) in patients undergoing coronary angiography and intervention. We studied 4582 consecutive patients undergoing coronary angiography and intervention. The incidence of MACE at 1 year, defined as urgent revascularization, myocardial infarction, admission for heart failure or all‐cause death, was considered the primary outcome. Of the 4582 patients, 562 (12.3%) had current prescriptions for PDE5 inhibitors before the procedure and 4020 (87.7%) did not. The incidence of MACE was 171 (30.4%) among patients of the PDE5 inhibitor group versus 1482 (36.9%) in the non‐PDE5 inhibitor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
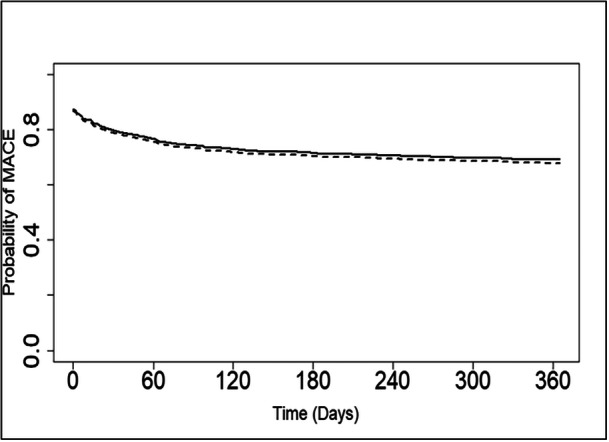 Figure 1
Figure 1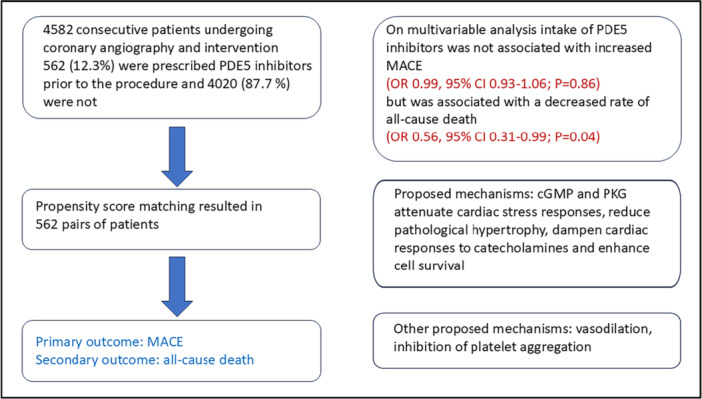 Central Illustration 1
Central Illustration 1| Overall | PDE5 inhibitor | No PDE5 inhibitor |
| |
|---|---|---|---|---|
|
|
|
| ||
| Male (%) | 4416 (96.4) | 561 (99.8) | 3855 (95.9) | < 0.001 |
| Age (mean [SD]) | 64.72 (9.71) | 62.40 (8.18) | 65.04 (9.86) | < 0.001 |
| BMI (mean [SD]) | 30.83 (6.61) | 31.15 (6.10) | 30.79 (6.68) | 0.22 |
| African American (%) | 1694 (37.0) | 300 (53.4) | 1394 (34.7) | < 0.001 |
| Creatinine (mean [SD] [mg/dL]) | 1.42 (1.40) | 1.47 (1.57) | 1.42 (1.37) | 0.40 |
| CAD (%) | 2463 (53.8) | 169 (30.1) | 2294 (57.1) | < 0.001 |
| HTN (%) | 3783 (82.6) | 467 (83.1) | 3316 (82.5) | 0.76 |
| AFIB (%) | 530 (11.6) | 51 (9.1) | 479 (11.9) | 0.05 |
| CHF (%) | 984 (21.5) | 104 (18.5) | 880 (21.9) | 0.07 |
| DM (%) | 2157 (47.1) | 279 (49.6) | 1878 (46.7) | 0.20 |
| PVD (%) | 449 (9.8) | 31 (5.5) | 418 (10.4) | < 0.001 |
| COPD (%) | 871 (19.0) | 81 (14.4) | 790 (19.7) | 0.004 |
| CKD (%) | 860 (18.8) | 84 (14.9) | 776 (19.3) | 0.01 |
|
| ||||
| ASA (%) | 3554 (77.6) | 428 (76.2) | 3126 (77.8) | 0.42 |
| Plavix (%) | 936 (20.4) | 61 (10.9) | 875 (21.8) | < 0.001 |
| Beta Blocker (%) | 2963 (64.7) | 299 (53.2) | 2664 (66.3) | < 0.001 |
| ACEI/ARB (%) | 2503 (54.6) | 303 (53.9) | 2200 (54.7) | 0.75 |
| Statin (%) | 3316 (72.4) | 405 (72.1) | 2911 (72.4) | 0.90 |
| Insulin (%) | 1004 (21.9) | 121 (21.5) | 883 (22.0) | 0.85 |
| Metformin (%) | 952 (20.8) | 139 (24.7) | 813 (20.2) | 0.01 |
|
| ||||
| Indication | ||||
| Chest pain (%) | 3042 (66.4) | 372 (66.2) | 2670 (66.4) | 0.09 |
| CHF/cardiomyopathy (%) | 673 (14.7) | 86 (15.3) | 587 (14.6) | |
| ACS (%) | 538 (11.7) | 53 (9.4) | 485 (12.1) | |
| Other (%) | 329 (7.2) | 51 (9.1) | 278 (6.9) | |
| Findings | ||||
| Non‐obstructive CAD (%) | 1899 (41.4) | 287 (51.1) | 1612 (40.1) | < 0.001 |
| Significant CAD (%) | 2683 (58.6) | 275 (48.9) | 2408 (59.9) | |
| Treatment | ||||
| CT Surgery (%) | 338 (7.4) | 41 (7.3) | 297 (7.4) | 0.07 |
| PCI (%) | 1076 (23.5) | 105 (18.9) | 971 (24.1) | |
| Medical (%) | 3168 (69.1) | 416 (73.8) | 2752 (68.5) | |
| Overall | PDE5 inhibitor | No PDE5 inhibitor |
| |
|---|---|---|---|---|
|
|
|
| ||
| MACE at 12 months (%) | 1653 (36.1) | 171 (30.4) | 1482 (36.9) | 0.003 |
| Death at 12 months (%) | 289 (6.3) | 19 (3.4) | 270 (6.7) | 0.003 |
| Overall | PDE5 inhibitor | No PDE5 inhibitor |
| |
|---|---|---|---|---|
|
|
|
| ||
| Male (%) | 1089 (96.9) | 561 (99.8) | 528 (94.0) | < 0.001 |
| Age (mean [SD]) | 62.55 (9.10) | 62.40 (8.18) | 62.69 (9.94) | 0.59 |
| BMI | 31.38 (6.61) | 31.15 (6.10) | 31.61 (7.09) | 0.25 |
| African American (%) | 521 (46.4) | 300 (53.4) | 221 (39.3) | < 0.001 |
| CAD (%) | 339 (30.2) | 169 (30.1) | 170 (0.2) | > 0.99 |
| HTN (%) | 940 (83.6) | 467 (83.1) | 473 (84.2) | 0.68 |
| AFIB (%) | 106 (9.4) | 51 (9.1) | 55 (9.8) | 0.75 |
| CHF (%) | 211 (18.8) | 104 (18.5) | 107 (19.0) | 0.87 |
| DM (%) | 561 (49.9) | 279 (49.6) | 282 (50.2) | 0.90 |
| PVD | 60 (5.3) | 31 (5.5) | 29 (5.2) | 0.89 |
| COPD (%) | 173 (15.4) | 81 (14.4) | 92 (16.4) | 0.40 |
| CKD (%) | 171 (15.2) | 84 (14.9) | 87 (15.5) | 0.86 |
|
| ||||
| ASA (%) | 854 (76.0) | 428 (76.2) | 426 (75.8) | 0.94 |
| Plavix (%) | 136 (12.1) | 61 (10.9) | 75 (13.3) | 0.23 |
| Beta blocker (%) | 586 (52.1) | 299 (53.2) | 287 (51.1) | 0.51 |
| ACEI/ARB (%) | 604 (53.7) | 303 (53.9) | 301 (53.6) | 0.95 |
| Statin (%) | 815 (72.5) | 405 (72.1) | 410 (73.0) | 0.78 |
| Insulin (%) | 255 (22.7) | 121 (21.5) | 134 (23.8) | 0.39 |
| Metformin (%) | 280 (24.9) | 139 (24.7) | 141 (25.1) | 0.94 |
|
| ||||
| Indication (%) | ||||
| Chest pain | 761 (67.7) | 372 (66.2) | 389 (69.2) | 0.63 |
| CHF/cardiomyopathy | 158 (14.1) | 86 (15.3) | 72 (12.8) | |
| ACS | 106 (9.4) | 53 (9.4) | 53 (9.4) | |
| Other | 99 (8.8) | 51 (9.1) | 48 (8.5) | |
| Findings (%) | ||||
| Non‐obstructive CAD | 577 (51.2) | 288 (51.1) | 289 (51.5) | 0.90 |
| Significant CAD | 547 (48.7) | 275 (48.9) | 272 (48.4) | |
| Treatment (%) | ||||
| CT Surgery | 88 (7.8) | 41 (7.3) | 47 (8.4) | 0.67 |
| PCI | 200 (17.8) | 106 (18.9) | 94 (16.7) | |
| Medical | 836 (74.4) | 413 (73.9) | 421 (74.9) | |
| Outcome | Predictor | Odds ratio | 95% CI |
|
|---|---|---|---|---|
| MACE at 12 months | ||||
| PDE5i | 0.99 | 0.93, 1.06 | 0.86 | |
| Age | 1.01 | 1.00, 1.01 | < 0.001 | |
| CHF | 0.90 | 0.83, 0.98 | 0.01 | |
| CKD | 1.03 | 0.93, 1.13 | 0.60 | |
| DM | 1.09 | 1.02, 1.17 | 0.01 | |
| Death at 12 months | ||||
| PDE5i | 0.56 | 0.31, 0.99 | 0.04 | |
| Age | 1.07 | 1.03, 1.1 | < 0.001 | |
| CHF | 2.53 | 1.38, 4.65 | 0.002 | |
| CKD | 1.34 | 1.18, 4.34 | 0.01 | |
| DM | 1.34 | 0.7, 2.55 | 0.37 | |
| Beta blocker | 0.81 | 0.46, 1.45 | 0.48 | |
| Statin | 0.63 | 0.34, 1.16 | 0.13 | |
|
Patients with cardiovascular disease are often denied therapy with PDE5 inhibitors because of concerns for cardiovascular risks We studied the outcomes of patients with cardiovascular disease who underwent coronary angiography and interventions and who had prescriptions for PDE5 inhibitors. We found no increase in major adverse cardiovascular events in patients who had prescriptions for PDE5 inhibitors We found that the patients who had PDE5 inhibitors prescriptions had a reduced all‐cause mortality |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Blood Pressure and Hypertension Studies · Cardiac Health and Mental Health
Introduction
1
Cardiovascular disease is the global leading cause of death. The World Health Organization (WHO) estimated the number deaths in 2016 from cardiovascular disease to be approximately 18 million people, and lifetime risk of cardiovascular disease exceeds 60% [1]. In the United States, about 700,000 people die yearly of cardiovascular disease, resulting in an estimated annual economic burden of over $200 billion [2, 3].
The coexistence of cardiovascular disease and erectile dysfunction (ED) is common likely due to both disease processes being driven, at least in part, by vascular dysfunction. The resultant high frequency of patients with cardiovascular disease being prescribed phosphodiesterase‐5 (PDE5) inhibitors for ED has driven efforts to identify the effects of PDE5 inhibitors on the cardiovascular system and clinical trials have studied the role of PDE5 inhibitors in cardiac disease [4, 5, 6, 7].
PDE5 inhibition has shown evidence of cardio‐protection in some but not all preclinical models [8, 9, 10]. Chronic administration of PDE5 inhibitors has shown promising results in reducing preclinical adverse cardiac outcomes [11, 12, 13]. However, these findings have not translated consistently as treatment for patients with congestive heart failure (CHF), myocardial infarction, or ventricular arrhythmia [5, 14, 15, 16, 17]. Therefore, despite well‐established safety and tolerance of PDE5 inhibitors, the unclear role of these medications in clinical cardiac pathologies has contributed to the lack of indications for prescribing PDE5 inhibitors in the treatment of cardiovascular disease [18] and has led to an insert package warning about potential risks in patients with coronary disease. Accordingly, we studied the effects of PDE5 inhibitors on the long‐term outcomes of patients referred for cardiac catheterization laboratory procedures.
Methods
2
Study Population
2.1
This was a retrospective chart review study done at a single Veterans Administration Medical Center, which serves as a referral center for several other medical centers. The study used the Veterans Healthcare Administration electronic medical records (CPRS) and was approved by the institutional medical board for exemption of consent.
We studied a cohort of 4582 consecutive patients who underwent coronary or peripheral angiography or intervention. All patients who underwent the procedures were included. This was a retrospective study and the follow‐up tests were ordered at the discretion of the physician providing care. Of the 4582 patients included, 562 patients (12.3%) had a PDE5 inhibitor prescription before the procedure and 4020 (87.7%) did not.
Outcomes
2.2
The primary outcome of this study was the composite incidence of major adverse cardiovascular events (MACE) at 1 year defined as urgent revascularization, myocardial infarction, admission for heart failure, or all‐cause death. The secondary endpoint was all‐cause death as a component of the composite primary outcome.
Statistics
2.3
A propensity score was calculated to determine the likelihood that a patient would receive PDE5 inhibitors based on a non‐parsimonious model that included variables such as age, gender, baseline creatinine and other baseline comorbid conditions such as CHF, and diabetes mellitus (DM), as well as medications such as angiotensin converting enzyme inhibitors (ACEI), beta blockers, statins, aspirin or metformin. A propensity score paired analysis was done to reduce the biases that are inherent with retrospective studies. As a sensitivity analysis, the propensity score was used as a covariate in the multivariate analysis. Odds ratios (OR) associated with the primary outcomes were calculated for individual exposures. Kaplan−Meier survival curves were made for the PDE5 inhibitors and no PDE5 inhibitors patient groups at 12 months using the data collected on deaths and other clinical outcomes.
Results
3
Study Population
3.1
Baseline characteristics of the study population are presented (Table 1). Briefly, this veteran population was predominantly male. The average age was 65 years, 37% of the patients were African American and the mean body mass index (BMI) was 31 kg/m^2^. The average baseline creatinine was 1.4 mg/dL (Table 2). The vast majority of patients had the diagnosis of hypertension (HTN), while approximately half of the cohort had the diagnoses of coronary artery disease (CAD) and/or DM. Approximately 20% of the study population had a history of CHF and/or chronic kidney disease (CKD).
Approximately 75% of the study population, regardless of concurrent PDE5 inhibitor use, were on home aspirin and insulin. The majority of patients were on home beta blocker and ACEI/angiotensin receptor blocker (ARB). In addition, approximately 20% of the overall study population were on home clopidogrel and metformin. Chest pain/angina (usually with a positive stress test) was the primary indication for cardiac catheterization in this study, while 12% of patients had signs or symptoms of acute coronary syndrome with or without ST elevation. Nearly 60% of patients were found to have significant CAD, and 24% of patients underwent PCI. The average volume of contrast used was 130 ml. In the propensity score matched cohort, the size of the patient cohort was smaller (1164 patients) but the groups (562 patients each) were well‐matched allowing for a valid comparison of the effects of treatment with PDE5 inhibitors (Table 2).
Effect of PDE5 Inhibitors on MACE and Other Long‐Term Outcomes
3.2
The composite incidence of MACE, defined as urgent revascularization, myocardial infarction, hospital admission for heart failure, or all‐cause death, was 30.4% in the PDE5 inhibitor group compared to 36.9% in the non‐PDE5 inhibitor group (171 vs 1482 patients, respectively; p = 0.003; Table 3). The secondary outcome measure of death from all causes occurred in 3.4% of the PDE5 inhibitor group compared to 6.7% of the non‐PDE5 inhibitor group (19 vs. 270 patients, respectively; p = 0.003; Table 3).
In the multivariable analysis (Table 4, Figure 1), there was no significant association between PDE5 inhibitor therapy and the risk of MACE at 12 months. However, there was a significant association between PDE5 inhibitor treatment and a decreased risk of death at 12 months (HR 0.56; 95% CI 0.31, 0.99; p = 0.04). The hazard ratios of the various baseline characteristics and 12‐month incidence of MACE revealed that age and a history of DM were significantly associated with an increased incidence of MACE (Table 4), while a h. We tested for the interaction between PDE5i intake and CHF, between PDE5i intake and CAD, and between PDE5i intake and CKD, with the outcome being MACE, and the interaction was not statistically significant in any of the tests. We also tested the same interactions between PDE5i intake and CHF, CAD, and CKD, with the outcome being survival at 12 months, and the interactions were not statistically significant in any of these tests either. Central Illustration 1.
Kaplan−Meier curves showing no difference in major adverse cardiac events (p = 0.85) of patients following cardiac catheterization who were on chronic PDE5 inhibitor therapy (solid line) compared to patients who were not on chronic PDE5 inhibitor therapy (dashed line).
cGMP, cyclic guanidyl monophosphate; MACE, major adverse cardiovascular events; PDE5, phosphodiesterase 5; PKG, protein kinase G. [Color figure can be viewed at wileyonlinelibrary.com]
Discussion
4
The frequent concurrence of cardiovascular disease and ED has led to a significant number of patients on PDE5 inhibitors who ultimately require coronary angiography and cardiac catheterization. This study was designed to investigate the association between PDE5 chronic therapy before coronary angiography/cardiac catheterization and MACE. Our data suggests that veterans on PDE5 inhibitors who undergo cardiac catheterization do not have an increased risk of MACE at 1 year. At the same time the data shows that there is an association between a reduced risk of all cause death and the intake of PDE5 inhibitors (Table 5).
The overall effect of PDE5 inhibition in myocardial ischemia seems to be beneficial, but evidence is largely preclinical with inconsistent results in the clinical setting. Early studies in animal models showed improved ventricular recovery, decreased myocardial infarction, and reduced ventricular infarct size following ischemia‐reperfusion injury and PDE5 inhibition [9, 19]. Findings from a meta‐analysis suggested that chronic PDE5 inhibitor use imparts a beneficial cardiac inotropic effect together with anti‐remodeling properties across different populations, suggesting that patients with longstanding cardiac disease could benefit from PDE5 inhibition‐induced cardio‐protection [4]. However, in another study, the effect of PDE5 inhibition on exercise tolerance times was neutral in patients with stable CAD [16]. Taken together, there is some evidence that PDE5 inhibition could be beneficial in ischemic coronary disease [7]. Our study is a retrospective study that did not investigate the mechanisms that could lead to improved outcomes in cardiac patients who are prescribed PDE5 inhibitors. However, proposed mechanisms are the activation of cGMP and PKG which can attenuate cardiac stress responses, reduce pathological hypertrophy, dampen cardiac responses to catecholamines and enhance cell survival. Other proposed mechanisms are vasodilation and inhibition of platelet aggregation [7, 20, 21],
A study in Swedish men with first myocardial infarction found that treatment with PDE5 inhibitors was associated with a lower risk of death and cardiovascular events [22]. This study had a control group which was not receiving any treatment for ED, potentially resulting in confounding for indication. This led to a recent subsequent study investigating the association between PDE5 inhibition versus prostaglandin E1 in men with stable CAD [23]. Results from this study showed that in men with stable CAD, treatment with PDE5 inhibitor was associated with lower cardiovascular outcomes including death, myocardial infarction, heart failure, and revascularization [23]. Because the study was observational, no inferences on causality can be made.
Findings from the present study offer an additional perspective of potential benefit from chronic PDE5 inhibition. Together with current literature, our findings support the notion that PDE5 inhibition is not deleterious and could be beneficial in treating patients with cardiovascular disease. Though the mechanism remains unclear as to how PDE5 inhibition could result in a reduction in all‐cause death, these findings are significant because of the widespread use of PDE5 inhibitors for the treatment of ED, as well as common use in advanced pulmonary hypertension [24], and off‐label use in the management of high‐altitude pulmonary edema [25], Raynaud phenomenon [26], and colorectal cancer as adjuvant therapy [27]. Interestingly, a recently published meta‐analysis suggests that intake of PDE5 inhibitors by patients without known cardiovascular disease is associated with reduced risks of both MACE and all cause death [28]. However, our study population was different because it had known or suspected cardiovascular disease of sufficient severity to warrant a cardiac catheterization/coronary angiography. This may account for the better results of the meta‐analysis compared to the results of our study. Finally, a recently published study in a large US based hospital database found a reduction in all‐cause death (as well as stroke and venous thromboembolism) in patients taking PDE5 inhibitors, consistent with our findings [29].
Limitations of this study include the retrospective design of the study. Because of this, the findings can only be considered as hypothesis‐generating. In addition, because this study was conducted at a Veterans Administration Medical Center, the population investigated was predominantly male and may be slightly older than the typical population of patients undergoing cardiac catheterization. Because of this, extrapolation to female and younger patients should be done with caution. Another limitation is the fact that we do not have information about how many patients were actually taking the PDE5i since the data that we collected pertains to prescriptions only. However, if only a small fraction of patients were indeed taking the medications prescribed this would skew the results more toward the null hypothesis. There is also incertitude regarding how many tablets the patients were taking and whether there is a chronic effect of PDE5i in patients who take the medication on an as needed basis. The VA offers four doses per month free of charge to the veterans as part of the pharmacy benefits, but we do not have information about how the tablets were taken. However, a study investigating the intake of PDE5 inhibitors in a random sample of 24,745 veterans over 66 years of age [30] showed that most of them who filled a prescription for PDE5i only filled it through VA pharmacies and only 3% were also getting prescriptions through Medicare.
Conclusion
5
In conclusion, our study showed that in a population of United States veterans undergoing coronary angiography/cardiac catheterization, chronic intake of PDE5 inhibitors was not associated with a significantly reduced rate of MACE but was associated with a significantly reduced risk of death at 1 year after the procedure. Further prospective, large‐scale trials are needed to confirm whether starting therapy with PDE5 inhibitors in patients undergoing coronary angiography/cardiac catheterization can improve long‐term outcomes in these patients.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. Garcia and J. Burkle , “New and Future Parenteral Therapies for the Management of Lipid Disorders,” Archives of Medical Research 49 (2018): 538–547.30739730 10.1016/j.arcmed.2019.01.001 · doi ↗ · pubmed ↗
- 2C. D. Fryar , T. C. Chen , and X. Li , Prevalence of Uncontrolled Risk Factors for Cardiovascular Disease: United States, 1999‐2010. NCHS Data Brief (2012), 1–8.23101933 · pubmed ↗
- 3M. Writing Group , D. Mozaffarian , E. J. Benjamin , et al., “Heart Disease and Stroke Statistics‐2016 Update: A Report From the American Heart Association,” Circulation 133 (2016): e 38–e 360.26673558 10.1161/CIR.0000000000000350 · doi ↗ · pubmed ↗
- 4E. Giannetta , T. Feola , D. Gianfrilli , et al., “Is Chronic Inhibition of Phosphodiesterase Type 5 Cardioprotective and Safe? A Meta‐Analysis of Randomized Controlled Trials,” BMC Medicine 12 (2014): 185.25330139 10.1186/s 12916-014-0185-3PMC 4201993 · doi ↗ · pubmed ↗
- 5M. Guazzi , M. Samaja , R. Arena , M. Vicenzi , and M. D. Guazzi , “Long‐Term Use of Sildenafil in the Therapeutic Management of Heart Failure,” Journal of the American College of Cardiology 50 (2007): 2136–2144.18036451 10.1016/j.jacc.2007.07.078 · doi ↗ · pubmed ↗
- 6M. M. Redfield , H. H. Chen , B. A. Borlaug , et al., “Effect of phosphodiesterase‐5 Inhibition on Exercise Capacity and Clinical Status in Heart Failure With Preserved Ejection Fraction: A Randomized Clinical Trial,” Journal of the American Medical Association 309 (2013): 1268–1277.23478662 10.1001/jama.2013.2024 PMC 3835156 · doi ↗ · pubmed ↗
- 7S. Roy , R. A. Kloner , F. N. Salloum , and I. S. Jovin , “Cardiac Effects of Phosphodiesterase‐5 Inhibitors: Efficacy and Safety,” Cardiocasular Drugs and Therapy 37 (2023): 793–806.10.1007/s 10557-021-07275-y PMC 901047934652581 · doi ↗ · pubmed ↗
- 8R. Kukreja , X. L. Tang , D. Lefer , et al., “Administration of Sildenafil at Reperfusion Fails to Reduce Infarct Size: Results From the CAESAR Cardioprotection Consortium (LB 650),” FASEB Journal 28 (2014): LB 650.