Mycobacterium genavense-induced spindle cell pseudotumor presenting with symptoms of giant cell arteritis
Britney Le, Guilherme Kuceki, Jamie Zussman

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
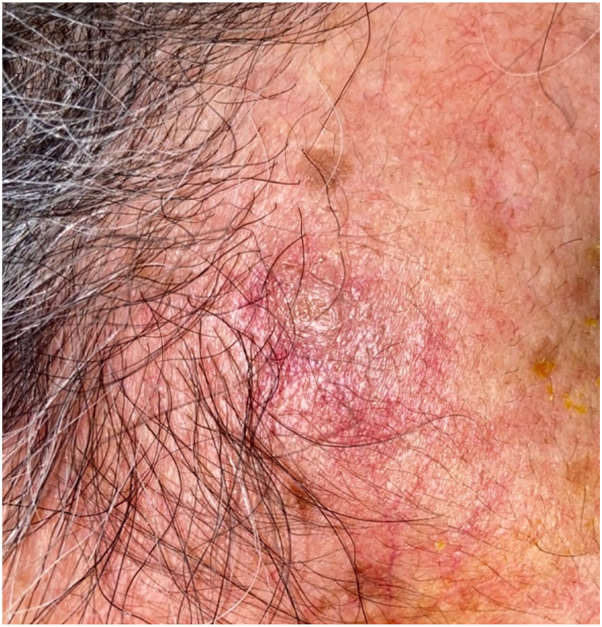 Figure 1
Figure 1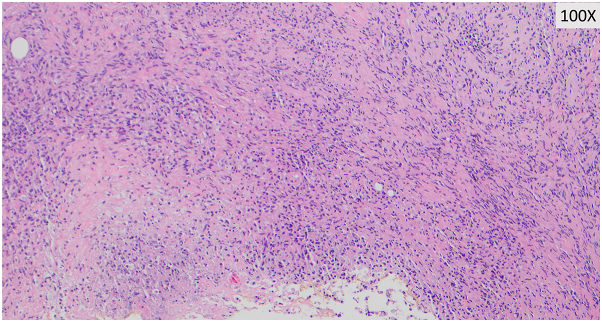 Figure 2
Figure 2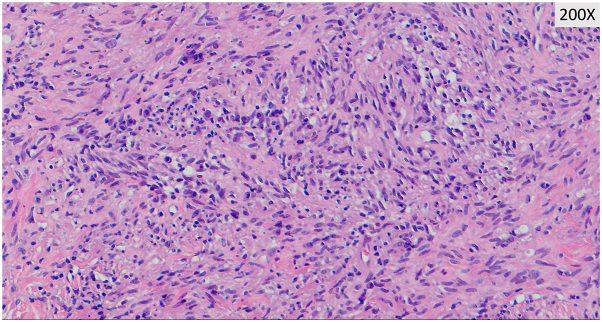 Figure 3
Figure 3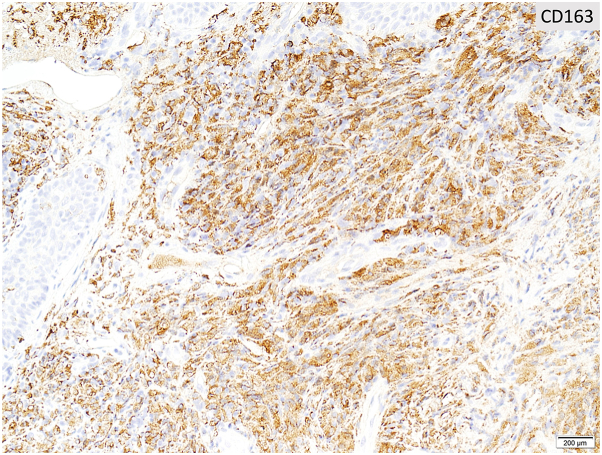 Figure 4
Figure 4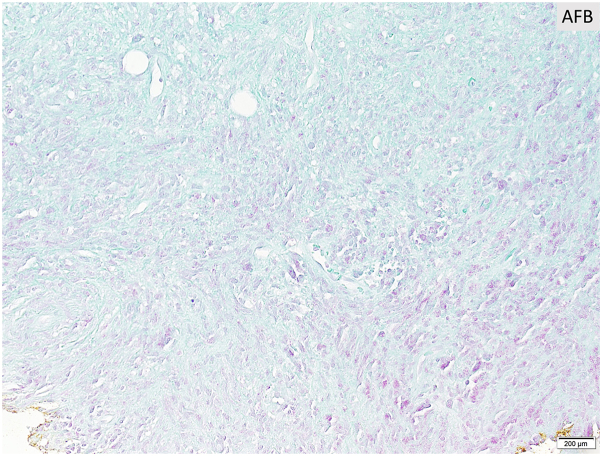 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Autoimmune and Inflammatory Disorders · Gastrointestinal Tumor Research and Treatment
Case description
An 80-year-old woman with poorly controlled diabetes (HbA1c 11.9%) presented with a painful, edematous, erythematous 1 cm nodule on the right temple. She reported a history of giant cell arteritis (GCA) 2 years earlier, for which she had received systemic corticosteroids but was lost to follow-up. A review of records revealed that a right temporal artery biopsy at that time was negative for arteritis. Due to ongoing concern for GCA, a temporal artery biopsy of the left side was obtained, which was also negative for arteritis. The right temple nodule was not biopsied at the time. Head computed tomography angiography showed a right temple subcutaneous soft tissue nodule and stranding, thought to be from the biopsy obtained 2 years earlier. Chest computed tomography revealed pulmonary calcified granulomas and calcified hilar lymphadenopathy, consistent with prior granulomatous disease. She was prescribed a systemic corticosteroid taper and referred to rheumatology, where a clinical diagnosis of GCA was made. Tocilizumab was initiated after latent tuberculosis, and Coccidioides were deemed unlikely. Notably, the interferon gamma release assay was twice indeterminate. Lung biopsy was deferred due to stability on repeat imaging.
After 3 months of tocilizumab and prednisone therapy, she returned with a right-sided headache and was treated for a presumed GCA flare. Two months later, during an admission for chest pain, she reported worsening pain and enlargement of the nodule on her temple. She denied recent dental, cosmetic, or surgical procedures prior to lesion development. Dermatology consult revealed a tender, red-brown papule overlying an indurated nodular plaque (Fig 1). Histopathology revealed diffuse spindled and epithelioid cells with necrosis, leukocytoclasis, and lymphoplasmacytic aggregates raising suspicion of mycobacterial infection (Figs 2 and 3). Immunohistochemistry was positive for CD163 (Fig 4), CD68, and CD31 and negative for AE1/AE3, SOX10, S100, CD34, and smooth muscle actin. Acid-fast bacillus stain showed abundant organisms (Fig 5); Gram and periodic acid–schiff were negative. Polymerase chain reaction confirmed Mycobacterium genavense. Tocilizumab was discontinued shortly after. She was treated with a combination antimicrobial therapy (rifabutin, moxifloxacin, azithromycin) for 12 months due to concern for disseminated infection. A follow-up biopsy demonstrated complete histologic resolution. She has now been off treatment for over 1 year, and her symptoms have remained completely resolved.Fig 1. Clinical photo of the right temple at the time of first skin biopsy.Fig 2. Dermal infiltrate of spindled histiocytes with interspersed lymphoplasmacytic inflammation.Fig 3. Higher magnifications reveal diffuse sheets of spindle-shaped histiocytes with foci of necrosis and leukocytoclasis.Fig 4A CD163 is strongly positive in the histiocytes.Fig 5AFB stain highlights innumerable acid-fast bacilli at the base of the specimen within and surrounding the areas of necrosis. AFB, acid-fast bacillus stain.
Question 1: An 80-year-old woman with poorly controlled diabetes and a history of presumed GCA presents with a painful, enlarging right temple nodule. After multiple courses of corticosteroids and later tocilizumab, the lesion progresses. A biopsy months later reveals acid-fast bacilli and polymerase chain reaction confirms Mycobacterium genavense. Which of the following most likely contributed to the delayed diagnosis?
- **A.**Reliance on inflammatory markers such as erythrocyte sedimentation rate in guiding immunosuppressive therapy.
- **B.**Misinterpretation of temporal artery biopsy results as falsely negative.
- **C.**Diagnostic anchoring on prior presumptive GCA without investigating the evolving lesion.
- **D.**Underappreciation of cutaneous mycobacterial infections in diabetic patients.
- **E.**Failure to recognize imaging evidence of granulomatous disease as clinically relevant.
Answer discussion:
- **C.**Correct. This case is unusual as the lesion’s location possibly contributed to symptoms mimicking GCA. It remains unclear whether her clinical course can be fully attributed to mycobacterial infection or if a component of GCA is also present; immunosuppressives likely contributed to the progression of the disease. Mycobacterial spindle cell pseudotumors are rare and most commonly caused by Mycobacterium avium complex or Mycobacterium tuberculosis.1 Their resemblance to neoplastic processes, such as Kaposi sarcoma or spindle cell melanomas, complicates diagnosis.2 M. genavense is a fastidious nontuberculous mycobacterium, often underdiagnosed due to its slow growth in culture. It is commonly found in gastrointestinal tracts and environmental sources, with infections primarily reported in patients with HIV or iatrogenic immunosuppression.3 Early recognition and accurate diagnosis of mycobacterial spindle cell pseudotumor are crucial, as M. genavense infections carry a mortality rate of ∼30% but are curable in over 50% of cases with timely treatment.4^,^5
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sfeir M.M.Schuetz A.Van Besien K.Mycobacterial spindle cell pseudotumour: epidemiology and clinical outcomes J Clin Pathol 71720186266302936730110.1136/jclinpath-2017-204777 · doi ↗ · pubmed ↗
- 2Yeh I.George E.Jokinen C.H.Cutaneous mycobacterial spindle cell pseudotumor: a potential mimic of soft tissue neoplasms Am J Dermatopathol 3362011 e 66e 692171268610.1097/DAD.0b 013e 3182120 ae 3 · doi ↗ · pubmed ↗
- 3Coelho R.Hanna R.Flagg A.Mycobacterium genavense-induced spindle cell pseudotumor in a pediatric hematopoietic stem cell transplant recipient: case report and review of the literature Transpl Infect Dis 1922017 e 1265610.1111/tid.1265628039955 · doi ↗ · pubmed ↗
- 4Mahmood M.Ajmal S.Abu Saleh O.M.Bryson A.Marcelin J.R.Wilson J.W.Mycobacterium genavense infections in non-HIV immunocompromised hosts: a systematic review Infect Dis (Lond)505May 201832933910.1080/2344235.2017.140463029157060 · doi ↗ · pubmed ↗
- 5Baldolli A.Chocron R.Dargère S.Mycobacterium genavense infections in immunocompromised patients without HIV: case series of solid organ transplant patients and literature review Open Forum Infect Dis 910202210.1093/ofid/ofac 498PMC 958546936285177 · doi ↗ · pubmed ↗