Mohs surgical postoperative wound infection caused by rare Enterobacteriaceae, Raoultella planticola
Jena C. Jacobs, Mario J. Sequeira

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1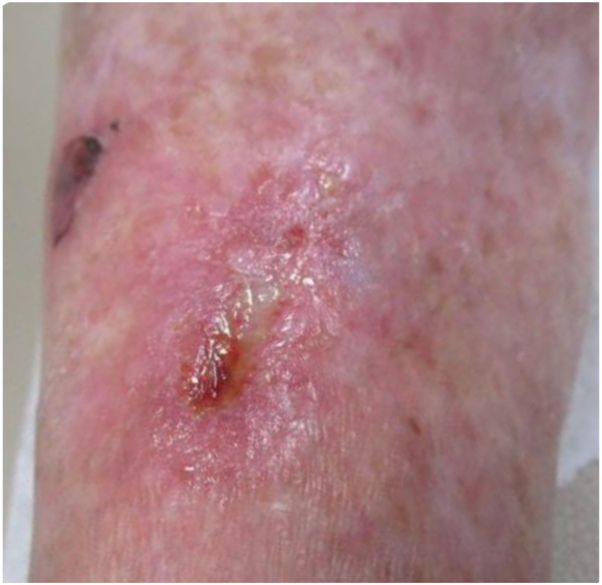 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPlant Pathogenic Bacteria Studies · Infections and bacterial resistance · Bacterial biofilms and quorum sensing
Introduction
Raoultella planticola (R. planticola) is a gram-negative, anaerobic, rod-shaped bacterium, belonging to the Enterobacteriaceae family.1 It was first found in humans in 1984 in a patient with sepsis and was originally classified as the Klebsiella spp., until 2001 when it was reclassified as a member of the Raoultella genus based on phylogenetic gene analysis.2 Initially it was considered a harmless environmental organism primarily found in soil and water.2 However, in recent years, it has emerged as a virulent pathogen closely associated with multiple severe human infections, including liver abscesses, cholangitis, pancreatitis, conjunctivitis, acute cholecystitis, urinary tract infections, and pneumonia.3 The reported cases involving skin infections were linked to a dog scratch, fatal bacteremia following burn wounds exposed to contaminated rainwater used to extinguish a flesh fire, a fractured tibia after an open reduction internal fixation, pelvic cellulitis in a neutropenic patient, and a crush injury of the thumb in a dirty environment washed with running water.4, 5, 6, 7, 8
In this study, we report an 85-year-old woman with a R. planticola wound infection of the right lower extremity following Mohs micrographic surgery. We aim to shed light on the rare potential for this organism to infect surgical wounds and cause delayed wound healing. To our knowledge, no cases of R. planticola have been reported in the setting of postsurgical wound infections following Mohs surgery.
Case report
An 85-year-old woman presented to our Cancer Center on February 10, 2023 for Mohs micrographic surgical excision of a squamous cell carcinoma keratoacanthoma type, located on her right shin. Her past medical history included malignant melanoma, squamous cell carcinoma, basal cell carcinoma, seborrheic dermatitis, Grover’s disease, deep vein thrombosis, hyperlipidemia, and thyroid dysfunction. Her medications included ketoconazole 2% shampoo, levothyroxine 50 mcg, rosuvastatin calcium 40 mg, enoxaparin sodium 60 mg/0.6 mL, rivaroxaban 20 mg, and multivitamin. The patient drank 5 alcoholic beverages a day and had never smoked. Preoperative review of systems and physical examination were unremarkable; she appeared in good health, well nourished, and alert.
The surgical team conducted proper wound preparation using chlorhexidine scrub, sterile draping, and gloving. The squamous cell carcinoma keratoacanthoma, measuring 1.3 cm, was excised in a single stage, resulting in a 1.7-cm defect (Fig 1, A and B). Closure was achieved with 3 deep 4.0 polyglactin 910 sutures, one superficial interrupted and one running 4.0 nylon suture, resulting in a 2.7 cm linear repair (Fig 1, C). A Telfa nonadherent pad, mupirocin ointment, sterile gauze, and paper tape were applied as a pressure dressing.Fig 1A, SCCKA, measuring 1.3 cm on the anterior right shin, denoted by yellow circle. B, Mohs defect, 1.7 cm. C, Final closed repair. SCCKA, Squamous cell carcinoma keratoacanthoma.
Fourteen days postsurgery, on February 24, 2023, the patient returned for suture removal. Examination revealed a dry, well-approximated wound with no erythema or drainage. However, 3 days later, on February 27, 2023, she reported abnormal wound healing. Physical examination revealed a superficial wound with mild erythema, granulation tissue, fibrinous slough, and an overlying crust. A scant amount of odorless, clear transudate was present, which was cultured, yielding heavy growth of Raoultella planticola (Fig 2) (Table I).Fig 2. Infected surgical wound.Table IBacterial culture and sensitivitiesCulture, aerobic bacteria Micro number16615949 Specimen sourceRight shin Specimen qualityAdequate ResultHeavy growth of Raoultella (Klebsiella) planticola CommentSkin flora also present AntibioticsSusceptibility (MIC) Amoxicillin/clavulanateS/≤2 mcg/mL AmpicillinR/8 mcg/mL Ampicillin/sulbactamS/≤2 mcg/mL CefazolinNR/≤4 mcg/mL ∗∗1 CefepimeS/≤1 mcg/mL CeftazidimeS/≤1 mcg/mL CeftriaxoneS/≤1 mcg/mL CiprofloxacinS/≤0.12 mcg/mL GentamicinS/≤1 mcg/mL ImipenemS/0.5 mcg/mL LevofloxacinS/≤0.12 mcg/mL Piperacillin/tazobactamS/≤4 mcg/mL TobramycinS/≤1 mcg/mL Trimethoprim/sulbactamS/≤20 mcg/mLTherapy comments: Note ∗∗1: For infections other than uncomplicated UTI caused by Escherichia coli, Klebsiella pneumonia, or Proteus mirabilis, cefazolin is resistant of MIC > or = 8 mcg/mL (distinguishing susceptible vs intermediate for isolates with MIC ≤4 mcg/mL requires additional testing).I, Intermediate; MIC, minimal inhibitory concentration; NR, not reported; R, resistant; S, susceptible.
Antibiotic susceptibility testing identified multiple effective treatments. The patient was prescribed oral amoxicillin/clavulanate (500/125 mg twice daily), topical gentamicin ointment (0.1% twice daily), along with aluminum acetate solution (Domeboro) daily soaks. By her follow-up on March 27, 2023, the oral antibiotic course was completed, but the wound displayed persistent granulation tissue and transudate. Wound debridement was performed, and daily cadexomer iodine gel (Iodosorb) application was initiated. The patient returned on April 03, 2023 with concerns of nonhealing wound, and a repeat culture identified only Proteus mirabilis sensitive to amoxicillin/clavulanate. A new course of amoxicillin-clavulanate (500/125 mg twice daily for 10 days), aluminum acetate solution soaks, and daily Iodosorb gel application were prescribed. On April 24, 2023, 10 weeks after the initial Mohs procedure, the wound was fully healed with no signs of infection (Fig 3).Fig 3. Healing wound with residual crust and postinflammatory redness.
Discussion
This case adds to the limited literature on R. planticola as a rare but significant pathogen in wound infections, particularly following surgical interventions. This gram-negative organism is traditionally associated with environmental sources, such as contaminated water and soil, and is very infrequently implicated in human infections. Notably, R. planticola infections have been documented in cholangitis, urinary infections, and systemic bacteremia. However, cases involving skin infections remain extremely rare, especially in surgical wounds, as seen here. This patient’s history of malignancy and her lesion’s location on the lower extremity could have contributed to the infection, as certain regions, like the lower limbs, are more susceptible to delayed healing due to compromised vascularity and proximity to potential environmental contamination. Her hobby of gardening likely placed her at an increased risk. R. planticola strains are usually susceptible to third-generation or fourth-generation cephalosporins, Beta-lactamase inhibitor combinations, aminoglycosides, ciprofloxacin, levofloxacin, tigecycline, and carbapenems.9 Although R. planticola infections are rare, especially in dermatologic surgery, awareness of this pathogen’s potential role in wound infections is crucial. Early culture and sensitivity testing, along with tailored antibiotic therapy, can significantly improve patient outcomes by mitigating complications and reducing morbidity associated with delayed wound healing. This case also emphasizes the value of follow-up and reassessment in wound management, particularly when initial treatment fails to resolve the infection fully.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hu A.Y.Leslie K.A.Baskette J.Elsayed S.Raoultella planticola bacteraemia J Med Microbiol 61Pt 1020121488148910.1099/jmm.0.041129-022820690 · doi ↗ · pubmed ↗
- 2Drancourt M.Bollet C.Carta A.Rousselier P.Phylogenetic analyses of Klebsiella species delineate Klebsiella and Raoultella gen. nov., with description of Raoultella ornithinolytica comb. nov., Raoultella terrigena comb. nov. and Raoultella planticola comb. nov Int J Syst Evol Microbiol 51Pt 3200192593210.1099/00207713-51-3-92511411716 · doi ↗ · pubmed ↗
- 3Xu M.Xie W.Fu Y.Zhou H.Zhou J.Nosocomial pneumonia caused by carbapenem-resistant Raoultella planticolla: a care report and literature review Infection 432201524524810.1007/s 15010-015-0722-925595510 · doi ↗ · pubmed ↗
- 4Yumoto T.Naito H.Ihoriya H.Raoultella planticola bacteremia-induced fatal septic shock following burn injury Ann Clin Microbiol Antimicrob 17120181910.1186/s 12941-018-0270-029728100 PMC 5934804 · doi ↗ · pubmed ↗
- 5Kalaria S.Elliott K.Combs N.Phillips L.G.Raoultella planticola: a rare cause of wound infection Wounds 29112017 E 103E 10529166257 · pubmed ↗
- 6Wolcott R.Dowd S.Molecular diagnosis of Raoultella planticola infection of a surgical site J Wound Care 198201032933210.12968/jowc.2010.19.8.7771020852504 · doi ↗ · pubmed ↗
- 7Al-Sawaf O.Garcia-Borrega J.Vehreschild J.J.Pelvic cellulitis caused by Raoultella planticolla in a neutropenic patient J Infect Chemother 254201929830110.1016/j.jiac.2018.09.01330482700 · doi ↗ · pubmed ↗
- 8O'Connell K.Kelly J.Niriain U.A rare case of soft-tissue infection caused by Raoultella planticolla Case Rep Med 2010201013408610.1155/2010/134086 PMC 292949220811592 · doi ↗ · pubmed ↗