Perceived stigma and the role of BMI on perceived HIV-related stigma among people living with HIV/AIDS in Southeast Ethiopia
Fikreab Desta, Demisu Zenbaba, Biniyam Sahiledengle, Shifera Metaferia, Tesfaye Desalegn, Degefa Gomora, Chala Kene, Girma Beressa, Telila Mesfin, Pammla Petruka, Lillian Mwanri

TL;DR
This study in Ethiopia found that underweight HIV patients and those with poor social support experience higher HIV-related stigma, with depression playing a mediating role.
Contribution
The study identifies BMI and depression as key factors in HIV-related stigma and reveals a chain mediation effect involving depression.
Findings
68% of participants experienced perceived HIV-related stigma.
Underweight (BMI <18.5) and poor social support significantly increased perceived stigma.
Depression indirectly predicted perceived HIV-related stigma through a chain mediation effect.
Abstract
People living with HIV/AIDS are at an increased risk of perceived HIV-related stigma. The effectiveness of social support for perceived HIV-related stigma is hampered by high depression. Although there is evidence that being underweight is associated with perceived HIV-related stigma, the mechanism is not well known. This study aimed to assess perceived HIV-related and the role of body mass index (BMI) on perceived HIV-related stigma in Southeast Ethiopia. A hospital-based cross-sectional study design was conducted among 547 randomly selected HIV/AIDS patients in Southeast Ethiopia. Perceived HIV-related stigma was assessed using a 10-item perceived HIV stigma scale assessment tool. Descriptive statistics were computed, and the data were analyzed by logistic regression, correlation, and mediation model. The magnitude of perceived HIV-related stigma was found to be 68% [95% CI: (64.1%,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1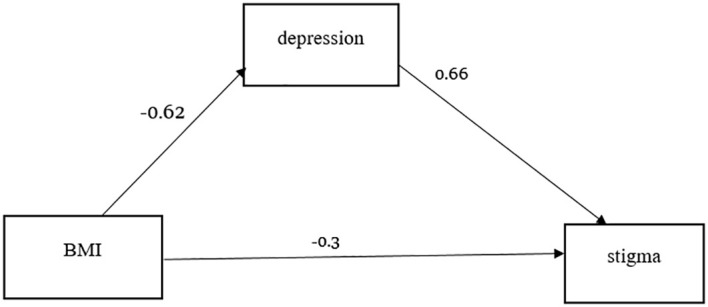 Figure 2
Figure 2| Variables | Frequency | Percent |
|---|---|---|
| Sex | ||
| Male | 274 | 50.1 |
| Female | 273 | 49.9 |
| Age category | ||
| 18–29 | 105 | 19.2 |
| 30–39 | 200 | 36.6 |
| 40–49 | 184 | 33.6 |
| ≥50 | 58 | 10.6 |
| Residence | ||
| Urban | 402 | 73.5 |
| Rural | 145 | 26.5 |
| Ethnicity | ||
| Oromo | 360 | 65.8 |
| Amhara | 164 | 30.0 |
| Others* | 23 | 4.2 |
| Religion | ||
| Protestant | 91 | 16.6 |
| Orthodox | 240 | 43.9 |
| Muslims | 197 | 36.0 |
| Catholic | 16 | 2.9 |
| Others** | 3 | 0.5 |
| Education status | ||
| Unable to read and write | 60 | 11.0 |
| Able to read and write | 104 | 19.0 |
| Primary school | 164 | 30.0 |
| Secondary or preparatory | 159 | 29.1 |
| College and University | 60 | 11.0 |
| Marital status | ||
| Single | 67 | 12.2 |
| Married | 340 | 62.2 |
| Widowed | 73 | 13.3 |
| Divorced | 67 | 12.2 |
| Occupation | ||
| Farmer | 126 | 23.0 |
| Housewife | 126 | 23.0 |
| Government employee | 114 | 20.8 |
| Daily laborer | 113 | 20.7 |
| Others*** | 68 | 12.4 |
| Income level | ||
| ≤500 | 94 | 17.2 |
| 501–1,500 | 133 | 24.3 |
| 1,501–2,500 | 119 | 21.8 |
| 2,501–3,500 | 80 | 14.6 |
| ≥3,501 | 121 | 22.1 |
| Family size | ||
| <5 | 448 | 81.9 |
| 5–7 | 79 | 14.4 |
| ≥8 | 20 | 3.7 |
| Variables | Frequency | Percent |
|---|---|---|
| Living condition | ||
| Alone | 89 | 16.3 |
| Live with my families (like wife, mother, father, sister, brother) | 437 | 79.9 |
| Others* | 21 | 3.8 |
| Lost job due to HIV | ||
| Yes | 153 | 28.0 |
| No | 394 | 72.0 |
| Opportunistic disease | ||
| Do not have | 469 | 85.7 |
| Toxoplasma | 17 | 3.1 |
| Fungus | 21 | 3.8 |
| Tuberculosis | 40 | 7.3 |
| BMI category | ||
| <18.5 | 112 | 20.5 |
| 18.5–24.99 | 390 | 71.3 |
| 25–29.99 | 45 | 8.2 |
| Source of infection | ||
| Blood contact | 97 | 17.7 |
| Unsafesexual intercourse | 213 | 38.9 |
| I do not know | 237 | 43.3 |
| Comorbidity | ||
| No | 482 | 88.1 |
| Diabetes mellitus | 26 | 4.8 |
| Hypertension | 39 | 7.1 |
| Substance use | ||
| Khat | 87 | 15.9 |
| Alcohol | 135 | 24.7 |
| Cigarettes | 40 | 7.3 |
| I do not use | 285 | 52.1 |
| Social support | ||
| Poor social support | 375 | 68.6 |
| Good social support | 172 | 31.4 |
| Depression status | ||
| Depressed | 376 | 68.7 |
| Non depressed | 171 | 31.3 |
| WHO clinical stage | ||
| Stage I | 434 | 79.3 |
| Stage II | 68 | 12.4 |
| Stage III | 45 | 8.2 |
| CD4 count current | ||
| <200 | 59 | 10.8 |
| 200–349 | 131 | 23.9 |
| 350–499 | 176 | 32.2 |
| ≥500 | 181 | 33.1 |
| Adherence to medication | ||
| Poor adherent | 442 | 80.8 |
| Good adherent | 105 | 19.2 |
| Drug side effect | ||
| Yes | 151 | 27.6 |
| No | 396 | 72.4 |
| Drug regimen | ||
| First line | 441 | 80.6 |
| Second line | 106 | 19.4 |
| Duration on HAART (in month) | ||
| 12 | 16 | 2.9 |
| 13-24 | 28 | 5.1 |
| ≥25 | 503 | 92.0 |
| Variables | Category | Stigma | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|---|
| No | Yes | ||||
| Sex | Male | 81 | 193 | 1 | 1 |
| Female | 94 | 179 | 0.79 (0.55, 1.15) | 0.71 (0.46, 1.1) | |
| Age | 18–29 | 33 | 84 | 1 | 1 |
| 30–39 | 58 | 130 | 0.88 (0.52,1.46) | 0.93 (0.52, 1.65) | |
| 40–49 | 61 | 109 | 0.70 (0.42,1.17) | 0.66 (0.36, 1.20) | |
| ≥50 | 23 | 49 | 0.44 (0.44, 1.58) | 0.83 (0.39, 1.77) | |
| Marital status | Single | 21 | 46 | 1 | 1 |
| Married | 10 | 236 | 1.03 (0.58, 1.82) | 1.2 (0.62, 2.25) | |
| Widowed | 30 | 43 | 0.65 (0.32, 1.31) | 0.77 (0.33, 1.78) | |
| Divorced | 20 | 47 | 1.07 (0.51, 2.23) | 1.4 (0.60,3.25) | |
| Substance use | Khat | 30 | 57 | 0.89 (0.53, 1.4) | 0.76 (0.42, 1.35) |
| Alcohol | 40 | 95 | 1.1 (0.71,1.73) | 0.94 (0.57, 1.55) | |
| Cigarette | 14 | 26 | 0.87 (0.43,1.74) | 0.83 (0.37,1.84) | |
| Do not use | 91 | 194 | 1 | 1 | |
| HIV stages | Stage I | 125 | 309 | 1.8 (0.96,3.38) | 1.78 (0.88, 3.58) |
| Stage II | 31 | 37 | 0.87 (0.40,1.86) | 0.89 (0.39, 2.04) | |
| Stage III | 19 | 26 | 1 | 1 | |
| CD4 counts | <200 | 18 | 41 | 1.24 (0.66, 2.34) | 1.1 (0.54, 2.05) |
| 200–349 | 37 | 94 | 1.38 (0.85, 2.26) | 1.4 (0.83, 2.43) | |
| 350–499 | 56 | 120 | 1.17 (0.75, 1.8) | 1.2 (0.75, 1.93) | |
| ≥500 | 64 | 117 | 1 | 1 | |
| BMI (kg/m2) | <18.5 | 27 | 85 | 5 (2.46, 10.89)* | 5 (2.30, 11.0)* |
| 18.5–24.99 | 120 | 270 | 3.7 (1.95, 7.01)* | 3.6 (1.88, 7.16)* | |
| >25 | 28 | 17 | 1 | 1 | |
| Level of depression | Depressed | 130 | 246 | 1 | 1 |
| Non-depressed | 45 | 16 | 1.4 (0.99, 2.21) | 1.5 (0.96, 2.35) | |
| Social support | Poor social support | 109 | 266 | 1.5 (1.03, 2.22)* | 1.5 (1.05, 2.40)* |
| Good social support | 66 | 106 | 1 |
| |
| HAART adherence | Adherent | 147 | 295 | 1 |
|
| Non-adherent | 28 | 77 | 1.3 (0.85, 2.2) | 1.7 (1.03, 3.05)* | |
| Mean (SD) | Stigma | BMICAT | Depression | |
|---|---|---|---|---|
| Stigma | 30.07 (9.4) | – | ||
| BMI | 20.98 (2.78) | -0.196*** | – | |
| Depression | 9.24 (7.13) | 0.518*** | -0.24*** | – |
| Effect size | SE | Boot LLCI | Boot ULCI |
| |
|---|---|---|---|---|---|
| Direct effect | -0.30 | 0.129 | -0.554513 | -0.045527 | 0.021 |
| Indirect effect | -0.41 | 0.076 | -0.557186 | -0.261132 | 0.000 |
| Total effect | -0.71 | 0.108 | -0.827837 | -0.403956 | 0.000 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV-related health complications and treatments · Adolescent Sexual and Reproductive Health
Introduction
HIV/AIDS is a major public health concern across the world, particularly in low- and middle-income countries (LMICs) (1). More than 74.9 million people worldwide have been infected with HIV (2). Sub-Saharan Africa (SSA), the most affected region, is home to 76% PLWHIV (3). HIV/AIDS-related stigma is seen as prejudice, discounting, ridiculing, and discrimination aimed against those who are suspected of having HIV/AIDS (4, 5).
Perceived stigma describes how people living with HIV (PLWHIV) feel or fear when they are being treated unfavorably (6, 7). The United Nations Programme on HIV/AIDS (UNAIDS) report indicated that over 50% of people globally experience discriminatory attitudes because of their HIV status (8). A study conducted in the United States reported that 89% of PLWHA in the US experienced perceived stigma (9). A study conducted in Botswana and Venezuela reported stigma as a major obstacle to HIV testing (10, 11). The perceived stigma has a significant impact on the quality of life in PLWHIV (12). Stigma limits PLWHIV’s access to care, which is a significant contributor to the global HIV pandemic (12–14).
Different studies conducted in Brazil (15), USA (16), South Africa (17), Zambia (18), and Southern Ethiopia (19) indicated an association between perceived HIV-related stigma and low birth weight. Other studies also revealed that a low BMI significantly increases the risk of developing antiretroviral drug-related liver injury (20) and tuberculosis (21) among people living with HIV patients. The findings from various studies highlight the importance of addressing perceived HIV-related stigma to improve the health outcomes for PWH, particularly in those with low BMI (22).
The national prevalence rate of HIV/AIDS in Ethiopia is 0.9% (23), and the number of PLWHA per region contributes to the varied prevalence rates (24). The Ethiopian Demographic and Health Survey (DHS) 2016 reported a low prevalence of HIV/AIDS (0.7%) in Oromia region (24) within and across nations. The low HIV prevalence may contribute to increased stigma toward PLWHA (25, 26).
In Ethiopia, about 16%–56% of PLWHA reported having perceived HIV-related stigma (27, 28). A stigma index survey done by networks of HIV-positive people in Ethiopia indicated that stigma is acquired and perpetuated through gossip, verbal insult, isolation, and rejection (6).
A recent systematic review indicated that an evidence-based effective programming to reduce stigmatizing and discriminatory attitudes has increased significantly (6, 29). However, money countries has not made reducing stigma a top priority in their national AIDS policies or programs (30), and HIV-related stigma continues to play a significant role in contributing to the spread of the epidemic (31). Although a substantial number of PLWHA live within the study area, the issue of HIV-related stigma has not been well addressed.
Therefore, this study primarily aimed at exploring BMI and its related mechanisms, which are essential to developing mental health interventions, which are becoming increasingly important to improve the mental and physical quality of life among HIV/AIDS patients. However, to the best of our knowledge, no studies have explored how and when BMI affects perceived HIV-related stigma in PLWHIV. Thus, this study also helps to determine whether depression mediates the association between BMI and perceived HIV-related stigma.
Methods
Study design and setting
A hospital-based cross-sectional study design was used to assess HIV-related perceived stigma and its associated factors among PLWHIV who receive treatment at antiretroviral therapy (ART) clinics. The Bale Zone is located approximately 412 kilometer (km) away from Addis Ababa. It has three government hospitals, one referral (Goba Referral Hospital), and two general hospitals (Dellomena and Robe General Hospitals) that are currently providing ART services in the Zone. During the period between February 1 and April 30, 2021, there were 3,308 adult HIV/AIDS patients who had registered for ART follow-up in these three public hospitals in the study hospitals.
Study population
All HIV-positive patients aged >18 years who were enrolled to receive ART treatment follow-up in public hospitals in Bale Zone were the source population (32). The potential participants were randomly selected for inclusion in the study if they had been enrolled for ART for at least 6 months. Patients who were unable to communicate or had a serious medical condition were excluded.
Sample size determination and sampling technique
The sample size was determined using the single population proportion formula using EPI info version 7.2 assuming the following parameters: 95% level of confidence, 4% marginal error, and 49.4% proportion of HIV-related perceived stigma among PLWHA (4). Moreover, 10% of the potential participants were added to address the non-response rate yielding the total sample size as 559. The study participants were chosen using systematic sampling techniques. The sampling interval was calculated by dividing the total number of patients on ART (N = 3 308) by the total desired sample size of 559. As a result, the k number was six, and the fourth patient was chosen at random from the first six ART patients, and then every sixth patient was included in the study. The sample size was allocated proportionally to each hospital after obtaining lists of potential participants from the ART registers of each hospital.
Variables of the study
Dependent variable
The dependent variable is perceived HIV-related stigma.
Independent variables
The socio-demographic variables included (age, sex, religion, residence, marital status, education level, occupation, and monthly income). The psychosocial variables included living condition, social support, and lost job. Clinically related data were included such as WHO HIV/AIDS stage, current CD4 count, medication adherence, drug regimen, current drug side effect, duration of HAART treatment, and viral load.
Data collection, measurement, procedures, and quality control
A data collection tool (questionnaire) that included socio-demographic, psychosocial, and disease-related information was developed after reviewing relevant literatures. The questionnaire was originally developed in the English language and translated into Amharic and local language (Afaan Oromo) by language experts. The Amharic and Afaan Oromo version was translated back to English to verify the consistency by language experts. Both of the Amharic and the Afaan Oromo language questionnaires were used to collect data.
HIV-related perceived stigma occurs when PLWHA feel/perceive or believe that they are being negatively treated by others including partners, family, friends, healthcare providers, and members of their community because of their HIV status (6). Perceived stigma was assessed using the HIV-related stigma scale assessment tool which contains 10 stigma assessment questions with Likert scale. The agreement questions (strongly disagree–strongly agree) were assigned values 1–5 in order to determine the level of perceived stigma. Respondents who scored higher than the mean from the total were considered to have experienced perceived stigma, whereas those who scored lower than the mean were considered to have not experienced perceived stigma (33, 34).
Additionally, social support was assessed using the Social Support Questionnaire-6 (SSQ-6) which assessed the available social support (35). It had six assessment questions (help from no one, help from family, friends, organization, regions father/person, and unknown persons); those respondents who scored higher than the mean were considered to have good social support, while those who scored lower than the mean were considered to have poor social support. Thirdly, the structured Patient Health Questionnaires-9 (PHQ-9) was used to measure the depression status of HIV/AIDS patients (36). It had a potential total sum score of 27 from nine items; those respondents who scored 5 and above in the total sum were considered depressed, while those scoring below 5 were considered non-depressed. Fourthly, the adherence was assessed using the Morisky Medication adherence scale questions eight (MMAS-8) that had a total sum score of 8 from eight items (37, 38). Respondents who scored below six were considered non-adherent, while those who scored six and above were considered adherent.
Data were collected using interviewer-administered questionnaires and by extracting pertinent information from the patients’ medical records. Four data collectors with bachelor of science (BSc) degrees prepared; nurses, midwifes, and public health were involved in data collection. A one-day intensive training was given on the objective of the study, how to fill the questionnaire, confidentiality of the information, and interviewing technique prior to their involvement for data collection. A pretesting of the questionnaire was done on 5% of the total sample size in a non-study area, and appropriate amendments were made before the actual data collection. The completed questionnaires were reviewed and checked for completeness, consistency, and relevance daily.
Data processing and analysis
The data were entered into Epi Data™ version 3.1 before being exported to Statistical Package for Social Science (SPSS ™) version 25 for cleaning, coding, and analysis. Descriptive statistics such as frequency, percentage, and mean were computed and presented by using text, tables, and graphs. Bivariable binary logistic regression was undertaken to see the association between dependent and independent variables. Those variables having a p-value of <0.25 in bivariable binary logistic regression were included in the multivariable logistic regression model. Both crude odds ratio (COR) and adjusted odds ratio along with 95% confidence interval (CI) were used to estimate the strength of the association between factors and outcome variable. In the multivariable logistic regression model, variables having a P-value of <0.05 were considered statistically significant. The Hosmer and Lemeshow test was used to determine the final model’s fitness, and the variance inflation factor was used to check for multi-collinearity among selected independent variables. We also used a mediation model in which body mass index served as the independent variable and perceived HIV-related stigma served as the dependent variable. In the model, depression was used as a mediating variable. Based on 5,000 bootstrap samples, the chain-mediating effect was estimated using the bootstrap 95% confidence interval (CI). All covariates were taken into account in the analysis.
Results
Socio-demographic and economic characteristics of study participants
A total of 547 study participants were included in the study, yielding an overall response rate of 97.8%. The respondents’ mean age (+SD) was 38.1 (± 9.8) years. A total of 274 (50.1%) respondents were male, 340 (62.2%) were married, and 200 (36.6%) were between the ages of 29 and 39 years. Almost one-third, 164 (30.0%), of the respondents attended primary education, 240 (43.9%) were Orthodox religion followers, 126 (23.0%) were housewives, and 402 (73.5%) lived in urban areas (Table 1). This study also identifies a negative association between body mass index and perceived HIV-related stigma in PLWHIV.
Psychosocial and clinical-related characteristics of respondents
Of the 547 study participants, 437 (79.9%) lived with their families, 153 (28%) lost their jobs due to HIV/AIDS-related illness, and 375 (68.6%) received inadequate social support from their families or other supportive bodies. Most of the respondents, 434 (79.3%), were at WHO clinical stage I, whereas 12.4% were at WHO clinical stage II. About one-third [181(33.1%)] of the respondents had a CD4 count greater than 500 cells/μL. More than two-thirds of 442 (80.8%) respondents had good adherence to HAART. Of all the study participants, 151 (27.6%) had HAART-related side effects, 441 (80.6%) were on the first line of the drug, and 503 (92%) were on HAART for more than or equal to 2 months (Table 2).
Table 2: Psychosocial and clinical characteristics of people living with HIV/AIDS in public hospitals in Southeast Ethiopia, 2021 ( n = 547).
Prevalence of perceived HIV-related stigma
The prevalence of perceived HIV-related stigma among people living AIDS was found to be 68% [95% CI: (64.1%, 71.9%)] (Figure 1).
Prevalence of perceived HIV-related stigma among people living with HIV/AIDS at hospitals in Southeast Ethiopia.
Factors associated with HIV-related perceived stigma
The multivariable binary logistic regression analysis result showed that having a BMI <18.5 kg/m^2^ [AOR = 5, 95% CI: (2.3, 11.0)], BMI 18.5–24.99 kg/m^2^ [AOR = 3.6, 5, 95%: (1.88, 7.16), poor social support [AOR = 1.5, 95% CI: (1.05, 2.40)], and non-adherent to HAART [AOR=1.7, 95% CI: (1.03, 3.05)] were significantly associated with perceived HIV-related stigma (Table 3).
Correlation analysis of BMI, stigma, and depression
Table 4 shows Pearson partial correlations among key variables after controlling for all covariates. All key variables were significantly associated. BMI was negatively associated with stigma (r = -0.196, P < 0.001). Stigma was positively associated with depression (r = 0.518, P < 0.001).,
Mediating roles of depression
Table 5 shows the mediating roles of depression in the association between body mass index and perceived HIV-related stigma.
Discussion
Internationally, it has been acknowledged that stigma kills more people than the HIV virus itself (39). The study attempted to ascertain the prevalence of HIV-related perceived stigma and associated factors among HIV patients attending an anti-retroviral treatment follow-up clinic at public hospitals of Southeast Ethiopia. The finding showed that the prevalence of HIV-related perceived stigma was high (68%) among the participants. Variables like BMI <18.5 kg/m^2^, BMI 18.5–24.99 kg/m^2^, poor social support, and non-adherence to HAART were significantly associated with perceived HIV-related stigma.
This study revealed that the prevalence of perceived stigma was higher compared to studies conducted in the hospitals of Oromia and Dessie city health facilities in Ethiopia (28, 40) and Cameron (13); however, it was lower than studies conducted at Jimma in Ethiopia (6), Iran (12), and University of Washington (41). This discrepancy might be explained by time variation and differences in setting, particularly for research conducted outside of Ethiopia. It might also be attributed to various governmental and non-governmental efforts in the respective sites.
In the current study, PLWHIV with a BMI of less than 18.5kg/m^2^ (underweight) were five times more likely to have perceived HIV-related stigma as compared to their counterparts. In the past, being underweight was used as a diagnostic criterion for HIV infection (42); hence, PLWHIV might be worrying about their body weight because as they become thinner or lose bodyweight they feel or fear discrimination.
In this study, social support was significantly associated with the level of perceived HIV-related stigma. Study participants with poor social support were 1.5 times more likely than their counter-parts to experience perceived stigma. However, there is evidence that social care and support should be provided in accordance with suitable social and ethical procedures rather than having PLWHIV being perceived as a distinct individual from the rest of the community sponsored by NGOs, which may result in significant stigma (6). Further investigation is needed to ameliorate this issue.
Despite this, the provision of ART was observed to increase the lifespan of people living with HIV/ADIS. Discrimination and a high burden of HIV/AIDS-related stigma, which is induced by socio-demographic, psychological, behavioral, and clinical variables, jeopardize this longer lifetime (43). This study also revealed that respondents who were non-adherent to HAART were 1.7 times more likely to have perceived HIV-related stigma. This could be due to stigma and discrimination, fear of being found, lack of social support, and poor health outcomes that may all play a role in emotional non-adjustment to HIV/AIDS, depression, and a loss of motivation in treatment; this would ultimately lead to poor treatment adherence among PLWHIV (44).
This study revealed a negative association between body mass index and perceived HIV-related stigma in PLWHIV (Figure 2). More importantly, the findings of this study suggest important roles for psychological status (depression) in the reduction of perceived HIV-related stigma in PLWHIV by body mass index. According to current studies, PLWHIV with a low body mass index (<18.5 kg/m^2^) (42) experience more severe perceived HIV-related stigma because of higher depression.
Specific path of the associations between body mass index and perceived HIV-related stigma (mediating effect).
This study suggests that body mass index affects perceived HIV-related stigma in PLWHIV with high depression (45), which adds numerical evidence to how body mass index affects perceived HIV-related stigma. PLWHIV who have a normal body mass index (18.5–24.9 kg/m^2^) might not worry about their body weight, and they are not feeling or fearing discrimination. These all contribute to a reduction in depression and thus a reduced risk of perceived HIV-related stigma. Thus, the study indicates that depression can be considered a potential psychological mechanism underlying the relationship between body mass index and perceived HIV-related stigma. Future researchers better explore other variables’ roles in this association.
Limitation of the study
In a study area lacking previous data on the prevalence and risk factors associated with HIV/AIDS, the aim of this study was to investigate the role of BMI on perceived HIV-related stigma. The following limitations must be taken into consideration when interpreting the study’s results, even though it employed primary data on the extent of perceived HIV-related stigma, depression, and social support with skilled data collectors and supervisors: First, a cause-and-effect relationship between the risk factors and perceived HIV-related stigma cannot be established due to the cross-sectional nature of the study. Second, self-reported surveys of social support, depression, and perceived stigma were used to evaluate the participants; however, these surveys may be liable to social desirability bias. Thirdly, because the study is centered in a hospital, the finding may not be generalizable to the total population.
Conclusion
This study showed that perceived HIV-related stigma was higher among people living with HIV/AIDS attending hospitals in Southeast Ethiopia due to low awareness of the impact of stigma. It is evident that PLWHIV can be stigmatized in a variety of ways, impacting treatment adherence and the mental health of patients living with HIV (46). As such, in order to address HIV management issues, in general, the impact of HIV-related stigma must be addressed with the same effort as vaccine trials and treatment development initiatives. The authors suggest that in all ART clinics, non-payment of services and free therapy should include education to increase awareness on the impact of stigma. The impact of HIV-related stigma including delayed testing, non-disclosure of HIV status, service access barriers, reduced treatment adherence, poor social support, and directly to the mental health among affected individuals and their families are detrimental to global efforts against HIV so far. In addition to addressing stigma in Ethiopia, the clinics should continue the promotion of HAART adherence to sustain people who are already affected by HIV. Our findings suggest that there is a relationship between body mass index and perceived HIV-related stigma, while depression can indirectly predict perceived HIV-related stigma. Importantly, the lessons learned from the findings of the current study need to be considered in the design and implementation of HIV initiatives, including policy making and programming in Ethiopia and related settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shao Y Williamson C. The HIV-1 epidemic: low- to middle-income countries. Cold Spring Harbor Perspect Med. (2012) 2:a 007187. doi: 10.1101/cshperspect.a 007187, PMID: 22393534 PMC 3282497 · doi ↗ · pubmed ↗
- 2WHO. HIV/AIDS. Australia: World health Organization (2020).
- 3WHO. key fact on HIV/AIDS. Australia: World health Organization (2021).
- 4Bedaso A Belagavi D Bekele G Mekonnen N. Factors Associated with Anxiety Disorder among ART Clients attending Antiretroviral Therapy Clinic. Ethiopia. (2016).
- 5Getalem A Emnet A. Prevalence and associated factors of depression among HIV patients taking antiretroviral therapy at Zewditu Memorial Hospital, Addis Ababa, Ethopia. J Sci Res Stud. (2016) 3:81–6.
- 6Fido NN Aman M Brihnu Z. HIV stigma and associated factors among antiretroviral treatment clients in Jimma town, Southwest Ethiopia. Hiv/aids (Auckland NZ). (2016) 8:183., PMID: 27920581 10.2147/HIV.S 114177 PMC 5126004 · doi ↗ · pubmed ↗
- 7Mohite VR Mohite RV George J. Correlates of perceived stigma and depression among the women with HIV/AIDS infection. Bangladesh J Med Science. (2015) 14:151–8. doi: 10.3329/bjms.v 14i 2.21864 · doi ↗
- 8Stover J Bollinger L Izazola JA Loures L De Lay P Ghys PD. What is required to end the AIDS epidemic as a public health threat by 2030? The cost and impact of the fast-track approach. Plo S One. (2016) 11:e 0154893. doi: 10.1371/journal.pone.0154893, PMID: 27159260 PMC 4861332 · doi ↗ · pubmed ↗