Epidural haematoma following vertebroplasty for osteoporosis compression fracture: A case report
Yongsheng Ye, Fangyue Deng, Yonghong Feng, Linfeng Luo, Henian Li, Shabin Zhuang

TL;DR
A 67-year-old woman developed an epidural haematoma after a vertebroplasty procedure for an osteoporotic fracture, highlighting the rare but serious risks of the treatment.
Contribution
This case report emphasizes the risk of epidural haematoma following vertebroplasty and the importance of preoperative imaging to prevent complications.
Findings
Epidural haematoma occurred after vertebroplasty due to puncture of the epidural venous plexus.
Preoperative CT and MRI analysis can help reduce the risk of such complications.
Urgent surgical decompression improved neurological symptoms in the patient.
Abstract
Percutaneous vertebroplasty (PVP) is a minimally invasive procedure commonly used to alleviate pain and stabilise vertebral compression fractures caused by osteoporosis. Although generally safe, the procedure carries the risk of rare complications, such as epidural haematomas. We present the case of a 67-year-old woman who underwent PVP for an abnormal pedicle structure associated with an osteoporotic compression fracture that led to the subsequently development of an epidural haematoma. The patient presented with severe back pain following a fall at home. Imaging revealed a T12 vertebral compression fracture with marked collapse and posterior wall involvement. The pain and functional impairment persisted despite conservative management. After polymethylmethacrylate injection into the fractured vertebrae, the patient reported unbearable lower back pain and bilateral lower limb…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
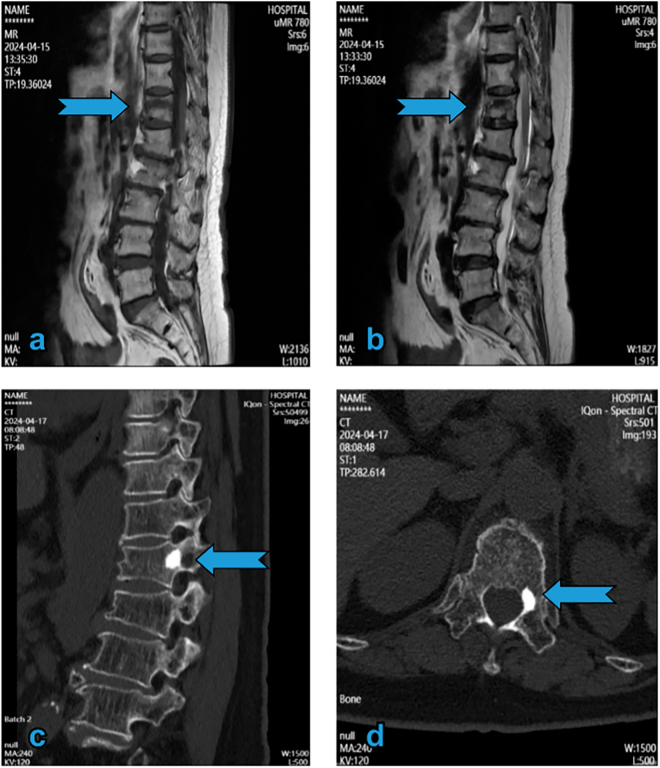 Figure 1
Figure 1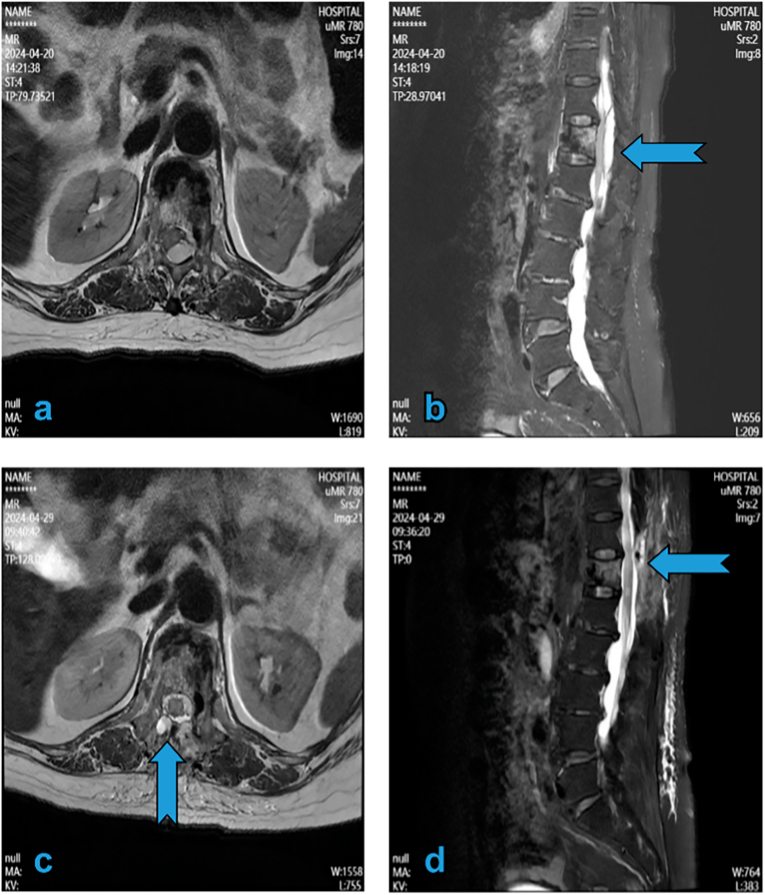 Figure 2
Figure 2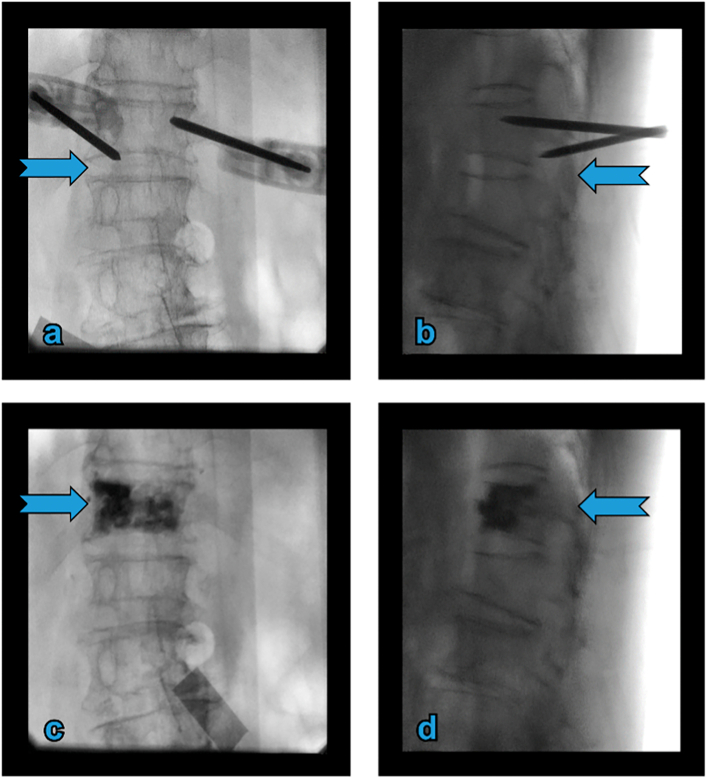 Figure 3
Figure 3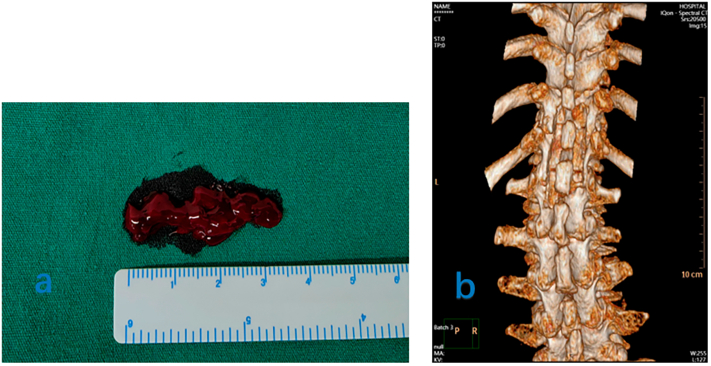 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Fractures and Fixation Techniques · Spinal Hematomas and Complications · Spine and Intervertebral Disc Pathology
Introduction
1
Percutaneous vertebroplasty (PVP) is a widely used procedure for managing painful osteoporotic vertebral compression fractures (OVCF), which can provide significant pain relief and improve function. However, PVP is associated with potential complications, including infection, neurological injury, bowel or bladder dysfunction, bleeding, rib fracture, cement leakage, adjacent vertebral fracture, and death due to pulmonary embolism [[1], [2], [3]]. Acute spinal epidural haematoma (SEH) is a rare but potentially severe complication that warrants attention in clinical practice. Herein, we report a case of pedicle structure abnormality that developed into SEH following PVP. This case has been reported in line with the SCARE criteria [1].
Presentation of case
2
A 67-year-old woman presented to our clinic with severe back pain after a fall at home. Imaging revealed a T12 vertebral compression fracture with significant collapse and posterior wall involvement (Fig. 1a, b). Pain and functional impairment persisted despite conservative management. Therefore, she was deemed eligible for PVP, which was conducted by a board-certified spinal surgeon in the hospital's main operating room. Polymethylmethacrylate was injected into the fractured vertebrae under fluoroscopic guidance. No cement leaked into the spinal canal (Fig. 3c, d).Fig. 1MRI of T1 and T2 sequences and preoperative CT. (a and b) Revealing vertebral compression fracture with hypointensity in T1 and hyperintensity in T2 (arrow). Preoperative CT (c) showing sclerosis lesions in the inner wall of the left pedicle in T12 (arrow). MRI: magnetic resonance imaging; CT: computed tomography.Fig. 1
Postoperatively, the patient exhibited improved mobility and no neurological deficits; nonetheless, she continued to have severe lower back pain. Approximately 1 h postoperatively, the patient complained of cold lower limbs. Skin examination revealed stable normal findings on palpation, and the dorsalis pedis artery had a normal pulse. She subsequently developed bilateral lower limb weakness. The neurological condition worsened, and she developed paraplegia. Magnetic resonance imaging (MRI) of the spine revealed bilateral SEH at T11–T12 that caused spinal cord compression (Fig. 2a, b).Fig. 2T2 vertebra MRI scan. (a and b) Hyper-acute epidural hematoma over T11 extending to the L1 vertebrae. Axial images showing epidural hematoma compressing the spinal cord (arrow). (c and d) MRI after hemilaminectomy decompression and hematoma removal showing resolution of both SEH and nerve compression (arrow). MRI: magnetic resonance imaging; SEH: spinal epidural haematoma.Fig. 2
Urgent surgical decompression was performed given the neurological deterioration and spinal cord compression due to SEH. Decompression was achieved via laminectomy without requiring supplemental spinal instrumentation (Fig. 4a, b). Intraoperatively, clotted blood was observed in the epidural space, exerting pressure on the spinal cord. After decompression, MRI revealed that SEH had been eliminated, and that the nerve was no longer compressed (Fig. 2c, d). Neurological symptoms improved gradually. Two weeks postoperatively, lower limb strength returned to grade IV, and skin sensation was normalised.
Discussion
3
PVP and percutaneous kyphoplasty (PKP) are well-established treatments for OVCF to alleviate pain and improve quality of life [2,5]. However, these procedures can cause complications, including pedicular fractures, nerve root injuries, and spinal cord lesions [3,4]. Spinal subdural haematoma (SSDH) and SEH are rare complications that usually occur a few hours after completion of PVP or PKP [6,7]. SSDHs can occur in the lower thoracic region, typically affecting two to five segments [7]. SSDHs are typically located anterior to the spinal cord, whereas SEHs are usually located posterior to the spinal cord [8]. To the best of our knowledge, a few SSDH cases following PVP have been reported, whereas SEH following PVP has been reported less frequently [6,7,[9], [10], [11], [12], [13], [14]].
SEHs can be classified as idiopathic, iatrogenic, traumatic, or coagulopathic. The analysis of over 1000 cases of SEH revealed that iatrogenic causes, such as coagulopathy or spinal puncture, accounted for 18 % of cases, while non-iatrogenic causes, such as genetic or metabolic coagulopathy, trauma, and pregnancy, comprised 29 %. The aetiology was multifactorial in 11.1 % of cases [15].
The aetiology of SEH is unclear however, it might include surgical iatrogenic factors, venous congestion, comorbidities, and anticoagulant therapy. Various iatrogenic causes might lead to SEH, including vascular injury during needle insertion, venous congestion caused by bone cement extravasation, and rupture of the epidural venous plexus. Cosar et al [11] suggested that spinal SEH can develop following a puncture of the spinal dura mater, allowing venous blood to infiltrate the subdural space post-trauma. Wang et al. emphasized that SEH after PKP resulted from damaged blood vessels caused by intraoperative puncture, which occurs when the rupture of the inner wall of the pedicle causes extravasation of blood within the cancellous bone, leading to blood flow into the epidural space [14].
Another potential cause of SEH is venous congestion due to bone cement leakage, which can increase pressure in the paravertebral veins, including the radiculomedullary veins, leading to SSDH and rupture of the epidural venous plexus [16].
Patients with underlying diseases, such as hypertension, coagulopathy, and thrombocytopenia, have an increased risk of bleeding. Hypertension before surgery can lead to spontaneous SEH [10]. Vascular malformation is also considered one of the causes of spontaneous SEH.
The pre- or postoperative use of anticoagulants might affect coagulation function and increase the risk of haematoma formation. Brelie et al. reported that SEH after PVP was due to coagulopathy induced by the long-term use of oral aspirin [17]. Zou reported that, in the absence of intraspinal cement leakage, the combination of pedicle puncture and the use of anticoagulants might cause SEH after PKP [14].
Our patient had normal haemostatic parameters (preoperative international normalised ratio, 1.0; platelet count, 200 × 10^9^/L), received no anticoagulants treatment, and normal baseline health metrics (blood pressure, 120/75 mm Hg; HbA1c, 5.2 %). We analysed the pathogenesis of the present case based on previous hypotheses. Direct puncture injury to the spinal cord during surgery was not likely as the patient had intact sensory and motor functions in the lower limbs after surgery. However, examination of the intraoperative puncture revealed that the left pedicle area was blocked by sclerosis (Fig. 1c, d), which prevented the puncture needle from entering the vertebrae via the transpedicular approach. The puncture needle inadvertently entered the nerve root exit area during needle adjustment, causing vessel injury (Fig. 3a, b).Fig. 3. Intraoperative fluoroscopy. (a and b) The left puncture needle accidentally penetrating the intervertebral foramen. (c and d) Anteroposterior view of the lumbar radiograph showing no evident intraspinal cement leakage.Fig. 3. Fig. 4Intraoperative imaging and postoperative CT findings. (a) Clotted blood is removed from the epidural space intraoperatively. (b) CT showing the extent of lamina decompression postoperatively. CT: computed tomography.Fig. 4
In our patient, the haematoma was located in the epidural space. The loose connective tissue in this space allows blood extravasation. The anterior and posterior spaces can be affected. The anterior space is located between the posterior part of the vertebral body and the dura mater, whereas the posterior space is located between the lamina and the dura mater. Bone cement leakage or damage to the posterior wall of the vertebral body can occur in the anterior space, resulting in bleeding. In the posterior space, the puncture needle can injure the epidural venous plexus or muscle vessels.
Preoperative computed tomography and other imaging data should be evaluated to identify physiological or structural abnormalities and to plan surgery. If an abnormal pedicle structure or puncture path is detected preoperatively, alternative puncture paths, such as those via the costovertebral joint or a unilateral transpedicular approach, should be considered. These alternatives decrease the risk of pedicle fracture, medial transgression of the pedicle, transgression into the spinal canal, nerve injury, cement extravasation along the cannula tract, and SEH [18].
Preventing SEH after PVP requires a continuous effort throughout the perioperative period. Improving coagulation and adjusting basic conditions before the operation are essential. For this purpose, three measures are recommended. The first includes assessing coagulation function. Preoperative tests are routinely performed to quantify four coagulation indicators and platelet count. The international normalised ratio should be ≤1.5, platelet count ≥100 × 10^9^/L, and anticoagulant drugs such as aspirin and warfarin should be discontinued before the operation. The second measure includes controlling underlying diseases, such as hypertension. Before the operation, blood pressure should be maintained below 140/90 mm Hg to reduce the risk of bleeding during puncture. The third measure includes conducting preoperative CT and MRI scans to assess the integrity of the posterior vertebral wall and the condition of the bone cortex and to predict injury to blood vessels during puncture.
Management includes emergency surgical decompression and conservative treatment. In patients with spinal cord compression (such as ASIA grade ≤ C) and progressive neurological dysfunction, laminectomy is performed for decompression and hematoma removal, whereas in patients with spinal cord compression (ASIA grade D) conservative treatment is selected.
Conclusion
4
Although PVP is considered safe and effective for managing compression fractures, clinicians should remain vigilant for potentially severe complications, such as SEH. Prompt recognition and early surgical intervention are crucial for optimising patient outcomes. Further studies are necessary to identify risk factors and develop preventive strategies for PVP.
CRediT authorship contribution statement
Y.S.Y. and F.Y.D. drafted the manuscript. Y.H.F. and H.N.L. designed the study. L.F.L. collected data. S.B.Z. performed all surgical procedures. All authors read and approved the final manuscript.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Ethical approval
This study was approved by the Ethics Committee of our institution, and written informed consent was obtained from the patient.
Guarantor
Shabin Zhuang.
Research registration number
Not applicable.
Funding
This study was supported by the Administration of Traditional Chinese Medicine of Guangdong Province (Grant No. 20251420), the Famous Traditional Chinese Medicine Studio of Dongguan Hospital of Traditional Chinese Medicine (Grant No.50202505002), and the Dongguan Social Development Science and Technology Project (Grant No. 20221800906042).
Declaration of competing interest
The authors declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kerwan A.Al-Jabir A.Mathew G.Sohrabi C.Rashid R.Franchi T.Nicola M.Agha M.Agha R.A.Revised surgical C Ase R Eport (SCARE) guideline: an update for the age of artificial intelligence Premier Journal of Science 102025100079
- 2Wang H.Sribastav S.S.Ye F.Yang C.Wang J.Liu H.Comparison of percutaneous vertebroplasty and balloon kyphoplasty for the treatment of single level vertebral compression fractures: a meta-analysis of the literature Pain Physician 18201520922226000665 · pubmed ↗
- 3Noguchi T.Yamashita K.Kamei R.Maehara J.Current status and challenges of percutaneous vertebroplasty (PVP)Jpn. J. Radiol.4120231133594368710.1007/s 11604-022-01322-w PMC 9813159 · doi ↗ · pubmed ↗
- 4Long Y.Yi W.Yang D.Advances in vertebral augmentation systems for osteoporotic vertebral compression fractures Pain Res. Manag.20202020394736810.1155/2020/3947368 PMC 773879833376566 · doi ↗ · pubmed ↗
- 5Wang W.Liu Y.Wan H.Zeng L.Peng Z.Yang D.Effectiveness and prognostic factors of different minimally invasive surgeries for vertebral compression fractures BMC Musculoskelet. Disord.242023113660929310.1186/s 12891-022-06125-8PMC 9817397 · doi ↗ · pubmed ↗
- 6Kang M.S.Shin Y.H.Lee C.D.Lee S.H.Delayed neurological deficits induced by an epidural hematoma associated with a thoracic osteoporotic compression fracture Neurol. Med. Chir. (Tokyo)5220126336362300687410.2176/nmc.52.633 · doi ↗ · pubmed ↗
- 7Wang X.Peng Y.Qiu J.Huang D.Spinal subdural and epidural hematomas after vertebroplasty for compression fracture: a case report Spinal Cord Ser. Cases 420188710.1038/s 41394-018-0120-5PMC 615504130275979 · doi ↗ · pubmed ↗
- 8Payer M.Agosti R.Spontaneous acute spinal subdural hematoma: spontaneous recovery from severe paraparesis—case report and review Acta Neurochir.1522010198119842070074810.1007/s 00701-010-0758-7 · doi ↗ · pubmed ↗