Assessment of Primary Malignancy Risk after Initiation of Biologic Therapy in Patients with Psoriasis
Chunghwan Ro, Ana Ormaza Vera, Waleed Adawi, Alexander Yap, Clinton W. Enos

TL;DR
This study found that biologic therapies for psoriasis are generally safe in terms of cancer risk over 10 years.
Contribution
The study provides new long-term oncologic safety evidence for IL-17 and IL-23 inhibitors in psoriasis treatment.
Findings
TNF inhibitors reduced the risk of any primary malignancy compared to biologic-naïve patients.
Biologic therapies did not increase the risk of melanoma or lymphoid/hematopoietic malignancies.
Nonmelanoma skin cancer risk was lower with TNF inhibitors but not with other biologic classes.
Abstract
Limited evidence exists regarding the long-term oncologic safety of biologic therapies, particularly IL-17 inhibitors and IL-23 inhibitors, in the management of psoriasis. This propensity score–matched retrospective cohort study assessed the risk of developing a primary malignancy within 10 years after exposure to a Food and Drug Administration–approved biologic among patients with psoriasis compared with that among biologic-naïve controls. After propensity score matching, 32,230 biologic-exposed patients were further grouped into cohorts of TNF inhibitors (n = 16,011), IL-23 inhibitors (n = 5604), IL-12/23 inhibitors (n =3856), and IL-17 inhibitors (n = 5467). During a 10-year period, TNF inhibitor–treated patients had a reduced risk of developing any primary malignancy compared with biologic-naïve patients with psoriasis (hazard ratio [HR] = 0.80; 95% confidence interval [CI] =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
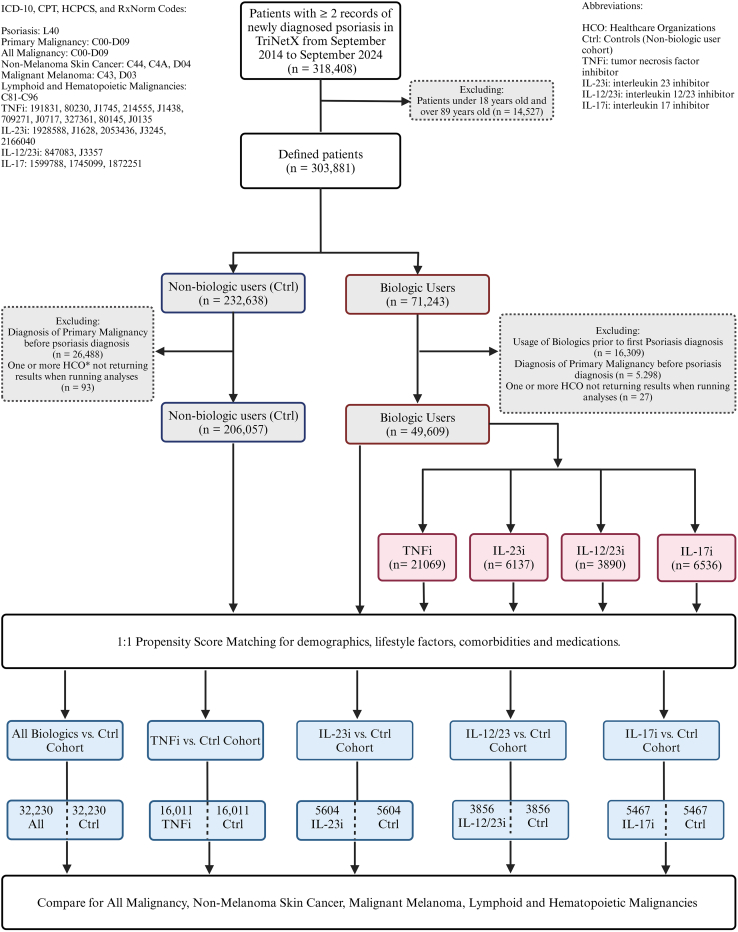 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsoriasis: Treatment and Pathogenesis
Introduction
Psoriasis has been associated with an elevated risk of certain malignancies relative to the general population (Trafford et al, 2019; Vaengebjerg et al, 2020), a link often attributed to chronic systemic inflammation, immune dysregulation, and lifestyle factors such as smoking and alcohol use (Boehncke and Schön, 2015). Although biologic therapies have revolutionized psoriasis management by significantly improving disease outcomes through targeted immunomodulation (Armstrong and Read, 2020), concerns remain regarding their long-term oncologic safety owing to their immunomodulatory effects (Briukhovetska et al, 2021). As a result, patients may experience apprehension initiating or continuing biologics owing to concerns about the potential long-term risk of malignancy (Lebwohl et al, 2016). Previous studies examining this association have yielded mixed results (Vaengebjerg et al, 2020), and there is limited evidence regarding the long-term oncologic safety profiles of newer biologic agents such as IL-17 inhibitor (IL-17i) and IL-23 inhibitor (IL-23i).
In this study, we conducted a propensity score–matched retrospective cohort analysis comparing patients with psoriasis with biologic exposure with biologic-naïve patients. Cohorts included patients with up to 10 years of follow-up, allowing for the assessment of both early- and late-onset malignancies. By encompassing a diverse group of biologic agents and extending the observation period, we aimed to provide a more comprehensive evaluation of the incidence and risk of primary malignancy associated with biologic treatments for psoriasis.
Results
Before propensity score matching, 49,609 patients with psoriasis received biologic therapy, whereas 206,057 did not (Table 1). In the crude analysis, there was an observed decreased risk for primary malignancy risk in each biologic-class cohort (TNF-α inhibitor [TNFi], IL-17 inhibitor [IL-17i], IL-12/23 inhibitor [IL-12/23i], or IL-23 inhibitors [IL-23i]) compared with that in biologic-naïve controls (risk for all malignancy: TNFi hazard ratio [HR] = 0.69, 95% confidence interval [CI] = 0.65–0.73; IL-23i HR = 0.81, 95% CI = 0.71–0.93; IL-12/23i HR = 0.73, 95% CI = 0.64–0.84; IL-17i HR = 0.74, 95% CI = 0.66–0.83) (Table 2). After propensity score matching, a total of 32,230 biologic-treated patients with psoriasis were included in the analysis (Table 1). These were further categorized into 16,011 patients receiving only TNFi; 5604 initiating IL-23i exclusively; 3856 initiating IL-12/23i exclusively; and 5467 initiating IL-17i exclusively. Each treatment group was 1:1 propensity score matched to a biologic-naïve control cohort (Table 3, Table 4, Table 5, Table 6). The maximum duration of treatment was 9.96 years for TNFi, 9.26 years for IL-17i, 9.98 years for IL-12/23i, and 6.4 years for IL-23i (Table 7).Table 1. Baseline Characteristics of Patients with Psoriasis with and without Biologic TherapiesCharacteristicCrudeStd diff.AdjustedStd diff.Psoriasis, Biologic (n = 49,609)Psoriasis, No Biologic (n = 206,057)Psoriasis, Biologic (n = 30,938)Psoriasis, No Biologic (n = 30,938)Age at index, y, mean (SD)48.1 (15)51 (16.6)0.1947.7 (15.4)48 (16)0.02Gender, n (%) Male21,394 (43.1)84,612 (41.1)0.0413,675 (44.2)14,163 (45.8)0.03 Female26,023 (52.5)108,403 (52.6)0.0015,946 (51.5)15,720 (50.8)0.01 Unknown gender2192 (4.4)13,042 (6.3)0.081317 (4.3)1055 (3.4)0.04Race, n (%) American Indian or Alaska Native247 (0.5)687 (0.3)0.03153 (0.5)130 (0.4)0.01 Asian1830 (3.7)10,354 (5.0)0.071203 (3.9)1150 (3.7)0.01 Black or African American2418 (4.9)10,376 (5.1)0.011750 (5.6)1625 (5.3)0.02 Native Hawaiian or Other Pacific Islander131 (0.3)803 (0.4)0.0285 (0.3)80 (0.3)0.00 Other race1750 (3.5)6303 (3.1)0.031154 (3.7)1086 (3.5)0.01 Unknown race6435 (12.9)33,234 (16.1)0.094138 (13.4)3770 (12.2)0.04 White36,798 (74.2)144,300 (70.0)0.0922,455 (72.6)23,097 (74.6)0.05Ethnicity, n (%) Hispanic or Latino3054 (6.2)12,367 (6.0)0.012007 (6.5)1928 (6.2)0.01 Not Hispanic or Latino34,701 (69.9)138,770 (67.3)0.0621,369 (69.1)21,497 (69.5)0.01 Unknown ethnicity11,854 (23.9)54,920 (26.7)0.067561 (24.4)7512 (24.3)0.00Diagnosis, n (%) Arthropathic psoriasis (L40.5)20,488 (41.3)5801 (2.8)1.054771 (15.4)5203 (16.8)0.04 Essential (primary) hypertension (I10)14,434 (29.1)56,503 (27.4)0.048587 (27.8)8505 (27.5)0.01 Overweight and obesity (E66)10,292 (20.7)30,613 (14.9)0.155862 (18.9)5913 (19.1)0.00 Nicotine dependence (F17.2)5857 (11.8)19,140 (9.3)0.083583 (11.6)3453 (11.2)0.01 Noninfective enteritis and colitis (K50–52)4339 (8.7)12,741 (6.2)0.102628 (8.5)2655 (8.6)0.00 Alcohol related disorders (F10)1899 (3.8)5926 (2.9)0.051197 (3.9)1115 (3.6)0.01 Unspecified viral hepatitis C (B19.2)469 (0.9)1581 (0.8)0.02293 (0.9)290 (0.9)0.00 HIV disease (B20)143 (0.3)880 (0.4)0.0292 (0.3)89 (0.3)0.00 Unspecified viral hepatitis B (B19.1)146 (0.3)449 (0.2)0.0285 (0.3)71 (0.2)0.01 Tuberculosis (A15–19)152 (0.3)289 (0.1)0.0481 (0.3)58 (0.2)0.02 Exposure to tanning bed (W89.1)15 (0.0)16 (0.0)0.0212 (0.0)10 (0.0)0.00Medication, n (%) Methotrexate11,206 (22.6)6820 (3.3)0.604024 (13.0)4047 (13.1)0.00 Apremilast4920 (9.9)1201 (0.6)0.431144 (3.7)1141 (3.7)0.00 Cyclosporine1315 (2.6)1476 (0.7)0.15689 (2.2)667 (2.2)0.00 Azathioprine463 (0.9)888 (0.4)0.06246 (0.8)253 (0.8)0.00 Mycophenolate mofetil230 (0.5)838 (0.4)0.01161 (0.5)145 (0.5)0.01Abbreviation: Std diff., Standardized mean difference.Table 2. Crude Incidence and Risk of Primary Malignancy after Initiation of a Biologic in Patients with Psoriasis at 10 yearsDrug ClassOutcomesIncidencesHazard Ratio (95% CI)RiskDifference %P-ValueBiologicNonbiologicTNFin = 21,619n = 206,057All malignancy1109117,0940.69 (0.65–0.73)−3.64%<.001NMSC239261280.74 (0.67–0.82)−1.16%<.001MM35310920.56 (0.43–0.73)−0.29%<.001Lymphoid and hematopoietic49818690.60 (0.50–0.74)−0.45%<.001IL-23in = 6137n = 206,057All malignancy119317,0940.81 (0.71–0.93)−5.54%.002NMSC26361280.82 (0.65–1.03)−1.94%.09MM31110920.71 (0.39–1.29)−0.35%.26Lymphoid and hematopoietic42218691.12 (0.60–2.09)−0.55%.49IL-12/23in = 3890n = 206,057All malignancy120717,0940.73 (0.64–0.84)−3.37%<.001NMSC29161280.96 (0.78–1.17)−0.64%.66MM31610920.93 (0.57–1.53)−0.12%.78Lymphoid and hematopoietic41918690.64 (0.41–1.00)−0.42%.05IL-17in = 6536n = 206,057All malignancy126117 0940.74 (0.66–0.83)−4.69%<.001NMSC29461280.81 (0.66–0.98)−1.53%.03MM31810920.90 (0.58–1.40)−0.25%.63Lymphoid and hematopoietic44618691.26 (0.95–1.67)−0.20%.10Abbreviations: CI, confidence interval; ICD-10, International Classification of Diseases, Tenth Revision; IL-17i, IL-17 inhibitor; IL-12/23i, IL-12/23 inhibitor; IL-23i, IL-23 inhibitor; MM, malignant melanoma; NMSC, nonmelanoma skin cancer; TNFi, TNF inhibitor.1ICD-10: C00-D09.2NMSC ICD-10: C44, C4A, and D04.3MM ICD-10: C43 and D03.4ICD-10: C81–C96.Table 3. Baseline Characteristics of Patients with Psoriasis on TNFi and without Biologic TherapiesCharacteristicCrudeStd diff.AdjustedStd diff.TNFi (n = 21,619)Nonbiologic (n = 206,057)TNFi (n = 16,011)Nonbiologic (n = 16,011)Age at index, y, mean (SD)48.3 (15.3)51 (16.6)0.1548.7 (15.5)49.1 (16.2)0.03Gender, n (%) Male9426 (43.6)84,612 (41.1)0.057029 (43.9)7403 (46.2)0.05 Female11,349 (52.5)108,403 (52.6)0.018350 (52.1)8151 (50.9)0.02 Unknown gender844 (3.9)13,042 (6.3)0.09632 (4.0)456 (2.9)0.06Race, n (%) American Indian or Alaska Native130 (0.6)687 (0.3)0.0490 (0.6)88 (0.6)0.00 Asian631 (2.9)10,354 (5.0)0.12540 (3.4)573 (3.6)0.01 Black or African American1116 (5.2)10,376 (5.1)0.01898 (5.6)877 (5.5)0.01 Native Hawaiian or Other Pacific Islander55 (0.3)803 (0.4)0.1048 (0.3)40 (0.3)0.01 Other race847 (3.9)6303 (3.1)0.02634 (4.0)596 (3.7)0.01 Unknown race2503 (11.6)33,234 (16.1)0.101928 (12.0)1692 (10.6)0.05 White16,337 (75.6)144,300 (70.0)0.1411,872 (74.2)12,144 (75.9)0.04Ethnicity, n (%) Hispanic or Latino1621 (7.5)12,367 (6.0)0.031207 (7.5)1206 (7.5)0.00 Not Hispanic or Latino15,078 (69.7)138,770 (67.3)0.0411,072 (69.1)11,297 (70.6)0.03 Unknown ethnicity4920 (22.8)54,920 (26.7)0.063732 (23.3)3508 (21.9)0.03Diagnosis, n (%) Arthropathic psoriasis (L40.5)10,878 (50.3)5801 (2.8)1.255256 (32.8)5298 (33.1)0.01 Essential (primary) hypertension (I10)6188 (28.6)56,503 (27.4)0.024504 (28.1)4590 (28.7)0.01 Overweight and obesity (E66)4314 (20.0)30,613 (14.9)0.122904 (18.1)2882 (18.0)0.00 Nicotine dependence (F17.2)2425 (11.2)19 140 (9.3)0.061676 (10.5)1752 (10.9)0.02 Noninfective enteritis and colitis (K50–52)2021 (9.3)12 741 (6.2)0.111401 (8.8)1511 (9.4)0.02 Alcohol related disorders (F10)846 (3.9)5926 (2.9)0.05612 (3.8)612 (3.8)0.00 Unspecified viral hepatitis C (B19.2)216 (1.0)1581 (0.8)0.03157 (1.0)155 (1.0)0.00 HIV disease (B20)57 (0.3)880 (0.4)0.0042 (0.3)48 (0.3)0.01 Unspecified viral hepatitis B (B19.1)64 (0.3)449 (0.2)0.0351 (0.3)51 (0.3)0.00 Tuberculosis (A15–19)57 (0.3)289 (0.1)0.0237 (0.2)37 (0.2)0.00 Exposure to tanning bed (W89.1)10 (0.0)16 (0.0)0.0210 (0.1)10 (0.1)0.00Medication, n (%) Methotrexate5526 (25.6)6820 (3.3)0.662416 (15.1)3032 (18.9)0.10 Apremilast1503 (7.0)1201 (0.6)0.32663 (4.1)738 (4.6)0.02 Cyclosporine423 (2.0)1476 (0.7)0.09291 (1.8)328 (2.0)0.02 Azathioprine90 (0.4)888 (0.4)0.0070 (0.4)90 (0.6)0.02 Mycophenolate mofetil208 (1.0)838 (0.4)0.06144 (0.9)144 (0.9)0.00Abbreviations: Std diff., Standardized mean difference; TNFi, TNF inhibitor.Table 4. Baseline Characteristics of Patients with Psoriasis on IL-23i and without Biologic TherapiesCharacteristicCrudeStd diff.AdjustedStd diff.IL-23i (n = 6137)Nonbiologic (n = 206,057)IL-23i (n = 5604)Nonbiologic (n = 5604)Age at index, y, mean (SD)49.0 (15.3)51 (16.6)0.1148.8 (15.4)49.2 (15.8)0.03Gender, n (%) Male2828 (46.1)84,612 (41.1)0.102592 (46.3)2629 (46.9)0.01 Female3131 (51.0)108,403 (52.6)0.042853 (50.9)2854 (50.9)0.00 Unknown G=gender178 (2.9)13,042 (6.3)0.14159 (2.8)121 (2.2)0.04Race, n (%) American Indian or Alaska Native22 (0.4)687 (0.3)0.0019 (0.3)10 (0.2)0.03 Asian292 (4.8)10,354 (5.0)0.03264 (4.7)237 (4.2)0.02 Black or African American347 (5.7)10,376 (5.1)0.02316 (5.6)345 (6.2)0.02 Native Hawaiian or Other Pacific Islander21 (0.3)803 (0.4)0.0918 (0.3)13 (0.2)0.02 Other race274 (4.5)6303 (3.1)0.05261 (4.7)227 (4.1)0.03 Unknown race722 (11.8)33,234 (16.1)0.09665 (11.9)592 (10.6)0.04 White4459 (72.7)144,300 (70.0)0.064061 (72.5)4180 (74.6)0.05Ethnicity, n (%) Hispanic or Latino342 (5.6)12,367 (6.0)0.05313 (5.6)252 (4.5)0.05 Not Hispanic or Latino4357 (71.0)138,770 (67.3)0.063952 (70.5)4055 (72.4)0.04 Unknown ethnicity1438 (23.4)54 920 (26.7)0.041339 (23.9)1297 (23.1)0.02Diagnosis, n (%) Arthropathic psoriasis (L40.5)1145 (18.7)5801 (2.8)0.50769 (13.7)679 (12.1)0.05 Essential (primary) hypertension (I10)1985 (32.3)56,503 (27.4)0.101747 (31.2)1751 (31.2)0.00 Overweight and obesity (E66)1594 (26.0)30,613 (14.9)0.251399 (25.0)1351 (24.1)0.02 Nicotine dependence (F17.2)881 (14.4)19,140 (9.3)0.15760 (13.6)727 (13.0)0.02 Noninfective enteritis and colitis (K50–52)533 (8.7)12,741 (6.2)0.08475 (8.5)443 (7.9)0.02 Alcohol related disorders (F10)297 (4.8)5926 (2.9)0.09260 (4.6)236 (4.2)0.02 Unspecified viral hepatitis C (B19.2)49 (0.8)1581 (0.8)0.0045 (0.8)36 (0.6)0.02 HIV disease (B20)21 (0.3)880 (0.4)0.0217 (0.3)16 (0.3)0.00 Unspecified viral hepatitis B (B19.1)23 (0.4)449 (0.2)0.0120 (0.4)16 (0.3)0.01 Tuberculosis (A15–19)22 (0.4)289 (0.1)0.0414 (0.3)27 (0.5)0.04 Exposure to tanning bed (W89.1)10 (0.2)16 (0.0)0.0510 (0.2)10 (0.2)0.00Medication, n (%) Methotrexate686 (11.2)6820 (3.3)0.59533 (9.5)554 (9.9)0.01 Apremilast1022 (16.7)1201 (0.6)0.30653 (11.7)677 (12.1)0.01 Cyclosporine197 (3.2)1476 (0.7)0.17161 (2.9)155 (2.8)0.01 Azathioprine29 (0.5)888 (0.4)0.0026 (0.5)22 (0.4)0.01 Mycophenolate mofetil38 (0.6)838 (0.4)0.0332 (0.6)22 (0.4)0.03Abbreviations: IL-23i, IL-23 inhibitor; Std diff., Standardized mean difference.Table 5. Baseline Characteristics of Patients with Psoriasis on IL-12/23i and without Biologic TherapiesCharacteristicsCrudeStd diff.AdjustedStd diff.IL-12/23i (n = 3890)Nonbiologic (n = 206,057)IL-12/23i (n = 3856)Nonbiologic (n = 3856)Age at index, y, mean (SD)46.8 (16.5)51 (16.6)0.2446.9 (16.5)47.1 (16.6)0.02Gender, n (%) Male1767 (45.4)84,612 (41.1)0.091751 (45.4)1782 (46.2)0.02 Female2005 (51.5)108,403 (52.6)0.031986 (51.5)1981 (51.4)0.00 Unknown gender119 (3.1)13,042 (6.3)0.14119 (3.1)93 (2.4)0.04Race, n (%) American Indian or Alaska Native11 (0.3)687 (0.3)0.0210 (0.3)12 (0.3)0.01 Asian198 (5.1)10,354 (5.0)0.02197 (5.1)170 (4.4)0.03 Black or African American233 (6.0)10,376 (5.1)0.03232 (6.0)232 (6.0)0.00 Native Hawaiian or Other Pacific Islander11 (0.3)803 (0.4)0.1010 (0.3)10 (0.3)0.00 Other race173 (4.4)6303 (3.1)0.06170 (4.4)171 (4.4)0.00 Unknown race536 (13.8)33,234 (16.1)0.04531 (13.8)488 (12.7)0.03 White2735 (70.3)144,300 (70.0)0.022706 (70.1)2773 (71.9)0.04Ethnicity, n (%) Hispanic or Latino252 (6.5)138,770 (67.3)0.00249 (6.5)213 (5.5)0.04 Not Hispanic or Latino2621 (67.4)12,367 (6.0)0.012597 (67.3)2615 (67.8)0.01 Unknown ethnicity1017 (26.1)54,920 (26.7)0.011011 (26.2)1028 (26.7)0.01Diagnosis, n (%) Arthropathic psoriasis (L40.5)848 (21.8)5801 (2.8)0.58818 (21.2)805 (20.9)0.01 Essential (primary) hypertension (I10)1068 (27.5)56,503 (27.4)0.011053 (27.3)1049 (27.2)0.00 Overweight and obesity (E66)763 (19.6)30,613 (14.9)0.10754 (19.5)760 (19.7)0.00 Nicotine dependence (F17.2)569 (14.6)19,140 (9.3)0.27555 (14.4)606 (15.7)0.04 Noninfective enteritis and colitis (K50–52)426 (10.9)12,741 (6.2)0.05422 (11.0)415 (10.8)0.01 Alcohol related disorders (F10)149 (3.8)5926 (2.9)0.04146 (3.8)138 (3.6)0.01 Unspecified viral hepatitis C (B19.2)24 (0.6)1581 (0.8)0.0224 (0.6)24 (0.6)0.00 HIV disease (B20)14 (0.4)880 (0.4)0.0213 (0.3)20 (0.5)0.02 Unspecified viral hepatitis B (B19.1)18 (0.5)449 (0.2)0.0018 (0.5)25 (0.6)0.03 Tuberculosis (A15–19)11 (0.3)289 (0.1)0.0312 (0.3)10 (0.3)0.01 Exposure to tanning bed (W89.1)11 (0.3)16 (0.0)0.0710 (0.3)10 (0.3)0.00Medication, n (%) Methotrexate579 (14.9)6820 (3.3)0.41558 (14.5)628 (16.3)0.05 Apremilast368 (9.5)1201 (0.6)0.41340 (8.8)361 (9.4)0.02 Cyclosporine132 (3.4)1476 (0.7)0.18128 (3.3)145 (3.7)0.02 Azathioprine57 (1.5)888 (0.4)0.1155 (1.4)57 (1.5)0.00 Mycophenolate mofetil30 (0.8)838 (0.4)0.0530 (0.8)33 (0.9)0.01Abbreviations: IL-12/23i, IL-12/23 inhibitor; Std diff., Standardized mean difference.Table 6. Baseline Characteristics of Patients with Psoriasis on IL-17i and without Biologic TherapiesCharacteristicsCrudeStd diff.AdjustedStd diff.IL-17i (n = 6536)Nonbiologic (n = 206,057)IL-17i (n = 5467)Nonbiologic (n = 5467)Age at index, y, mean (SD)49.9 (14.3)51 (16.6)0.2149.9 (14.4)51.1 (15.4)0.08Gender, n (%) Male2847 (43.6%)84,612 (41.1%)0.052416 (44.2%)2493 (45.6%)0.03 Female3384 (51.8%)108,403 (52.6%)0.032811 (51.4%)2791 (51.1%)0.01 Unknown gender305 (4.6%)13,042 (6.3%)0.04240 (4.4%)183 (3.3%)0.05Race, n (%) American Indian or Alaska Native27 (0.4)687 (0.3)0.0123 (0.4)14 (0.3)0.03 Asian294 (4.5)10,354 (5.0)0.03257 (4.7)248 (4.5)0.01 Black or African American333 (5.1)10,376 (5.1)0.00288 (5.3)264 (4.8)0.02 Native Hawaiian or Other Pacific Islander19 (0.3)803 (0.4)0.0915 (0.3)11 (0.2)0.02 Other race276 (4.2)6303 (3.1)0.05220 (4.0)194 (3.5)0.02 Unknown Race988 (15.1)33,234 (16.1)0.03816 (14.9)723 (13.2)0.05 White4599 (70.4)144,300 (70.0)0.013848 (70.4)4013 (73.4)0.07Ethnicity, n (%) Hispanic or Latino417 (6.4)138,770 (67.3)0.01351 (6.4)305 (5.6)0.04 Not Hispanic or Latino4269 (65.3)12,367 (6.0)0.083606 (66.0)3713 (67.9)0.04 Unknown ethnicity1850 (28.3)54,920 (26.7)0.091510 (27.6)1449 (26.5)0.03Diagnosis, n (%) Arthropathic psoriasis (L40.5)2735 (41.8%)5801 (2.8%)1.041678 (30.7%)1641 (30.0%)0.01 Essential (primary) hypertension (I10)2164 (33.1%)56,503 (27.4%)0.111764 (32.3%)1837 (33.6%)0.03 Overweight and obesity (E66)1517 (23.2%)30,613 (14.9%)0.011200 (22.0%)1166 (21.3%)0.02 Nicotine dependence (F17.2)827 (12.7%)19,140 (9.3%)0.08651 (11.9%)599 (11.0%)0.03 Noninfective enteritis and colitis (K50–52)368 (5.6%)12,741 (6.2%)0.10298 (5.5%)284 (5.2%)0.01 Alcohol related disorders (F10)280 (4.3%)5926 (2.9%)0.05226 (4.1%)206 (3.8%)0.02 Unspecified viral hepatitis C (B19.2)51 (0.8%)1581 (0.8%)0.0245 (0.8%)42 (0.8%)0.01 HIV disease (B20)21 (0.3%)880 (0.4%)0.0215 (0.3%)10 (0.2%)0.02 Unspecified viral hepatitis B (B19.1)20 (0.3%)449 (0.2%)0.0116 (0.3%)22 (0.4%)0.02 Tuberculosis (A15–19)17 (0.3%)289 (0.1%)0.0313 (0.2%)17 (0.3%)0.01 Exposure to tanning bed (W89.1)10 (0.2%)16 (0.0%)0.0510 (0.2%)10 (0.2%)0.00Medication, n (%) Methotrexate1086 (16.6%)6820 (3.3%)0.45707 (12.9%)758 (13.9%)0.03 Apremilast1000 (15.3%)1201 (0.6%)0.56517 (9.5%)616 (11.3%)0.06 Cyclosporine206 (3.2%)1476 (0.7%)0.17144 (2.6%)161 (2.9%)0.02 Azathioprine38 (0.6%)888 (0.4%)0.0226 (0.5%)27 (0.5%)0.00 Mycophenolate mofetil48 (0.7%)838 (0.4%)0.0436 (0.7%)33 (0.6%)0.01Abbreviations: IL-17i, IL-17 inhibitor; Std diff., Standardized mean difference.Table 7. Time on Biologic Treatment for Patients with Psoriasis1DrugTime on Treatment, yMean (SD)MedianMaximumTNFi3.44 (2.58)2.959.96IL-23i1.60 (1.38)1.396.4IL-12/23i3.42 (2.50)2.989.98IL-17i2.45 (1.50)1.469.26Abbreviations: IL-17i, IL-17 inhibitor; IL-12/23i, IL-12/23 inhibitor; IL-23i, IL-23 inhibitor; TNFi, TNF inhibitor.1At baseline.
Within a 10-year observation window, TNFi-treated patients with psoriasis exhibited a reduced risk of any primary malignancy compared with the biologic-naïve controls (832 vs 1173, HR = 0.80, 95% CI= 0.73–0.87). Similar reduced risks were observed for NMSC (292 vs 392, HR = 0.82, 95% CI = 0.71–0.96). Although reduced incidences of malignant melanoma (41 vs 59, HR = 0.72, 95% CI = 0.49–1.06) and lymphoid or hematopoietic cancers (84 vs 126, HR = 0.78, 95% CI = 0.60–1.02) were observed, these did not reach statistical significance (Table 8).Table 8. Incidence and Risk of Primary Malignancy after Initiation of a Biologic in Patients with Psoriasis 10 Years after Propensity Score MatchingDrug ClassOutcomesIncidencesHazard Ratio (95% CI)RiskDifference %P-ValueBiologicNonbiologicTNFin = 16,011n = 16 011All malignancy183211730.80 (0.73–0.87)−2.31%<.001NMSC22923920.82 (0.71–0.96)−0.68%.01MM341590.72 (0.49–1.06)−0.12%.26Lymphoid and hematopoietic4841260.78 (0.60–1.02)−0.28%.06IL-23in = 5604n = 5604All malignancy11742090.83 (0.68–1.02)−0.63%.07NMSC260561.09 (0.77–1.55)0.07%.62MM310110.90 (0.38–2.12)−0.02%.81Lymphoid and hematopoietic421191.12 (0.60–2.09)0.04%.72IL-12/23in = 3856n = 3856All malignancy11992570.85 (0.71–1.03)−1.55%.09NMSC290841.22 (0.90–1.64)0.16%.21MM313180.80 (0.39–1.64)−0.13%.54Lymphoid and hematopoietic418290.70 (0.39–1.26)−0.30%.23IL-17in = 5467n = 5467All malignancy11892350.87 (0.73–1.04)−1.04%.12NMSC267571.03 (0.77–1.38)0.23%.85MM317200.91 (0.48–1.75)−0.07%.78Lymphoid and hematopoietic439261.56 (0.95–2.58)0.29%.08Abbreviations: CI, confidence interval; ICD-10, International Classification of Diseases, Tenth Revision; IL-17i, IL-17 inhibitor; IL-12/23i, IL-12/23 inhibitor; IL-23i, IL-23 inhibitor; MM, malignant melanoma; NMSC, nonmelanoma skin cancer; TNFi, TNF inhibitor.1ICD-10: C00-D09.2NMSC ICD-10: C44, C4A, and D04.3MM ICD-10: C43 and D03.4ICD-10: C81–C96.
Decreased incidence of developing any primary malignancy was observed for those treated with IL-23i (174 vs 209, HR = 0.83, 95% CI = 0.68–1.02), IL-12/23i (199 vs 257, HR = 0.85, 95% CI = 0.71–1.03), or IL-17i (189 vs 235, HR = 0.87, 95% CI = 0.73–1.04) compared with that for the biologic-naïve controls; however, CIs included the null. There was no significant difference in the risk of developing NMSC, malignant melanoma, and lymphoid or hematopoietic cancers compared with the controls over the same period for these cohorts (Table 8).
Discussion
In this retrospective cohort study, biologic therapies were not associated with an increased risk of primary malignancy in patients with psoriasis over a 10-year follow-up period. Notably, TNFi-treated patients with psoriasis showed a reduced risk of NMSC, diverging from prior findings (Asgari et al, 2017; Peleva et al, 2018), offering reassurance regarding their oncologic safety. The divergence between our findings and prior data may stem from differences in study populations, follow-up durations, and methodological approaches.
Recent evidence suggests that IL-17i and IL-23i do not confer an elevated malignancy risk compared with TNFi and with matched biologic-naïve patients (Kridin et al, 2024). Although this study has been instrumental in establishing confidence in the safety profiles of IL-17i and IL-23i, the shorter observation period may limit detection of potential late-emerging malignancies beyond 5 years. This analysis not only confirms prior findings (Kridin et al, 2024; Wu et al, 2023) but also reinforces the reassuring profile of these novel agents beyond 5 years through an extended follow-up period of up to 10 years.
Our data support the role of TNFi, IL-17i, IL-12/23i, and IL-23i in the long-term clinical management of psoriasis, offering greater reassurance to both clinicians and patients in decisions regarding sustained biologic therapy.
Limitations include differences in treatment availability and follow-up durations across biologic subclasses, which may have influenced the results. Potential inaccuracies in electronic medical records used to source data also may affect diagnostic precision and event reporting. In addition, matching on patient-level data alone may not fully address center-level confounding, and TriNetX’s open system might miss diagnoses or treatments occurring elsewhere. Consequently, data should be interpreted as purely observational without establishing a cause–effect relationship between biological therapies and the incidence of primary malignancies.
In conclusion, biologic therapies were not associated with an increased risk of primary malignancies in patients with psoriasis during a 10-year follow-up period; in fact, we often observe a decreased risk for malignancy. Notably, TNFi demonstrated a reduced risk of NMSC, challenging prior data and providing reassurance regarding its oncologic safety profile. Ultimately, the prescription of biologics should be approached thoughtfully and tailored to the individual needs of each patient.
Materials and Methods
This observational retrospective cohort study utilized deidentified data from the federated electronic health record TriNetX from 2014 to 2024. TriNetX is a global research platform that provides real-time access to data from a range of healthcare organizations, including hospitals, outpatient clinics, academic medical centers, and community hospitals. This study utilized data from the TriNetX Research Network, which encompasses more than 133 million individuals receiving care at 95 healthcare organizations located in multiple countries but primarily focused on the United States. The data included demographic information, diagnoses (documented according to ICD-10, Clinical Modification), procedures (recorded using either the ICD-10, Procedure Coding System; Current Procedural Terminology; or Healthcare Common Procedure Coding System), medications, and laboratory test results.
Patients aged 18–89 years with 2 separate psoriasis diagnosis who initiated a TNFi (adalimumab, etanercept, infliximab, certolizumab pegol), IL-17i (secukinumab, ixekizumab, brodalumab), IL-12/23i (ustekinumab), or IL-23i (guselkumab, Risankizumab, and tildrakizumab) between September 2014 and September 2024 were included. Individuals with a known history of malignancy prior to their first psoriasis diagnosis were excluded from analysis. The control cohort included patients with psoriasis with similar eligibility criteria without biologic exposure. To reduce the confounding impact of multiple therapeutic regimens, exclusion criteria ensured that individuals in any given treatment group had neither prior nor future exposure to any other biologic class. For example, participants in the IL-17i group could not have ever received IL-23i, IL-12/23i, or TNFi.
Of note, during the study period, International Classification of Diseases, Ninth Revision codes were utilized to identify patients and outcomes until the transition to ICD-10 coding in October 2015. TriNetX inherently addresses this coding transition by mapping International Classification of Diseases, Ninth Revision codes directly to their corresponding ICD-10 codes. Consequently, we included cases identified through International Classification of Diseases, Ninth Revision that seamlessly transitioned to ICD-10 within the analysis, ensuring the uniqueness of each patient case and eliminating any duplicate counting from patients diagnosed with both coding systems. The study design and relevant codes are depicted in Table 9 and Figure 1.Table 9ICD-10-CM Codes Utilized within TriNetXICD-10-CM CodesDescriptorL40PsoriasisC00-D09Malignant neoplasms and in situ neoplasmsF10Alcohol related disordersF17.2Nicotine dependenceW89.1Exposure to tanning bedE66Overweight and obesityL40.5Arthropathic psoriasisI10Essential (primary) hypertensionA15–19TuberculosisB20HIV diseaseB19.1Unspecified viral hepatitis BB19.2Unspecified viral hepatitis CK50–52Noninfective enteritis and colitisC44Other and unspecified malignant neoplasms of the skinC4AMerkel cell carcinomaD04Carcinoma in situ of the skinC43Malignant melanoma of the skinD03Melanoma in situC81–C96Malignant neoplasms of lymphoid, hematopoietic, and related tissuesAbbreviation: ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification.Figure 1Study design. Shown is a flowchart illustrating the study design and cohort construction from the TriNetX database, with cohorts defined using ICD-10, CPT, HCPCS, and RxNorm codes. CPT, Current Procedural Terminology; Ctrl, control; HCO, healthcare organization; HCPCS, Healthcare Common Procedure Coding System; ICD, International Classification of Diseases; IL-17i, IL-17 inhibitor; IL-12/23i, IL-12/23 inhibitor; IL-23i, IL-23 inhibitor; TNFi, TNF inhibitor.
To account for potential confounding factors, we implemented 1:1 propensity score matching to create cohorts with comparable baseline characteristics. Matching characteristics included demographics (age, sex, race, and ethnicity), lifestyle factors (alcohol-related disorders, nicotine dependence, and exposure to tanning beds), comorbidities (overweight and obesity, arthropathic psoriasis, primary hypertension, tuberculosis, HIV disease, unspecific viral hepatitis B, unspecific viral hepatitis C, and noninfective enteritis and colitis), and medication use (methotrexate, apremilast, cyclosporine, azathioprine, and mycophenolate mofetil) (Table 1). Race and ethnicity classifications were derived from patient electronic medical records, which contain either self-reported data or classifications observed by healthcare providers. The race category labeled "Other Race" included patients who identified with multiple races or with a racial group not listed in the predefined database options (American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, unknown race, and White). The "Unknown Race" category was used when race information was not available within patient records.
Propensity score matching ensured an even distribution of confounding variables across the study groups. Propensity score matching was performed through a 1:1 matching with a nearest-neighbor greedy algorithm and a caliper set at 0.25 times the SD.
Cohorts were followed up to 10 years. HRs and 95% CIs were calculated to assess the risk of primary malignancy after treatment with biologics. Primary malignancies were defined according to ICD-10-CM codes as follows: all malignancies (C00-D09), NMSCs (C44, C4A, and D04), malignant melanoma (C43 and D03), and lymphoid and hematopoietic malignancies (C81–C96).
All study variables were reported as means with SDs for continuous variables and as frequencies with corresponding percentages for dichotomous variables. Comparisons involving continuous variables were conducted using Student’s t-test, whereas Pearson’s chi-square test was applied for dichotomous variables. Survival analyses were performed using the Kaplan–Meier method, and a log-rank test was used to determine differences in malignancy risk between the groups. HRs were calculated through Cox regression, and Schoenfeld residuals analysis was employed to assess the proportional hazards assumption. Statistical significance was defined as a 2-tailed P < .05. All statistical analyses, including propensity score matching, were conducted within the built-in TriNetX Compare Outcomes Analytics function (TriNetX, 2025).
Ethics Statement
This study utilized deidentified patient data from TriNetX and is exempt from institutional review board approval.
Data Availability Statement
The data underlying this article are available within the main text. All data were retrieved from TriNetX, LLC, a platform ensuring compliance with the Health Insurance Portability and Accountability Act Security Rule for the protection of healthcare data. Because all patient data were deidentified, this study was deemed exempt for institutional review board review.
ORCIDs
Chunghwan Ro: http://orcid.org/0009-0000-3072-6732
Ana Ormaza Vera: http://orcid.org/0009-0004-4995-841X
Waleed Adawi: http://orcid.org/0000-0003-1242-7960
Alexander Yap: http://orcid.org/0000-0001-5695-9227
Clinton Enos: http://orcid.org/0000-0002-6783-1904
Conflict of Interest
CE has previously served as a consultant on an advisory board for UCB and Amgen, is an investigator for Amgen and Castle Biosciences, and has previously received research funding from La Roche-Posay and the ASA/Arcutis Biotherapeutics. The remaining authors state no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Armstrong A.W.Read C.Pathophysiology, clinical presentation, and treatment of psoriasis: a review JAMA 3232020194519603242730710.1001/jama.2020.4006 · doi ↗ · pubmed ↗
- 2Asgari M.M.Ray G.T.Geier J.L.Quesenberry C.P.Malignancy rates in a large cohort of patients with systemically treated psoriasis in a managed care population J Am Acad Dermatol 7620176326382816285410.1016/j.jaad.2016.10.006 · doi ↗ · pubmed ↗
- 3Boehncke W.H.Schön M.P.Psoriasis Lancet 38620159839942602558110.1016/S 0140-6736(14)61909-7 · doi ↗ · pubmed ↗
- 4Briukhovetska D.Dörr J.Endres S.Libby P.Dinarello C.A.Kobold S.Interleukins in cancer: from biology to therapy Nat Rev Cancer 2120214814993408378110.1038/s 41568-021-00363-z PMC 8173513 · doi ↗ · pubmed ↗
- 5Kridin K.Abdelghaffar M.Mruwat N.Ludwig R.J.Thaçi D.Are interleukin 17 and interleukin 23 inhibitors associated with malignancies?-Insights from an international population-based study J Eur Acad Dermatol Venereol 3820243153243773096210.1111/jdv.19520 · doi ↗ · pubmed ↗
- 6Lebwohl M.G.Kavanaugh A.Armstrong A.W.Van Voorhees A.S.US perspectives in the management of psoriasis and psoriatic arthritis: patient and physician results from the population-based multinational assessment of psoriasis and psoriatic arthritis (MAPP) survey Am J Clin Dermatol 17201687972671871210.1007/s 40257-015-0169-x PMC 4733141 · doi ↗ · pubmed ↗
- 7Peleva E.Exton L.S.Kelley K.Kleyn C.E.Mason K.J.Smith C.H.Risk of cancer in patients with psoriasis on biological therapies: a systematic review Br J Dermatol 17820181031132872216310.1111/bjd.15830 · doi ↗ · pubmed ↗
- 8Trafford A.M.Parisi R.Kontopantelis E.Griffiths C.E.M.Ashcroft D.M.Association of psoriasis with the risk of developing or dying of cancer: a systematic review and meta-analysis JAMA Dermatol 1552019139014033161786810.1001/jamadermatol.2019.3056 PMC 6802036 · doi ↗ · pubmed ↗