Interventional Treatment Is an Effective Approach to Relieve Symptoms in Patients With Malignant Tracheoesophageal Fistula
Pei Huang, Jinghua Cui, Zhenbang Lie, Jing Li

TL;DR
Interventional treatments for malignant tracheoesophageal fistulas in esophageal cancer patients improve symptoms and short-term survival.
Contribution
This study demonstrates that interventional treatments are more effective than traditional methods for managing malignant tracheoesophageal fistulas.
Findings
Patients receiving interventional treatments had significantly longer survival durations compared to traditional medical treatment.
Interventional treatments effectively relieved symptoms in patients with malignant tracheoesophageal fistulas.
Cox regression analysis identified treatment regimen as an independent predictive factor for increased survival.
Abstract
A malignant tracheoesophageal fistula (mTEF) is a complication of primary tumor growth or the recurrence of esophageal tumors or lung carcinoma. Patients with mTEF have lower survival and quality of life than those who do not develop this complication. Esophageal cancer (EC), a common gastrointestinal malignancy, ranks among the world's leading causes of cancer‐related death. The low survival rate in patients with EC is attributed to malnutrition, repeated aspiration, and severe infection; the mean survival duration is 2–4 months after diagnosis. This study investigated the clinical characteristics of patients with EC complicated with mTEF and the efficacy of various treatment regimens. This study was a retrospective analysis of the clinical data of 51 patients with EC complicated with mTEF hospitalized at Guangdong Provincial People's Hospital from February 2007 to May 2021. Patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
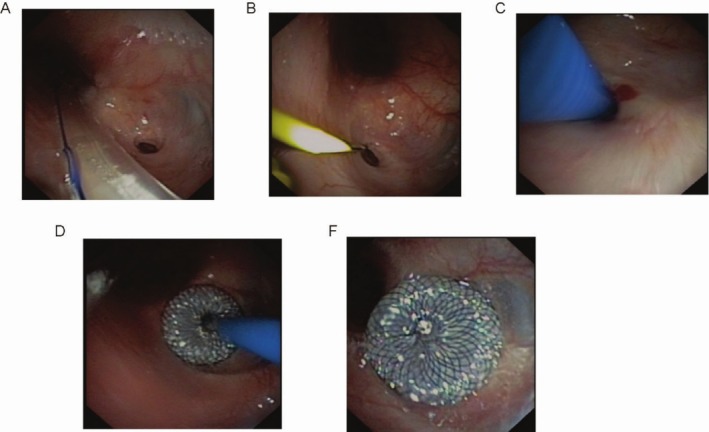 FIGURE 1
FIGURE 1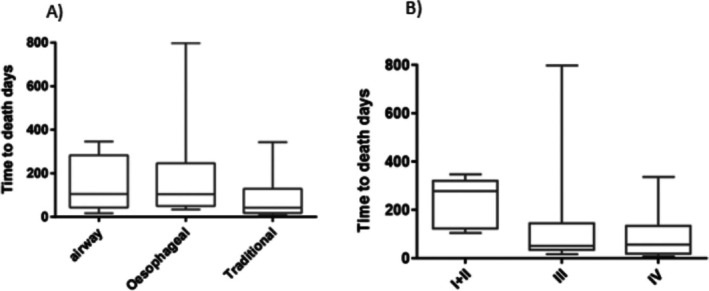 FIGURE 2
FIGURE 2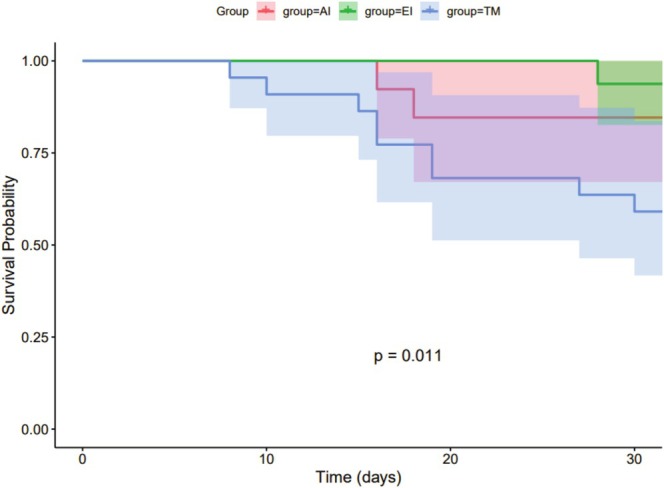 FIGURE 3
FIGURE 3 FIGURE 4
FIGURE 4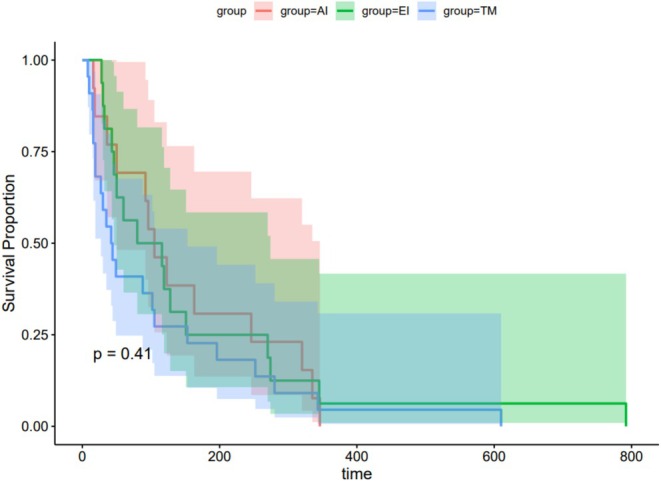 FIGURE 5
FIGURE 5| Variable | Patients, no. (%) | ||
|---|---|---|---|
| AI | EI | TM | |
| Sex | |||
| Male | 11 (21.6) | 15 (29.4) | 21 (41.1) |
| Female | 2 (3.9) | 1 (2.0) | 1 (2.0) |
| Age, years | |||
| ≥ 55 | 10 (19.6) | 10 (19.6) | 14 (27.5) |
| < 55 | 3 (5.9) | 6 (11.8) | 8 (15.7) |
| Fistula cause | |||
| Tumor invasion | 3 (5.9) | 9 (17.6) | 10 (19.6) |
| Radical surgery | 6 (11.8) | 1 (2.0) | 8 (15.7) |
| Radiotherapy | 3 (5.9) | 5 (9.8) | 4 (7.8) |
| Chemotherapy | 1 (2.0) | 1 (2.0) | 0 (2.0) |
| Fistula location in airway | |||
| Trachea | 10 (19.6) | 7 (13.7) | 18 (35.3) |
| Main bronchus | 3 (5.9) | 7 (13.7) | 3 (5.9) |
| Bronchus | 0 (0) | 2 (4.0) | 1 (2.0) |
| Initial tumor staging | |||
| I + II | 3 (5.9) | 1 (2.0) | 4 (7.8) |
| III | 5 (9.8) | 10 (19.6) | 13 (25.5) |
| IV | 5 (9.8) | 5 (9.8) | 5 (9.8) |
| Variable | ORR ( | NR ( |
|
|
|---|---|---|---|---|
| Sex | ||||
| Male | 28 | 18 | 0.706 | 0.639 |
| Female | 4 | 1 | ||
| Age | ||||
| ≥ 55 years | 22 | 11 | 0.615 | 0.547 |
| < 55 years | 10 | 8 | ||
| Fistula cause | ||||
| Tumor invasion | 12 | 10 | 1.570 | 0.666 |
| Radical surgery | 11 | 4 | ||
| Radiotherapy | 8 | 4 | ||
| Chemotherapy | 1 | 1 | ||
| Fistula location in airway | ||||
| Trachea | 24 | 11 | 5.569 | 0.062 |
| Main bronchus | 5 | 8 | ||
| Bronchus | 3 | 0 | ||
| Treatment group | ||||
| AI | 11a | 2a | 8.176 | 0.015 |
| EI | 12a,b | 4a,b | ||
| TM | 9b | 13b | ||
| Tumor stage | ||||
| I + II | 7 | 1 | 4.535 | 0.104 |
| III | 18 | 10 | ||
| IV | 7 | 8 | ||
| Variable |
| Mean survival | Median survival |
|
|---|---|---|---|---|
| Sex | ||||
| Male | 46 | 128.9 | 87.0 | 0.82 |
| Female | 5 | 143.0 | 150.0 | |
| Age | ||||
| ≥ 55 years | 33 | 131.5 | 91.5 | 0.65 |
| < 55 years | 18 | 145.3 | 76.0 | |
| Fistula cause | ||||
| Invasion of fistula | 22 | 95.1 | 76.0 | 0.074 |
| Radical of fistula | 15 | 230.2 | 222.5 | |
| Radiotherapy | 11 | 99.4 | 49 | |
| Chemotherapy | 3 | 32 | 32 | |
| Fistula location | ||||
| Trachea | 35 | 138.9 | 91.5 | 0.27 |
| Main bronchus | 13 | 88.4 | 49 | |
| Bronchus | 3 | 211 | 196 | |
| Treatment | ||||
| AI | 13 | 153.5 | 108.0 | 0.041 |
| EI | 16 | 166.1 | 104.0 | |
| TM | 22 | 88.1 | 42 | |
| Tumor stage | ||||
| I + II | 8 | 244.4 | 276.0 | 0.012 |
| III | 28 | 120.8 | 52.5 | |
| IV | 15 | 93.9 | 56 | |
| Total | 51 | 130.1 | 87.0 | |
| Variable | Low‐risk groups vs. high‐risk | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|---|
| Hazard ratio |
| 95% CI | Hazard ratio |
| 95% CI | ||
| Sex | Female vs. male | 2.537 | 0.201 | 0.609–10.567 | |||
| Age | ≥ 55 vs. < 55 years | 0.967 | 0.922 | 0.494–1.894 | |||
| Treatment | EI vs. TM | 0.604 | 0.222 | 0.269–1.357 | |||
| AI vs. TM | 0.669 | 0.288 | 0.319–1.404 | ||||
| Fistula cause | Radical of fistula vs. invasion of fistula | 0.288 | 0.008 | 0.114–0.726 | 0.328 | 0.018 | 0.130–0.829 |
| Radiotherapy vs. invasion of fistula | 0.871 | 0.733 | 0.395–1.923 | 0.838 | 0.663 | 0.379–1.852 | |
| Invasion of fistula vs. chemotherapy | 2.895 | 0.095 | 0.831–10.089 | 2.479 | 0.154 | 0.710–8.651 | |
| Fistula location | Main bronchus + bronchus vs. trachea | 0.861 | 0.663 | 0.440–1.686 | |||
| Tumor stage | I + II + III vs. IV | 0.152 | 0.010 | 0.036–0.634 | 0.182 | 0.020 | 0.043–0.766 |
- —the National Key Research and Development Program of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Esophageal Cancer Research and Treatment · Tracheal and airway disorders
Introduction
1
Malignant tumor‐related tracheoesophageal fistula (mTEF) is a pathological connection between the esophagus and airway due to primary tumor growth or the recurrence of esophageal or lung carcinoma [1, 2]. It can occur secondary to radiation or chemotherapy, resulting in tumor dehiscence, poor quality of life (QoL), and low survival. Approximately 70% of mTEF are associated with esophageal cancer (EC), 20% with lung cancer, and a small proportion with other tumors, such as malignant mediastinal lymph node lesions, thyroid cancer, and laryngeal cancer [3].
Approximately 10% of patients with EC develop mTEF, trapping them in a vicious cycle of choking during eating, repeated pulmonary infections, and cachexia [4]. In patients with EC complicated by mTEF, frequent airway aspiration, malnutrition, and severe infections can cause rapid deterioration. Their QoL scores are on average > 40% lower than those of tumor patients without fistulas, with a 1‐year survival rate < 15% and most surviving only 2–4 months after diagnosis [5, 6, 7]. There is an urgent need for more effective interventions to break through this therapeutic bottleneck.
Therapeutic strategies for mTEF have undergone continuous development, including surgical resection/fistula repair, medical supportive care, and interventional treatment. Surgery is the first‐line treatment for EC patients with mTEF, but it has limited efficacy. The reported surgical closure rate was only 1.9% (14/733) for a bronchial fistula occurring within 14 days after pneumonectomy; furthermore, most patients are not suitable candidates for surgery because of severe infection and poor general condition [8]. Traditional medical support care also has limited effects, and it provides no obvious relief from short‐term symptoms. By contrast, interventional treatment has emerged as a core development direction in mTEF treatment due to its minimally invasive nature, target specificity, and rapid symptom control. It enables enteral nutrition, direct fistula closure, and lower pulmonary infection risk, relieving symptoms quickly and reducing surgical needs. Guided by endoscopy or imaging, these techniques enable precise placement of fistula occluders and establishment of enteral nutrition pathways. Avoiding thoracotomy trauma, these techniques reduce pulmonary infection incidence by 60%–70% and relieve choking symptoms in > 90% of patients within 48 h postoperatively [9, 10]. More groundbreaking is the development of emerging biodegradable occlusive materials, which are rewriting the long‐term complication challenges of traditional metal stents and offering new pathways for biological fistula closure [11].
However, significant clinical evidence gaps exist in interventional treatment for EC with mTEF, including lacking standardized treatment selection guidelines, unclear long‐term survival impacts, and particularly undefined mechanisms on whether it can create opportunity windows for subsequent tumor chemoradiotherapy [12]. Through retrospective analysis, this study systematically compares the efficacy of esophageal stenting (EI), airway stenting (AI), and traditional therapy (TM) for the first time, aiming to establish evidence‐based personalized treatment strategies for mTEF and provide critical clinical evidence to address this “dead end in cancer treatment.”
Materials and Methods
2
Study Design and Ethics
2.1
This study is a single‐center retrospective study, which has been approved by the Research Ethics Committee of Guangdong Provincial People's Hospital (approval no. KY‐Q‐2022‐079‐01). Due to the retrospective nature of the study, the ethics committee waived the requirement for informed consent.
Patients
2.2
This study included patients hospitalized at Guangdong Provincial People's Hospital between February 2007 and May 2021, aged 20–80 years, with histologically confirmed EC and diagnosed with esophagotracheal fistula via upper gastrointestinal radiography, fibroesophagoscopy, bronchoscopy, or chest computed tomography. Patients were ineligible for surgery due to malnutrition, high disease severity, poor general condition, high surgical risk, or refusal of treatment. Additionally, patients who underwent open surgical repair, thoracoscopic intervention, or had unavailable survival data were excluded from this study.
Subsequently, the enrolled patients were divided into three groups according to the treatment received: traditional medical treatment (TM) group, esophageal interventional therapy (EI) group, and airway interventional therapy (AI) group. Patients in the TM group received noninvasive treatments such as anti‐infection therapy, thoracic drainage, intravenous nutritional support, nasogastric feeding, and gastrostomy. Patients with stent implantation were classified into esophageal stent group and airway stent group according to stent type. Patients in the EI group underwent covered esophageal stent implantation, while patients in the AI group received direct occlusion device implantation under fiberoptic bronchoscopy guidance, such as atrial septal occluders or airway stents.
For AI procedures, the selection of occlusion devices or stents was based on lesion characteristics: self‐expanding metallic stents (e.g., nitinol) were preferred for complex airway stenosis with elastic recoil, while silicone stents were used for benign strictures requiring easier removability. Modified atrial septal occluders were selected for tracheobronchial fistulas with defect diameters ≤ 15 mm, matched to fistula size via pre‐procedural imaging. For EI, covered esophageal stents were chosen based on lesion location (proximal/mid/distal esophagus) and severity. AI procedures were performed under general anesthesia with continuous vital sign monitoring, involving bronchoscopic visualization of airway lesions (e.g., stenosis or fistulas), followed by fluoroscopically guided deployment of airway stents or modified atrial septal occluders to restore patency or seal defects. EI involved conscious sedation or general anesthesia, fluoroscopic navigation for esophageal stent placement, with pre‐procedural endoscopic measurement of lesions and deployment of covered stents to prevent leakage, followed by post‐implantation assessment of patency and complications. The specific interventional procedure can be seen in Figure 1.
Interventional procedure. (A) A fistula is visualized via gastroscopy. (B) A guidewire is inserted via bronchoscopy. (C) Guidewire‐guided sheath insertion. (D) Release the occluder. (E) A fistula occluded by an occluder.
Data Acquisition
2.3
The baseline characteristics of the patients (age, sex, initial tumor staging, fistula location, fistula cause, and therapeutic effects) were recorded. Initial tumor staging refers to the tumor stage at the time of initial diagnosis. The causes of fistula formation include tumor invasion, residual tumor progression after radical surgery, and tumor regression during radiotherapy and chemotherapy. Currently, there is no standardized criterion for evaluating the treatment response of airway fistulas. Wang et al. established a standard evaluation to determine the efficacy of stent fistula closure according to experience from multiple centers in China [13]. Patients in complete remission (CR) exhibit a sealing of the fistula and complete relief of clinical symptoms (such as choking while drinking, fever, etc.) for one month; patients in clinical complete remission (cCR) have a sealed fistula that is completely occluded by stents along with complete relief of clinical symptoms for one month; patients in partial remission (PR) exhibit a fistula that is not closed and is partially occluded by a stent, along with partially relieved clinical symptoms; and patients not in remission (NR) are those in whom the fistula is not closed and not occluded by a stent, and the clinical symptoms are not relieved. The overall response rate (ORR) is the sum of CR, cCR, and PR. The treatment outcomes of this study were evaluated with reference to the above criteria. Tumor staging was determined according to the 8th edition of the American Joint Committee on Cancer Staging Manual [14].
Patient Follow‐Up
2.4
All patients were followed up through outpatient data, inpatient data, and telephone calls. Follow‐ups occurred 1 month after discharge to assess the therapeutic effects and every 2 months thereafter or as needed according to the patient's symptoms. The referring doctor conducted long‐term follow‐ups via telephone for patients who were unable to routinely visit our clinic.
Statistical Analysis
2.5
Data are presented as the mean ± standard deviation (for normally distributed continuous data), or the number (%) (for categorical data), or the median (interquartile range, IQR) (for non‐normally distributed continuous data). For comparisons of continuous data, the unpaired t‐test was used for normally distributed variables, while the Mann–Whitney U test was applied for non‐normally distributed variables. For categorical data, Pearson's chi‐square test was used when sample sizes were sufficient, and Fisher's exact test was employed for small sample sizes or sparse data. Survival data were analyzed using the Kaplan–Meier method with log‐rank tests for group comparisons, and the Cox proportional hazards regression model was used for multivariate analysis of survival factors. For chi‐square comparisons across three groups, post hoc pairwise comparisons were adjusted using the Bonferroni correction, with statistical significance set at a corrected threshold of p < 0.016 (0.05/3). For all other tests, statistical significance was defined as p < 0.05. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 20.0 (IBM Corporation, Armonk, NY, USA).
Results
3
Demographics
3.1
Of the 51 patients with EC complicated with mTEF, 46 were male and five were female; the mean age was 58.2 ± 1.1 years. The patients were divided into three groups: TM group (22 patients with an average age of 58.6 ± 1.8 years), an EI group (16 patients with an average age of 57.5 + 1.9 years), and an AI group (13 patients with an average age of 58 ± 2.2 years).
The main causes of EC complicated with mTEF were tumor invasion, radiotherapy, chemotherapy, and radical surgery. Direct invasion of EC accounted for 43.1% of the cases (22/51); radiotherapy accounted for 23.5% of the cases (12/51); radical surgery accounted for 29.5% of the cases (15/51); and chemotherapy accounted for 3.9% of the cases (2/51) (Table 1).
Therapeutic Effects
3.2
We did not identify a significant influence of sex, age, fistula cause, fistula location, or tumor stage on therapeutic effect, but we did observe significant differences among the different treatment groups (p = 0.015), with better symptom improvement in the AI group than the TM group. By contrast, the results did not indicate a significant difference in symptom improvement between the EI and TM groups (Table 2).
Survival Analysis
3.3
Survival
3.3.1
The median overall survival (OS) duration was 87 days (TM group, 42 days; AI group, 108 days; EI group, 104 days) and the mean OS duration was 130.1 days (TM group, 88.1 days; AI group, 153.5 days; EI group, 166.1 days). The survival duration was significantly shorter in the TM group than in the AI and EI groups (p = 0.032 and p = 0.030, respectively; Table 3). Figure 2 presents the survival duration according to the treatment regimen and fistula stage.
Survival analysis with independent factors. Box plots showing the relationship between (A) survival time and treatment and (B) survival time and tumor stage. The boxes represent the median and interquartile range (IQR), and the whiskers represent ±1.5 IQR.
Survival at 1 Month, 6 Months, and Overall Survival (OS)
3.3.2
The survival curves created using the Kaplan–Meier method showed that 1‐month survival was higher in the AI and EI groups than in the TM group (p = 0.011) (Figure 3). However, survival at 6 months (p = 0.374, Figure 4) and OS (p = 0.41, Figure 5) did not differ between groups.
Kaplan–Meier analysis of 1‐month survival in patients with EC with mTEF.
Kaplan–Meier analysis of 6‐month survival in patients with EC with mTEF.
Kaplan–Meier analysis of OS in patients with EC with mTEF.
Univariate Cox analysis showed that the treatment regimen was an independent predictor of 1‐month survival but not 6‐month survival (Table 4). However, the analysis indicated that fistula cause and tumor stage were independent predictors of 6‐month survival.
Discussion
4
EC is a common malignant tumor of the digestive tract. Tumor invasion, radiotherapy, chemotherapy, and radical surgery in advanced EC can often lead to an mTEF [15]; approximately 60% of which are secondary to chemoradiotherapy [1, 2]. Due to its propensity to cause life‐threatening secondary complications such as severe malnutrition, aspiration pneumonia, and massive hemorrhage, most patients die within 3–4 months of diagnosis, with a median survival period of only 1–6 weeks. Despite the rapid advancements in cancer treatment and supportive care, the incidence of EC complicated with mTEF has been increasing annually. For example, a study by Manini et al. involving 1943 EC patients in the 1970s reported an mTEF incidence of only 4.94% [16]. Since 2010, the incidence of EC with mTEF has risen to 8%–10% [17].
The treatment modalities for mTEF include surgical and nonsurgical approaches. Surgery remains the preferred treatment for mTEF, but the reported closure rate of early bronchial fistulas within 14 days after pneumonectomy is only 1.9% (14/733). Moreover, most patients are ineligible for surgery due to severe infection and malnutrition [8]. Nonsurgical treatments encompass tumor medical therapy, chemoradiotherapy, and interventional therapy. Tumor medical therapy (TM) has limited value in mTEF patients, with unclear efficacy in symptom relief [18].
In the treatment of TEF, radiotherapy and chemotherapy are perhaps the most controversial. At the beginning of this century, some scholars still advocated that radiotherapy and chemotherapy should be included in mTEF treatment protocols [2], arguing that there was no evidence that they would exacerbate mTEF progression and claiming they could improve patient survival. Although radiotherapy and chemotherapy are not formally recommended as standard treatment for TEF, in clinical practice, certain antitumor therapies are still administered to patients with good general condition and no absolute contraindications [19].
The goal of interventional therapy is to create an occlusion between the airway and esophagus, thereby enabling enteral nutrition and reducing bronchial contamination, so as to rapidly relieve symptoms and avoid the need for surgery [20, 21]. Current interventional treatments mainly include two types. One is biological adhesives: in some previous studies, endoscopic injection of “biological glues” such as fibrin glue has achieved efficacy for smaller fistulas (diameter < 5 mm). However, for larger fistulas, the effectiveness of such adhesives is limited, and they may damage the endoscope if they flow into the operating channel. The other is mesenchymal stem cell transplantation, which also holds promise for TEF repair but remains in the exploratory stage [22].
Another interventional treatment is stent implantation. Placing airway or esophageal stents has become the most commonly used supportive treatment for mTEF. Currently, there are two main interventional occlusion methods: one is to occlude the fistula by placing an esophageal stent via gastroscopy, and the other is to place an occluder or airway stent via bronchoscopy. If the size and location of the fistula are suitable, occluders commonly used in cardiology, such as ventricular septal defect (VSD) or atrial septal defect (ASD) occluders, are also an option [23]. In this study, the interventional treatments used included conventional esophageal stents and airway stents, and a small number of patients also received ventricular septal defect occluders.
This approach of placing stents through natural lumens to occlude mTEF is minimally invasive. It is reported that the short‐term aspiration symptom relief rate can reach 75%–90% [9, 10]. For example, Fruchter et al. treated 31 mTEF patients with atrial septal defect occluders and found that 30 patients experienced immediate symptom relief after treatment, making it suitable for all emergency cases and patients requiring long‐term treatment [24]. Our study results also showed that AI and EI can fully relieve the symptoms of advanced EC patients with mTEF within 1 month after treatment, with ORR rates of 84.6% and 75%, respectively. In terms of symptom improvement, our results are basically consistent with previous reports.
Meanwhile, these two types of stents also have their respective advantages and disadvantages. Compared with esophageal stents, airway stents can not only treat mTEF but also prevent airway stenosis. Additionally, although esophageal stents can better address the problem of dysphagia, their displacement may lead to life‐threatening risks of airway stenosis and bleeding; this may also account for the survival differences between the two interventional methods.
Balazs et al. conducted a retrospective survey of 264 EC patients with mTEF and found that the survival time of patients who received esophageal interventional therapy (EI) was significantly longer than that of patients who received nutritional support (3.4 vs. 1.8 months) [17]. Furthermore, Herth et al. performed a prospective study on 112 mTEF patients who underwent airway and/or esophageal stent implantation: 65 patients received airway stents, 37 received esophageal stents, and 10 received combined airway‐esophageal stents [25]. The study showed an average OS of 236.6 days (219.1 days in the airway stent group, 262.8 days in the esophageal stent group, and 252.9 days in the combined stent group), and the QoL of all three groups significantly improved after treatment.
The results of our study also showed that patients' symptoms significantly improved after interventional therapy. The OS time was 130.1 days (TM group, 42 days; AI group, 108 days; EI group, 104 days). The difference in average survival time between our study and Herth's study may stem from the following reasons: the average age of patients in our study was 58 years, while that in Herth's prospective study was 52 years. Another explanation is that Herth's study was prospective, with regular follow‐ups and more symptomatic treatments after interventional therapy; in contrast, our study was retrospective, and most patients did not receive regular follow‐ups after interventional therapy, leading to significant differences in survival time.
Since Herth's study was published, many studies have explored the safety and efficacy of AI and EI in the treatment of mTEF; but few have compared the efficacy of AI and EI.
This study is consistent with previous findings, showing that patients treated with AI or EI had better survival rates than those treated with TM. One possible explanation is that patients in the AI and EI groups had better general conditions than those in the TM group, likely because interventional therapy enables enteral nutrition and reduces bronchial contamination. Tumor stage was also associated with survival, suggesting that AI may prolong survival in patients with Stage I, II, and III EC.
Kaplan–Meier analysis showed that the 1‐month survival rate of patients in the AI and EI groups was higher than that in the TM group, but the analysis did not show significant differences in 6‐month survival rates and OS between groups (Figure 3). This finding suggests that EI and AI can reduce the short‐term mortality of mTEF patients, but may not significantly improve long‐term mortality and OS. One possible reason is that interventional therapy improves early survival by creating an occlusion between the airway and esophagus to enable enteral nutrition and reduce aspiration. However, in addition to tumor progression, these patients also face malnutrition, repeated airway aspiration, and episodes of pneumonia, which may exacerbate their condition. Therefore, compared with TM treatment, interventional therapy appears to confer higher early survival rates in EC patients with mTEF.
This study has several limitations. First, it is a single‐center study, so only a limited number of patients could be included. Second, the follow‐up period was relatively short. Therefore, prospective randomized controlled trials with longer follow‐up periods and larger sample sizes are needed to validate these results.
Conclusion
5
In summary, this study confirms that AI and EI can serve as effective treatment modalities for EC patients with mTEF. These interventions not only reduce short‐term mortality by occluding fistulas and restoring enteral nutrition, but also enable AI to rapidly improve symptoms such as dyspnea within 1 month, thereby enhancing QoL. The findings suggest that clinicians should actively incorporate AI and EI into first‐line palliative treatment strategies for EC with mTEF, especially for elderly patients and other critically ill individuals unable to tolerate surgery. The minimally invasive nature and low complication rate of these interventions provide a rationale for their promotion in primary healthcare settings. Future research should further optimize treatment protocols through multicenter studies.
Author Contributions
Pei Huang: acquisition of data and drafting the initial manuscript. Jinghua Cui: conception and design of the study. Zhenbang Lie: analysis and interpretation of data. Jing Li: critical revision of the manuscript for important intellectual content and final editing. All authors contributed to the study, approved the final version of the manuscript, and agree to be accountable for all aspects of the work.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. S. Kim , D. Khemasuwan , J. Diaz‐Mendoza , and A. C. Mehta , “Management of Tracheo‐Oesophageal Fistula in Adults,” European Respiratory Review 29, no. 158 (2020): 200094, 10.1183/16000617.0094-2020.33153989 PMC 9488631 · doi ↗ · pubmed ↗
- 2F. M. Shamji and R. Inculet , “Management of Malignant Tracheoesophageal Fistula,” Thoracic Surgery Clinics 28, no. 3 (2018): 393–402, 10.1016/j.thorsurg.2018.04.007.30054077 · doi ↗ · pubmed ↗
- 3H. Wang , M. Tao , N. Zhang , et al., “Airway Covered Metallic Stent Based on Different Fistula Location and Size in Malignant Tracheoesophageal Fistula,” American Journal of the Medical Sciences 350 (2015): 364–368, 10.1097/MAJ.0000000000000565.26422803 · doi ↗ · pubmed ↗
- 4M. F. Reed and D. J. Mathisen , “Tracheoesophageal Fistula,” Chest Surgery Clinics of North America 13, no. 2 (2003): 271–289, 10.1016/s 1052-3359(03)00030-9.12755313 · doi ↗ · pubmed ↗
- 5B. L. Bick , L. M. Song , N. S. Buttar , et al., “Stent‐Associated Esophagorespiratory Fistulas: Incidence and Risk Factors,” Gastrointestinal Endoscopy 77, no. 2 (2013): 181–189, 10.1016/j.gie.2012.10.004.23245798 · doi ↗ · pubmed ↗
- 6I. Ahmad , K. S. Chufal , R. Bajpai , et al., “Malignant Esophagorespiratory Fistulas: A Comparative Effectiveness Survival Analysis,” BMJ Supportive & Palliative Care 14 (2020): e 1700–e 1703.10.1136/bmjspcare-2020-00237032826266 · doi ↗ · pubmed ↗
- 7J. K. Grass , N. Küsters , F. L. von Döhren , et al., “Management of Esophageal Cancer‐Associated Respiratory‐Digestive Tract Fistulas,” Cancers 14, no. 5 (2022): 1220, 10.3390/cancers 14051220.35267527 PMC 8909259 · doi ↗ · pubmed ↗
- 8A. Mazzella , A. Pardolesi , P. Maisonneuve , et al., “Bronchopleural Fistula After Pneumonectomy: Risk Factors and Management, Focusing on Open‐Window Thoracostomy,” Seminars in Thoracic and Cardiovascular Surgery 30 (2018): 104–113, 10.1053/j.semtcvs.2017.10.003.29109057 · doi ↗ · pubmed ↗