Intraoperative Asystole Induced by Intramedullary Reaming During Orthopedic Surgery
Jacob McCleerey, Gina DiMattia, Takor Arrey-Mbi

TL;DR
A 71-year-old woman experienced temporary heart stoppage during orthopedic surgery, likely due to pressure from a procedure called intramedullary reaming, highlighting a rare but important surgical complication.
Contribution
This case report adds to the limited literature on intraoperative asystole during intramedullary reaming and suggests a parasympathetic-mediated mechanism.
Findings
The patient experienced two episodes of asystole during intramedullary reaming, which resolved upon stopping the procedure.
The suspected cause is parasympathetic-mediated bradycardia due to transmitted pressure from reaming.
The patient remained stable and required no interventions, emphasizing the transient nature of the complication.
Abstract
Intramedullary nailing has become the standard of care for the treatment of femoral diaphyseal fractures due to its low incidence of complications and return of limb function. We present a case of a rare complication that we believe deserves attention for further studies and research. A 71-year-old female with a past medical history of essential hypertension, hypothyroidism, and osteoarthritis of the bilateral knees presented after a ground-level fall resulting in a right intertrochanteric femoral fracture. The patient underwent operative repair with an intramedullary nail during orthopedic surgery. Preprocedural vitals were stable, and no abnormalities were seen on preprocedural EKG. During the procedure, the patient experienced two episodes of asystole that began with intramedullary reaming and spontaneously resolved with cessation of reaming. The patient remained hemodynamically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
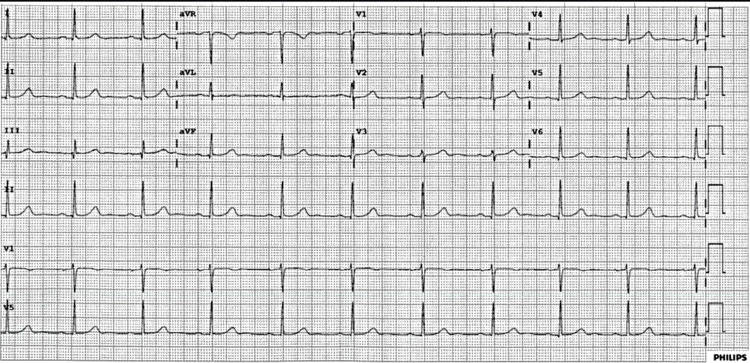 Figure 1
Figure 1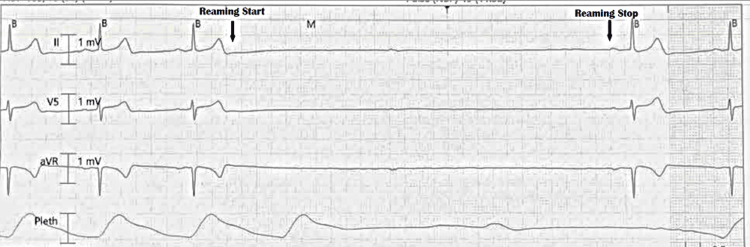 Figure 2
Figure 2| Laboratory parameter | Pre-procedure | Post-procedure | Reference range |
| WBC | 5.0 × 103/µL | 8.6 × 103/µL | 4.5–13.0 × 103/uL |
| Hemoglobin | 13.9 g/dL | 12.7 g/dL | 10.0–15.0 g/dL |
| Hematocrit | 43% | 38% | 35%–45% |
| Platelets | 289 × 103/µL | 250 × 103/µL | 140–420 × 103/µL |
| MCV | 85 fL | 85 fL | 80–98 fL |
| Sodium | 140 mmol/L | 138 mmol/L | 135–145 mmol/L |
| Potassium | 4.30 mmol/L | 3.70 mmol/L | 3.50–5.10 mmol/L |
| Chloride | 102 mmol/L | 102 mmol/L | 98–107 mmol/L |
| Bicarbonate | 27 mmol/L | 22 mmol/L | 22–31 mmol/L |
| Serum creatinine | 0.63 mg/dL | 0.72 mg/dL | 0.5–1.00 mg/dL |
| Estimated GFR | 95 mL/min/1.73m2 | 89 mL/min/1.73m2 | - |
| Glucose | 87 mg/dL | 97 mg/dL | 74–109 mg/dL |
| Calcium | 9.5 mg/dL | 8.9 mg/dL | 8.6–10.3 mg/dL |
| Albumin | 4.5 g/dL | 4.2 g/dL | 3.5–5.2 g/dL |
| TSH | 2.27 µlU/mL | - | 0.27–4.32 µlU/mL |
| T4 | 1.27 ng/dL | - | 0.58–1.64 ng/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Sedative Agents · Anesthesia and Pain Management · Nausea and vomiting management
Introduction
Intramedullary nailing is the standard of care for femoral diaphyseal fractures [1,2]. High fracture union rates, an excellent return of limb function, and a low incidence of complications make intermedullary nailing one of the most successful orthopedic procedures [1]. However, as with any surgical procedure, risks and complications exist. Some clinical complications that have been associated with intramedullary nailing include fat embolism, acute respiratory distress syndrome, infection, and dysrhythmias [1,2]. Two prior case reports of asystole during reaming of the intermedullary femoral canal have been described by Martinez et al. and Wooster et al. [3,4]. In each of these cases, the patient was noted to have severe bradycardia/asystole that resolved spontaneously after reaming stopped. We present a case of transient intraoperative asystole also triggered by right femoral intramedullary reaming with spontaneous resolution when intermedullary reaming was terminated. The objective of this case report is to describe a rare complication that has been associated with reaming during intramedullary nail procedures to bring focus to this complication for further research that will hopefully benefit both surgical procedures and patient care.
Case presentation
A 71-year-old female with a past medical history of essential hypertension, hypothyroidism, and osteoarthritis of the bilateral knees presented to the emergency room after a ground-level fall resulting in severe right hip pain. The patient had been independently ambulatory in the past with no other history of falls, osteoporosis, or previous fractures. The patient had no prior cardiac history before her procedure and had a revised Cardiac Risk Index score of less than 1, which did not warrant any further cardiac preoperative risk assessment. Preliminary EKG showed normal sinus rhythm with no conduction abnormality present. Laboratory results were unremarkable (Table 1).
She was found to have a right intertrochanteric femoral fracture visualized on X-ray and CT, which necessitated evaluation by orthopedic surgery. Orthopedic surgery recommended operative repair with an intramedullary nail. Her vitals before the start of the procedure were a heart rate of 71 beats per minute, systolic blood pressure of 152 mmHg, diastolic blood pressure of 62 mmHg, and an oxygen saturation of 97% breathing ambient air. Baseline EKG showed normal sinus rhythm (Figure 1). She remained hemodynamically stable after induction of anesthesia. However, during intramedullary reaming, the patient abruptly experienced episodes of asystole. The longest asystole episode lasted six seconds (Figure 2). The asystole episode spontaneously resolved with cessation of reaming (Figure 2).
Baseline EKG showing normal sinus rhythm.
Intraoperative EKG monitoring showing reamer on and off.
The patient remained hemodynamically stable for the remainder of the procedure. Cardiology was consulted intraoperatively, and as the patient’s asystole acutely resolved to normal sinus rhythm after intramedullary reaming was stopped, no acute interventions were necessary, such as cardiopulmonary resuscitation or pharmacological interventions. Other etiologies for asystole, including anesthetics, acute ischemia, and fat embolism, were discussed but ruled out as the patient remained hemodynamically stable and asystole resolved upon cessation of intramedullary reaming. Limited intraoperative echocardiogram showed preserved ejection fraction with no significant left ventricular wall motion abnormality. Given the return to baseline and ruling out other possible considerations, it was decided by the surgical and cardiology teams that the procedure should continue. Cardiology was consulted postoperatively and recommended further evaluation with a full transthoracic echocardiogram (TTE). TTE demonstrated normal left ventricular size and function with an ejection fraction of greater than 65%, normal wall motion, and no evidence of valvular heart disease. Cardiac biomarkers drawn during the procedure returned normal, and the postoperative EKG was unchanged when compared to her pre-procedural EKG. She was monitored on telemetry overnight without recurrence of dysrhythmia or other conduction abnormalities and was discharged on postoperative day one.
Discussion
Possible etiologies for intraoperative cardiac arrest can include fat embolism, acute coronary syndrome, medication effects, or others. In this case, myocardial infarction was considered but was found to be unlikely given no acute ischemic changes seen on the telemetry monitors or post-procedure EKG and normal troponin level. Additionally, fat embolism syndrome is a known potential complication of long bone fractures or surgical repair. This patient did not demonstrate traditional symptoms associated with fat embolism, such as respiratory distress, neurological symptoms after the procedure, or petechial rash. Given the patient’s hemodynamic and respiratory stability outside of the reaming period as well as the absence of post-procedure symptoms and typical clinical findings of known complications, it was suspected that this patient’s asystole was similar to the same mechanism described in the other case reports by Martinez et al. and Wooster et al. [3,4]. Intraoperative asystole during intramedullary reaming is a rare occurrence that has been scarcely reported in the literature. The proposed mechanism has been described as likely secondary to a vagal response or the Bezold-Jarisch reflex, resulting in bradyarrhythmia or asystole [2,4]. The pathophysiology of this reflex was described by Wilkinson and Gallagher [2] as transmitted pressures through the pelvis to the intra-abdominal organs, resulting in a vagal-mediated bradycardia. However, the pathophysiology of this reflex is not well documented, and we hope that by demonstrating this case report, as well as the previous reports mentioned, other mechanisms can be identified and investigated further.
Conclusions
Multiple etiologies of the patient’s transient asystole were considered to include intraoperative cardiac event and fat embolism. However, as the patient did not have a significant previous cardiovascular history and post-procedural workup for cardiovascular complications with troponin, EKG, and TTE was normal, these etiologies were considered to be less likely. Therefore, we conclude that this case demonstrates a transient intraoperative asystole induced by intramedullary reaming, as described by earlier case reports and the Bezold-Jarisch reflex. We believe that this finding underscores the potential cardiovascular risks associated with this common orthopedic procedure and recommend that further studies be conducted to better document and evaluate this complication. Until this reflex is better understood and described as a clear cause of intraoperative asystole during reaming, we recommend that surgeons, anesthesiologists, and cardiologists be aware of this condition and prepare for this potential complication intraoperatively.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intramedullary nailing of the lower extremity: biomechanics and biology J Am Acad Orthop Surg Bong MR Kummer FJ Koval KJ Egol KA 97106152007 https://journals.lww.com/jaaos/fulltext/2007/02000/intramedullary_nailing_of_the_lower_extremity_.4.aspx 1727725610.5435/00124635-200702000-00004 · doi ↗ · pubmed ↗
- 2The Gallagher-Wilkinson reflex Anaesthesia Wilkinson DJ Gallagher L 12201221572002 https://doi.org/10.1046/j.1365-2044.2002.02913_12.x 12437723 · pubmed ↗
- 3Reproducible transient asystolic arrest during intramedullary reaming of the femoral canal: a case report J Clin Orthop Trauma Wooster BM Nickel BT Neumann JA Lindsay DR Wellman SS 06182017 http://www.clinicalkey.com/#!/content/play Content/1-s 2.0-S 0976566217301376?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS 0976566217301376%3Fshowall%3Dtrue&referrer=https:%2F%2Fpubmed.ncbi.nlm.nih.gov%2F 10.1016/j.jcot.2017.07.010PMC 557486228878543 · doi ↗ · pubmed ↗
- 4Intraoperative dysrhythmias cease after venting during intramedullary nailing of an impending femur fracture: a case report JBJS Case Connect Martinez FA Dugdale EM Sims CR 3rd Hofer RE Sems SA 013202310.2106/JBJS.CC.22.0012637026803 · doi ↗ · pubmed ↗