Vitamin B12 Deficiency Exhibiting as Pancytopenia: A Diagnostic Conundrum
Erica Lama, Susmita Sharma

TL;DR
This case study highlights how vitamin B12 deficiency can cause pancytopenia, a condition with symptoms that mimic more serious blood disorders, emphasizing the importance of early diagnosis.
Contribution
The novelty lies in illustrating the diagnostic challenge of vitamin B12 deficiency presenting as pancytopenia and advocating for its inclusion in differential diagnosis.
Findings
Vitamin B12 deficiency can present with pancytopenia and macrocytic anemia, mimicking severe hematologic diseases.
Early supplementation with vitamin B12 led to clinical and laboratory improvement in the patient.
The case underscores the need to consider vitamin B12 deficiency in patients with unexplained pancytopenia to avoid unnecessary procedures.
Abstract
Pancytopenia is caused by impaired production and peripheral destruction of blood cells, leading to decreased levels of red blood cells (RBCs), white blood cells (WBCs), and platelets. The etiologies can be classified as reversible and irreversible causes. One of the reversible causes is Vitamin B12 deficiency. Vitamin B12 deficiency can cause various types of manifestations, including hematologic as well as neurological symptoms, and sometimes mimicking serious hematologic conditions. A 46-year-old male presented with generalized body weakness, easy fatigability, and occasional nausea with vomiting for two months. His vital signs were stable, and on physical examination, icterus was present. The patient presented with anemia accompanied by leukopenia and thrombocytopenia on complete blood count, suggesting pancytopenia. Red blood cell indices showed macrocytosis, and the peripheral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
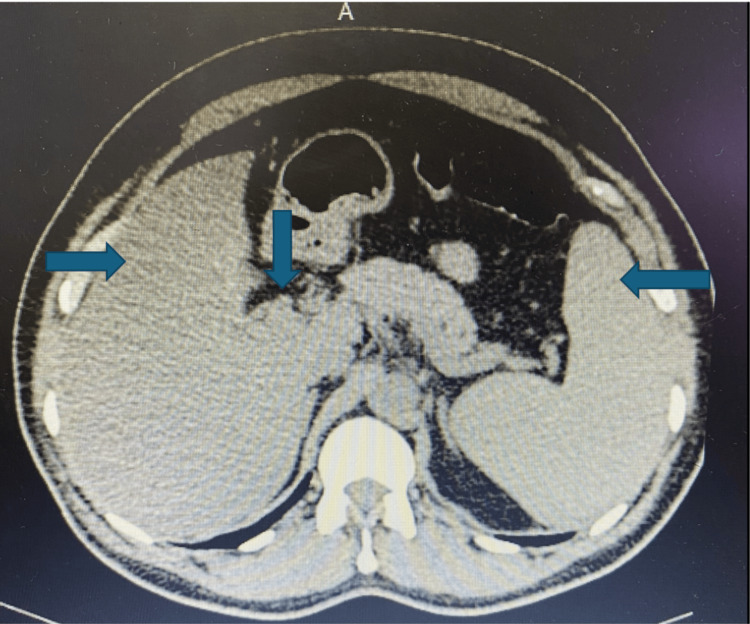 Figure 1
Figure 1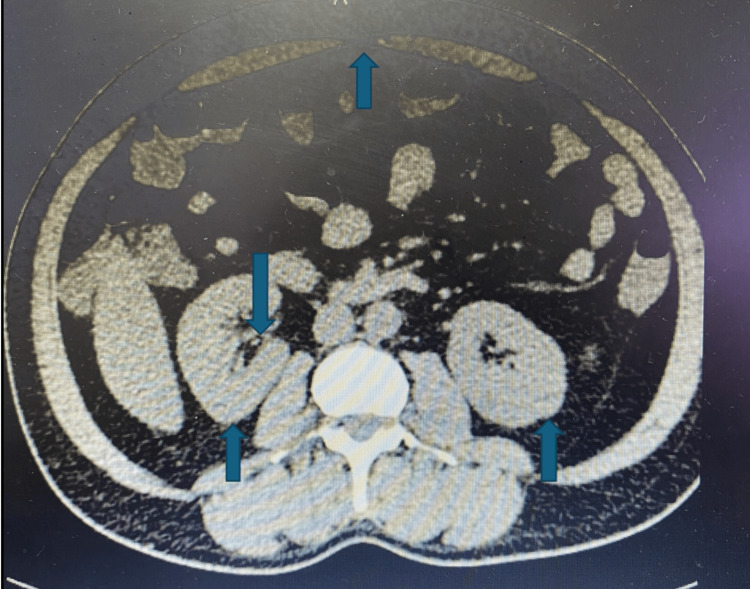 Figure 2
Figure 2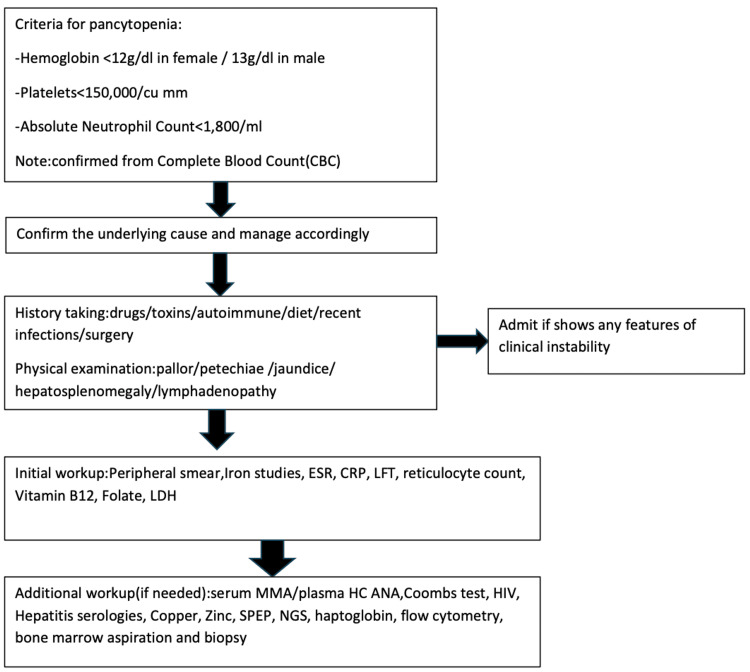 Figure 3
Figure 3| Investigations | Result | Normal range |
| HBsAg | Reactive | |
| HCV Ab | Non-reactive | |
| Anti-HAV IgG | Non-reactive | |
| Anti-HAV IgM | Non-reactive | |
| HBeAg | Non-reactive | |
| HBV DNA titer (IU/mL) | <2000 | Undetectable: <20; low viral load: 20–2000; intermediate viral load: 2000–20,000; high viral load: >20,000; active replication: >1 million |
| Lactate dehydrogenase (LDH) (U/L) | 4438 | 45-90 |
| Vitamin B12 (pg/ml) | 159 | 300-950 |
| Antinuclear antibodies (ANA) (AU/ml) | Negative (0.74) | Negative: <20; equivocal: 20–39; positive: ≥40 |
| Iron (µg/dl) | 255 | 50-170 |
| Iron saturation (%) | 74.78 | 15-50 |
| Ferritin (ng/ml) | 373 | Male: 15-200; female: 12-150 |
| C-reactive protein (mg/L) | 22.6 | <10 |
| Investigations | Day 1 | Day 2 | Day 10 | Normal range |
| Total leucocyte count (cells/µL) | 3300 | 4000 | 4240 | 4500-11,000 |
| Red blood cells (million/µL) | 1.79 | 2.39 | 2.98 | Male: 4.3-5.9; Female: 3.5-5.5 |
| Hemoglobin (gms%) | 6.9 | 8.7 | 9.9 | Male: 13.5-17.5; Female: 12-16 |
| Mean corpuscular volume (MCV) (fl) | 121.2 | 112.7 | 108.8 | 80-100 |
| Platelet (cells/µL) | 78,000 | 95,000 | 1,40,000 | 150,000-400,000 |
| Alanine aminotransferase (ALT/SGPT) (U/L) | 107 | 80 | 8-40 | |
| Aspartate aminotransferase (AST/SGOT) (U/L) | 202 | 120 | 8-40 | |
| Total bilirubin (mg/dl) | 2.5 | 1.9 | 0.1-1 | |
| Unconjugated bilirubin(mg/dl) | 1.9 | 1.8 | 0.2-0.8 |
| Serum level (pg/mL) | Interpretation |
| >300 | Normal |
| 200-300 | Borderline |
| <200 | Deficient |
| System involved | Clinical manifestations |
| Neuropsychiatric manifestations | Headache, erectile dysfunction, spinal degeneration, peripheral neuropathy, epileptiform symptoms in <20 years old individuals and psychiatric, namely, depression, mania, Alzheimer’s, and delirium in >70 years old individuals |
| Oral manifestations | Hunter glossitis |
| Hematologic manifestations | Pancytopenia, decreased hemoglobin levels, hyper-segmented neutrophils, and increased mean corpuscular volume |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Bone and Joint Diseases · Hematological disorders and diagnostics
Introduction
Pancytopenia is a hematologic disorder caused by impaired production and peripheral destruction of blood cells, leading to decreased levels of red blood cells (RBCs), white blood cells (WBCs), and platelets. The etiologies can be classified as reversible and irreversible causes. Reversible causes include viral infections, such as Epstein-Barr virus or Parvovirus B19, chronic alcohol use disorder, deficiencies in Vitamin B12, folate, iron, and certain medications. As it can be caused due to various factors, thorough assessment should be done to find out the underlying cause [1,2].
Vitamin B12, also known as cobalamin, is a water-soluble vitamin. Its sources are dairy products, eggs, and red meat. It is mainly absorbed in the terminal ileum with the aid of intrinsic factor, a glycoprotein produced by parietal cells of stomach. It is involved in DNA, fatty acids, and myelin synthesis. Due to the large hepatic stores and the low daily requirement of Vitamin B12, clinical manifestations of its deficiency often take several years to develop. The causes of Vitamin B12 deficiency are drugs that led to decreased absorption (i.e., metformin), defect in its release from food (i.e., proton pump inhibitors, H2 receptor antagonists), and malabsorption, like in pernicious anemia, chronic pancreatic insufficiency, malnutrition, post-gastrectomy, chronic liver disease and atrophic gastritis. Vitamin B12 deficiency can cause various types of manifestations, including hematological, such as pancytopenia, neurological, such as peripheral neuropathy, and sometimes mimicking serious conditions like leukemia, thrombotic thrombocytopenic purpura (TTP), or myelodysplastic syndrome. It is also found that there is a higher prevalence of Vitamin B12 deficiency in elderly population due to decreased intestinal absorption of Vitamin B12. Measurement of plasma cobalamin is the gold standard diagnostic test for Vitamin B12 deficiency [1-5].
Case presentation
A 46-year-old male, ex-tobacco user, with history of hepatitis B infection 25 years ago, for which he was treated with entecavir but lost to follow up after that, hypothyroidism under medication, and cholecystectomy, presented with generalized body weakness, easy fatiguability, and occasional nausea with vomiting for two months. He reported no recent exposure to ill individuals, travel, bleeding, blood in vomitus, black stool, shortness of breath, unintentional weight loss, alcohol consumption, and illicit drug use.
The patient’s vital signs were stable: blood pressure was 130/80 mmHg, heart rate was 84 bpm, respiratory rate was 18 breaths/min, temperature was 98.1°F, and oxygen saturation rate was 98% on room air. On physical examination, icterus was present. On systemic examination, findings were normal.
On initial blood analysis, HBsAg was reactive, whereas hepatitis C virus antibody test (HCV Ab), anti-hepatitis A virus (HAV) IgG, and anti-HAV IgM were non-reactive. On complete blood count (CBC), total leukocyte count was 3300 cells/µL, red blood cells were 1.79 million/µL, hemoglobin was 6.9 gms%, mean corpuscular volume (MCV) was 121.2 fl, platelet count was 78,000 cells/µL, and reticulocyte count was 2%. Liver function test (LFT) revealed alanine aminotransferase (ALT/SGPT) of 107 U/L, aspartate aminotransferase (AST/SGOT) of 202 U/L, total bilirubin of 2.5 mg/dl, and unconjugated bilirubin of 1.9 mg/dl. Lactate dehydrogenase was 4438 U/L, Vitamin B12 was 159 pg/ml, antinuclear antibody (ANA) was 0.74 AU/ml, iron was 255 µg/dl, iron saturation % was 74.78%, ferritin was 373 ng/ml, and C-reactive protein was 22.6 mg/L. On peripheral blood smear, teardrop cells, normocytic normochromic cells with hypersegmented neutrophils, and few macroovalocytes and polychromatophils were observed, and stool sample was negative for occult blood (Tables 1, 2).
Furthermore, Figures 1, 2 are the computed tomography scans of whole abdomen showing diffuse fatty liver, mild splenomegaly (13.93 cm) with dilated portal vein (14.1 mm), tiny right nephrolithiasis (2.3 × 2.2 mm) in lower pole of calyx, bilateral simple renal cortical cysts-Bosniak category 1 and small umbilical hernia (7.3 mm).
Computed tomography scan of the whole abdomen showing diffuse fatty liver, mild splenomegaly with dilated portal vein.
Computed tomography of the whole abdomen showing tiny right nephrolithiasis in the lower pole of the calyx, bilateral simple renal cortical cysts-Bosniak category 1, and small umbilical hernia.
During the hospital stay, gastrointestinal medicine consultation was done for hepatitis B status, and further investigations were done and advised to follow up with reports. Two pints of packed red blood cells were transfused to correct anemia (post-transfusion Hb 9.3 gms%), and vitamin supplements were started. At the time of discharge, the patient was symptomatically improving and hemodynamically stable. The patient was prescribed an oral Vitamin B12 supplement, ursodeoxycholic acid, thiamine, and was advised to follow up in one week with CBC, LFT, HBeAg, and HBV DNA titer reports.
On follow-up, the patient was symptomatically better and hemodynamically stable. According to the lab investigations, HBeAg was negative, and the HBV DNA titer was less than 2000 IU/mL. On LFT, ALT was 80 U/L, AST was 120 U/L, total bilirubin was 1.9 mg/dl, as well as unconjugated bilirubin was 1.8 mg/dl, and anti-viral was not started. Total leukocyte count was 4240 cells/µL, red blood cells were 2.98 million/µL, hemoglobin was 9.9 gms%, mean corpuscular volume (MCV) was 108.8 fl, and platelet count was 1,40,000 cells/µL.
Given the patient's history and findings of chronic hepatitis B and elevated liver enzymes, hepatic dysfunction has contributed to the Vitamin B12 deficiency. Considering that Vitamin B12 deficiency is the cause of pancytopenia, Vitamin B12 supplementation was continued.
Discussion
This discussion will simplify and aid clinicians to identify the various causes of pancytopenia, specifically Vitamin B12 deficiency, considering its wide range of manifestations and manage it effectively.
Pancytopenia can occur due to various etiologies and is often associated with other conditions. For prompt diagnosis and treatment, as shown in Figure 3, a thorough history and physical examination should be carried out, followed by appropriate management [1,6].
Workup algorithm for pancytopenia.ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; LFT: liver function test; LDH: lactate dehydrogenase; MMA: methylmalonic acid; HC ANA: antinuclear antibodies with high concentration; SPEP: serum protein electrophoresis.
In our case scenario of pancytopenia with increased MCV, normal reticulocyte count, and teardrop cells, normocytic normochromic cells with hypersegmented neutrophils, few macroovalocytes and polychromatophils on peripheral smear ruled out aplastic anemia, iron deficiency anemia, and myelodysplastic syndrome. Negative ANA, normal body temperature, and absence of hepatomegaly ruled out an autoimmune cause. Increased LDH level with a low serum Vitamin B12 level indicates Vitamin B12 deficiency. Given the patient’s history and findings of chronic hepatitis B and elevated liver enzymes, hepatic dysfunction has contributed to the Vitamin B12 deficiency [1,7]. Therefore, the values of Vitamin B12 should be known for accurate interpretation, as given in Table 3.
The clinical features seen in cobalamin-deficient individuals are given in Table 4. Regarding the treatment, administration of Vitamin B12 is the mainstay of treatment; however, the route of administration depends on the severity of the symptoms [8-13].
In severe cases, the parenteral route is preferred; however, there are some contraindications to it, specifically in individuals who use anticoagulants. The common treatment given is injection of hydroxocobalamin 1 mg via the intramuscular route on alternate days for 14 days, and then weekly injection for one to two months, but cyanocobalamin is used in the United States. Regarding oral supplements, 1-2 mg of cyanocobalamin can be taken on a daily basis. In cases with severe neurological manifestations, the treatment is continued until no further relief is seen clinically, after which two injections are given per month. Since biomarkers often return to normal levels before clinical improvement, and conversely, in cases of relapse, they should not be solely relied upon for assessment and titrating the treatment [7,8,12-17].
Conclusions
This case illustrates the importance to consider reversible and treatable causes of pancytopenia, such as Vitamin B12 deficiency. The overlapping hematologic features with serious hematological disorders, including myelodysplastic syndrome and aplastic anemia, posed a diagnostic challenge. However, careful interpretation of peripheral smear findings and targeted investigations helped avoid unnecessary invasive procedures. Clinicians should maintain a high index of suspicion for nutritional deficiencies in similar presentations, especially when supported by subtle morphological clues. Early identification and management can significantly improve outcomes and prevent misdiagnosis in resource-limited or complex clinical settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vitamin B 12 deficiency manifesting as pancytopenia, lymphadenopathy, and fever: a clinical mimic of hematologic malignancies Cureus Choi E Galicia Garcia G Kishore Anna K Albuja Altamirano MF Yip L Oh J Lee JH 0162024 https://doi.org/10.7759/cureus.6467610.7759/cureus.64676 PMC 1132680339149666 · doi ↗ · pubmed ↗
- 2A study on prevalence of vitamin B 12 deficiency in patients with pancytopenia in Western part of UP state of India Int J Trop Med Tyagi VK Batra J Tyagi V Faiz S Kumar A Tayal N 130133192024
- 3Hemolytic anemia and pancytopenia secondary to vitamin B 12 deficiency: evaluation and clinical significance Cureus Labban H Begum F Paracha A John V Islam M 0162024 https://doi.org/10.7759/cureus.5728610.7759/cureus.57286 PMC 1105916238690452 · doi ↗ · pubmed ↗
- 4Unmasking vitamin B 12 deficiency misdiagnosed as myelodysplastic syndrome Case Rep Hematol Jamil M Nasser Z Jamil D Sheqwara JZ 325822720242024 https://doi.org/10.1155/2024/32582273965518610.1155/2024/3258227 PMC 11628167 · doi ↗ · pubmed ↗
- 5Case report: Vitamin B 12 deficiency-associated hemolytic anemia Front Hematol Sainatham C Dy PS Kaushik S 144624132024
- 6Approach to pancytopenia: diagnostic algorithm for clinical hematologists Blood Rev Gnanaraj J Parnes A Francis CW Go RS Takemoto CM Hashmi SK 361367322018 https://doi.org/10.1016/j.blre.2018.03.0012955536810.1016/j.blre.2018.03.001 · doi ↗ · pubmed ↗
- 7A brief overview of the diagnosis and treatment of cobalamin (B 12) deficiency Food Nutr Bull Wolffenbuttel BH Mc Caddon A Ahmadi KR Green R 0945202410.1177/0379572124122950038987879 · doi ↗ · pubmed ↗
- 8How I treat cobalamin (vitamin B 12) deficiency Blood Carmel R 2214222111220081860687410.1182/blood-2008-03-040253 PMC 2532799 · doi ↗ · pubmed ↗