A Rare Case of Intravascular Large B-cell Lymphoma Presenting as Leukemic Phase in a Patient With HCV-Related Cirrhosis
Michael Assefa

TL;DR
A rare case of aggressive lymphoma presenting as a leukemic phase in a patient with cirrhosis is reported, highlighting diagnostic challenges in such complex cases.
Contribution
Presentation of a rare case of IVLBCL with a leukemic phase in a cirrhotic patient, emphasizing diagnostic difficulties.
Findings
Intravascular large B-cell lymphoma was confirmed through peripheral smear and flow cytometry.
The patient's presentation included a leukemic phase, a rare manifestation of IVLBCL.
Liver dysfunction complicated the diagnosis due to overlapping symptoms with lymphoma.
Abstract
We report a rare case of a 65-year-old man with decompensated cirrhosis due to alcohol and HCV, who presented with altered mental status, hypotension, and a diffuse rash. Laboratory findings were notable for leukocytosis, severe coagulopathy, and acute kidney injury. Peripheral smear and flow cytometry confirmed intravascular large B-cell lymphoma (IVLBCL), a rare and aggressive subtype of non-Hodgkin lymphoma characterized by intravascular proliferation of malignant lymphocytes. Even more rarely, the patient presented with a leukemic phase, marked by circulating lymphoma cells, a presentation reported in only a few cases worldwide. The diagnostic challenge was further compounded by liver dysfunction, as features of advanced cirrhosis, such as coagulopathy, encephalopathy, and renal injury closely overlapped with lymphoma-related findings. This case underscores the need for a broad…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
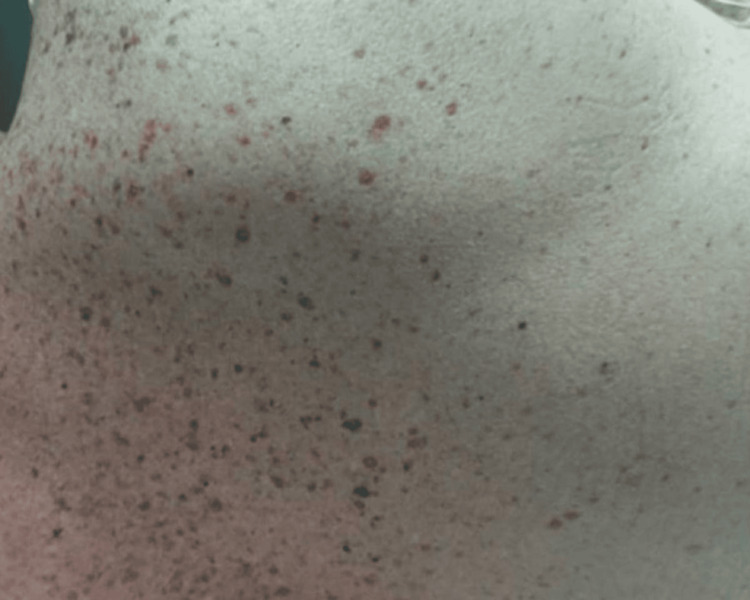 Figure 1
Figure 1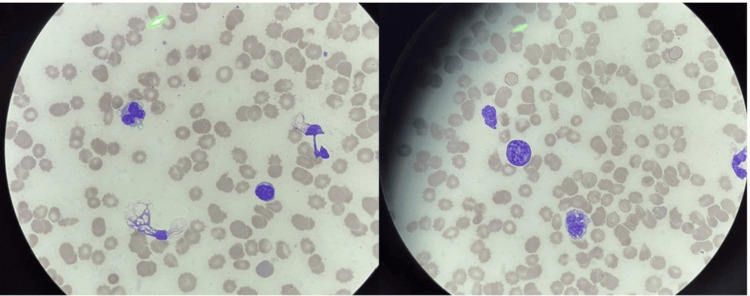 Figure 2
Figure 2| Laboratory Test | Patient Value | Reference Range |
| White blood cell count | 47×10⁹/L | 4.0-10.0×10⁹/L |
| Hemoglobin level | 10.2 g/dL | 13.5-17.5 g/dL (male) |
| Platelet count | 42×10⁹/L | 150-450×10⁹/L |
| International normalized ratio | 3.6 | 0.9-1.2 |
| Partial thromboplastin time | 44 seconds | 25-35 seconds |
| D-dimer level | >20 μg/mL | <0.5 μg/mL |
| Fibrin monomer test | Positive | Negative |
| Fibrinogen level | 140 mg/dL | 200-400 mg/dL |
| Serum creatinine | 3.63 mg/dL | 0.6-1.3 mg/dL |
| Blood urea nitrogen | 80 mg/dL | 7-20 mg/dL |
| Serum lactate | 11.4 mmol/L | 0.5-2.2 mmol/L |
| Serum uric acid | 10.1 mg/dL | 3.5-7.2 mg/dL |
| Serum ammonia | 62 μmol/L | 15-45 μmol/L |
| Total bilirubin | 9.2 mg/dL | 0.1-1.2 mg/dL |
| Aspartate aminotransferase | 447 U/L | 10-40 U/L |
| Alanine aminotransferase | 73 U/L | 7-56 U/L |
| Alkaline phosphatase | 171 U/L | 44-147 U/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCNS Lymphoma Diagnosis and Treatment · Neurological Complications and Syndromes · Moyamoya disease diagnosis and treatment
Introduction
Intravascular large B-cell lymphoma (IVLBCL) is a rare, aggressive subtype of diffuse large B-cell lymphoma, characterized by the proliferation of malignant lymphocytes within the lumina of small vessels, particularly capillaries and post-capillary venules, without forming a discrete tumor mass or causing lymphadenopathy [1]. It often presents with nonspecific systemic symptoms and is frequently diagnosed post-mortem. In Western populations, IVLBCL commonly involves the skin and central nervous system [2]. According to population-based data from the Surveillance, Epidemiology, and End Results (SEER) Program and the National Cancer Database from 2000 to 2013, the incidence of IVLBCL is approximately 0.095 cases per 1,000,000 persons per year in the United States [3]. The leukemic-phase presentation of IVLBCL corresponds to Stage IV disease and is characterized by circulating neoplastic lymphoid cells in the peripheral blood. This presentation is exceedingly rare and has been described only in isolated case reports and small series [4]. We present a diagnostically challenging case of IVLBCL presenting in the leukemic phase in a patient with HCV-related decompensated cirrhosis. The underlying malignancy was obscured by overlapping features of advanced liver disease, including coagulopathy, encephalopathy, and renal dysfunction, making the timely recognition of the lymphoma more difficult.
Case presentation
A 65-year-old man with a history of decompensated cirrhosis due to alcohol use and chronic HCV infection, hypertension, type 2 diabetes mellitus, obstructive sleep apnea, and seizure disorder presented to the emergency department with confusion and hypotension. He had been recently evaluated in the hepatology clinic and was on the wait list for liver transplantation. His wife reported the onset of a petechial facial rash over the previous four to five days, accompanied by increasing lethargy. He had also recently returned from a vacation on the Mississippi River.
On examination, the patient was hypotensive (blood pressure 94/47 mmHg), afebrile, and had a heart rate of 70 and a respiratory rate of 20. A diffuse, non-blanching, non-pruritic, erythematous maculopapular rash, consisting of flat erythematous areas interspersed with raised, coalescing papules, was noted across his face, chest, and back (Figure 1). Neurologically, he was intermittently confused and responded slowly.
Diffuse papular rash on torsoA non-blanching, erythematous, coalescing papular rash observed over the back on initial physical examination.
Initial laboratory evaluation demonstrated profound cytopenias, coagulopathy, renal and hepatic dysfunction, and severe metabolic disturbances (Table 1). Laboratory tests revealed marked leukocytosis (white blood cell count 47×10⁹/L), anemia (hemoglobin 10.2 g/dL), and thrombocytopenia (platelet count 42,000/μL). Coagulation studies were consistent with disseminated intravascular coagulation, showing an international normalized ratio of 3.6, a partial thromboplastin time of 44 seconds, D-dimer >20 μg/mL, positive fibrin monomer, and a decline in fibrinogen levels from 140 to 88 mg/dL. Metabolic panels indicated acute kidney injury (creatinine 3.63 mg/dL, blood urea nitrogen 80 mg/dL), progressive lactic acidosis (lactate rising from 11.4 to 18 mmol/L), elevated uric acid (10.1 mg/dL), and hyperammonemia (62 μmol/L). Liver function tests showed rising bilirubin (from 9.2 to 9.9 mg/dL), aspartate aminotransferase decreasing from 447 to 379 U/L, alanine aminotransferase of 73 U/L, and alkaline phosphatase declining from 171 to 137 U/L. The calculated model for the end-stage liver disease score was 38.
The patient was admitted to the intensive care unit with a working diagnosis of septic or distributive shock, acute kidney injury, disseminated intravascular coagulation, and hepatic encephalopathy. Management included broad-spectrum antibiotics, intravenous fluids, albumin, bicarbonate infusion for metabolic acidosis, dextrose for hypoglycemia, and cryoprecipitate for hypofibrinogenemia. Rifaximin was added to his home lactulose regimen. Paracentesis for ascites revealed a transudative profile. Continuous renal replacement therapy was initiated. Infectious workup, including blood, urine, and ascitic fluid cultures, was negative. There was no clinical or laboratory evidence of an acute hepatitis C flare at the time of presentation.
Peripheral smear revealed abnormal circulating lymphocytes, and flow cytometry confirmed aggressive B-cell lymphoma consistent with IVLBCL (Figure 2).
Peripheral blood smear showing abnormal lymphocytesPeripheral smear demonstrates circulating atypical lymphocytes with irregular nuclear contours and scant cytoplasm, consistent with intravascular large B-cell lymphoma (IVLBCL).
Although his hemodynamics briefly improved with resuscitation, his neurologic function declined, and he became obtunded. The diagnosis rendered him ineligible for liver transplantation. Plans for rasburicase and dexamethasone were discussed, but the family ultimately elected comfort care. The patient passed away a few days after presentation.
Discussion
IVLBCL is a pathologically distinct, clinically aggressive, and exceedingly rare subtype of extranodal large B-cell lymphoma defined by the selective growth of malignant lymphocytes within the lumina of small blood vessels. It typically presents with systemic symptoms such as B symptoms, cytopenias, and neurologic or cutaneous involvement, often without detectable lymphadenopathy, factors that contribute to diagnostic delay and poor outcomes in many cases [1,2].
Although the true incidence of IVLBCL remains unknown [4], a population-based study using U.S. SEER and National Cancer Database (NCDB) data estimated an age-adjusted incidence of 0.095 cases per 1,000,000 from 2000 to 2013, with a significant annual increase of 9.84% [5]. Despite its intravascular localization, a leukemic phase, characterized by abundant circulating lymphoma cells, is extremely rare. A retrospective review from MD Anderson Cancer Center identified only six such cases, each with ≥10% lymphoma cells in peripheral blood, often with bone marrow involvement, CD5 positivity, complex cytogenetics, and high mortality [6]. Recognition of this rare presentation expands the clinicopathologic spectrum of IVLBCL and underscores its diagnostic challenge.
Cirrhosis, particularly due to chronic HCV infection, further complicates the clinical picture. The overlap of cirrhosis-related features, such as encephalopathy, cytopenias, coagulopathy, and multiorgan dysfunction, may delay the recognition of an underlying hematologic malignancy. Cirrhosis is associated with chronic immune dysregulation, impaired clearance of malignant clones, and systemic inflammation, all of which can increase the risk of lymphoproliferative disorders [7,8]. This immune dysfunction, often referred to as cirrhosis-associated immune dysfunction syndrome (CAIDS), involves both immune suppression and persistent inflammation that impair immune surveillance [9].
In patients with HCV-related cirrhosis, the risk of B-cell non-Hodgkin lymphoma is further elevated due to direct lymphotropic effects of the virus [10]. In this case, the patient’s clinical decline was initially attributed to hepatic decompensation and presumed sepsis. However, the degree of leukocytosis, elevated lactate and uric acid levels, and atypical cutaneous findings prompted hematologic investigation. The presence of numerous circulating lymphoma cells likely reflected a leukemic variant of IVLBCL, an exceedingly rare manifestation.
This case reinforces the importance of maintaining a broad differential diagnosis in patients with cirrhosis and systemic decline. It also highlights how cirrhosis can obscure signs of aggressive malignancies, contributing to diagnostic delay and limiting treatment options.
Conclusions
IVLBCL is a rare and aggressive malignancy that may present atypically with circulating disease mimicking a leukemic phase. This unusual presentation, coupled with overlapping features of hepatic decompensation and systemic inflammation, makes timely diagnosis especially challenging in patients with cirrhosis.
This case emphasizes the importance of maintaining a broad differential diagnosis when evaluating cirrhotic patients with multiorgan dysfunction, cytopenias, or unexplained systemic decline. Early consideration of hematologic malignancy and prompt hematopathologic investigation can be critical to avoid delays in diagnosis and missed opportunities for treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intravascular lymphoma: clinical presentation, natural history, management and prognostic factors in a series of 38 cases, with special emphasis on the 'cutaneous variant'Br J Haematol Ferreri AJ Campo E Seymour JF 17318312720041546162310.1111/j.1365-2141.2004.05177.x · doi ↗ · pubmed ↗
- 2Leukosialin (CD 43) defines hematopoietic progenitors in human embryonic stem cell differentiation cultures Blood Vodyanik MA Thomson JA Slukvin II 2095210510820061675768810.1182/blood-2006-02-003327 PMC 1895535 · doi ↗ · pubmed ↗
- 3Ponzoni M, Ferreri AJM. Clinical manifestations, pathologic features, and diagnosis of intravascular large B cell lymphoma. Up To Date 5 2025 Ponzoni M Ferreri AJM 2025 Waltham, MA 232025 https://www.uptodate.com/contents/intravascular-large-b-cell-lymphoma
- 4Case report: intravascular large B-cell lymphoma: a clinicopathologic study of four cases with review of additional 331 cases in the literature Front Oncol Han Y Li Q Wang D 8831411220223564667110.3389/fonc.2022.883141 PMC 9135977 · doi ↗ · pubmed ↗
- 5Intravascular large B-cell lymphoma in the United States (US): a population-based study using Surveillance, Epidemiology, and End Results program and National Cancer Database Leuk Lymphoma Rajyaguru DJ Bhaskar C Borgert AJ Smith A Parsons B 1958201710.1080/10428194.2017.128736328278725 · doi ↗ · pubmed ↗
- 6From the archives of MD Anderson Cancer Center: intravascular large B-cell lymphoma with numerous circulating lymphoma cells Ann Diagn Pathol Qiu L Wang SA Vega F 1519345820223529908110.1016/j.anndiagpath.2022.151934 · doi ↗ · pubmed ↗
- 7WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues IARC Swerdlow SH Campo E Harris NL 2017
- 8Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment Am J Hematol Gertz MA 8488609520203226702010.1002/ajh.25819 · doi ↗ · pubmed ↗