Public Understanding of and Engagement With Community Health Workers and Promotores de Salud: Findings From Two National Surveys
Elizabeth A. Rohan, Julie S. Townsend, Andrea Torres, Hope L. Thompson, Dawn M. Holman, Avid Reza, Felicia Solomon Tharpe, Erin Caple, Ashley Wennerstrom

TL;DR
This study explores how familiar the public is with community health workers and finds that Hispanic/Latino individuals are more likely to have interacted with them.
Contribution
The paper provides the first national data on public familiarity and interactions with community health workers in the US.
Findings
62.4% of Spanish-speaking respondents were familiar with CHWs, compared to 52.1% of English-speaking respondents.
42.0% of Estilos respondents had interacted with CHWs, compared to 16.7% of FallStyles respondents.
Most interactions with CHWs occurred in healthcare settings rather than community or religious settings.
Abstract
Community health workers (CHWs) can improve health by helping people navigate health care services and systems and connecting them to community services that address nonmedical factors such as food insecurity, housing, and transportation. While CHWs have long been part of the US public health system, there are no data, to our knowledge, on the public’s familiarity and interactions with CHWs. We analyzed data from the 2022 Porter Novelli FallStyles and Estilos surveys, online market research surveys of the general public delivered in English (FallStyles) or primarily Spanish (Estilos). Each survey asked the same 4 questions on familiarity and interactions with CHWs, including, for respondents reporting having interacted with CHWs, the types of issues CHWs helped them with. Of 3,410 FallStyles respondents, 52.1% were familiar with CHWs, and 16.7% had interacted with a CHW. Of 954…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
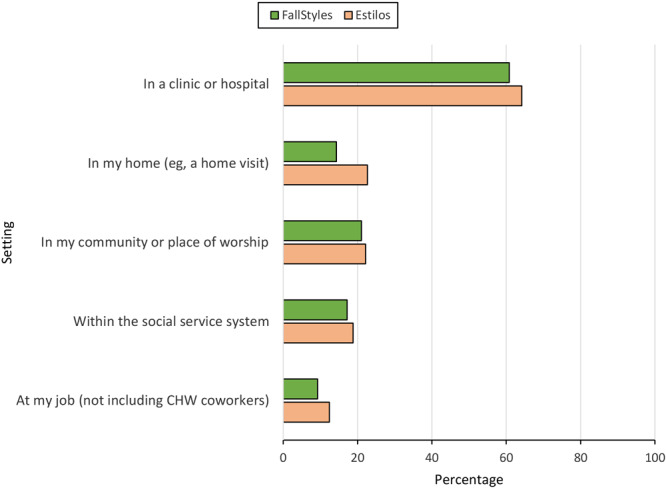 Figure 1
Figure 1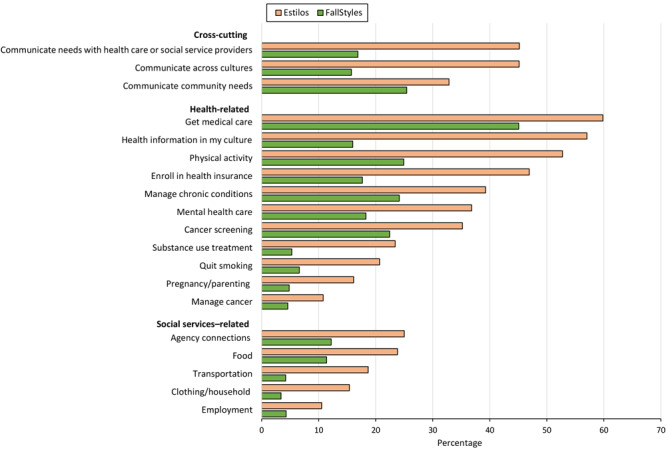 Figure 2
Figure 2| Characteristic | FallStyles, no. (%) | Estilos, no. (%) |
|---|---|---|
| | 3,410 | 954 |
| | ||
| American Indian or Alaska Native | 46 (1.3) | — |
| Asian | 206 (6.1) | |
| Black or African American | 400 (11.8) | |
| Hispanic or Latino | 442 (13.0) | |
| Native Hawaiian or Pacific Islander | 11 (0.3) | |
| White | 2,224 (65.4) | |
| I identify equally with more than one | 72 (2.1) | |
| | ||
| 18–29 | 660 (19.3) | 219 (22.9) |
| 30–44 | 899 (26.4) | 329 (34.4) |
| 45–59 | 768 (22.5) | 235 (24.6) |
| 360 | 1,083 (31.8) | 172 (18.0) |
| | ||
| Male | 1,657 (48.6) | 469 (49.1) |
| Female | 1,741 (51.1) | 486 (50.9) |
| | ||
| <25,000 | 425 (12.5) | 167 (17.5) |
| 25,000–49,999 | 1,138 (33.4) | 242 (25.4) |
| 50,000–74,999 | 1,064 (31.2) | 284 (29.8) |
| 375,000 | 783 (23.0) | 261 (27.4) |
| | ||
| Less than high school diploma | 308 (9.0) | 259 (27.1) |
| High school graduate | 961 (28.2) | 261 (27.4) |
| Some college | 923 (27.1) | 242 (25.4) |
| College diploma or more | 1,218 (35.7) | 192 (20.1) |
| | ||
| Northeast | 582 (17.1) | 132 (13.9) |
| South | 1,303 (38.2) | 364 (38.2) |
| Midwest | 710 (20.8) | 92 (9.7) |
| West | 815 (23.9) | 365 (38.2) |
| Characteristic | Familiar with CHWs | Interacted with CHWs | ||||||
|---|---|---|---|---|---|---|---|---|
| FallStyles | Estilos | FallStyles | Estilos | |||||
| No. (%) |
| No. (%) |
| No. (%) |
| No. (%) |
| |
|
| 1,771 (52.1) | — | 595 (62.4) | — | 570 (16.7) | — | 401 (42.0) | — |
|
| ||||||||
| 18–29 | 297 (45.0) | .01 | 117 (53.5) | .23 | 109 (16.5) | .91 | 84 (38.3) | .35 |
| 30–44 | 481 (53.9) | 234 (71.3) | 144 (16.0) | 168 (51.0) | ||||
| 45–59 | 407 (53.3) | 147 (62.6) | 128 (16.7) | 89 (37.7) | ||||
| ≥60 | 586 (54.1) | 97 (56.3) | 189 (17.5) | 60 (35.1) | ||||
|
| ||||||||
| <25,000 | 203 (47.9) | .02 | 93 (55.9) | .48 | 105 (24.6) | <.001 | 63 (37.9) | .14 |
| 25,000–49,999 | 554 (48.9) | 148 (61.0) | 183 (16.1) | 96 (39.8) | ||||
| 50,000–74,999 | 575 (54.2) | 171 (60.4) | 184 (17.3) | 101 (35.6) | ||||
| ≥75,000 | 439 (56.2) | 183 (70.1) | 98 (12.6) | 140 (53.5) | ||||
|
| ||||||||
| Less than high school diploma | 122 (39.6) | <.001 | 162 (62.6) | .48 | 49 (15.9) | .21 | 128 (49.4) | .05 |
| High school graduate | 408 (42.8) | 144 (54.9) | 143 (14.8) | 81 (30.9) | ||||
| Some college | 506 (54.8) | 155 (64.1) | 178 (19.2) | 89 (36.6) | ||||
| College diploma or more | 736 (60.6) | 135 (70.0) | 201 (16.5) | 103 (53.7) | ||||
|
| ||||||||
| Northeast | 285 (49.2) | .33 | 61 (46.0) | .01 | 88 (15.2) | .15 | 45 (34.2) | .43 |
| South | 668 (51.4) | 201 (55.1) | 243 (18.7) | 139 (38.2) | ||||
| Midwest | 388 (54.8) | 66 (71.2) | 119 (16.8) | 40 (43.7) | ||||
| West | 430 (53.0) | 268 (73.4) | 120 (14.7) | 176 (48.2) | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPublic Health Policies and Education · Health Policy Implementation Science · Food Security and Health in Diverse Populations
Introduction
Since the 1960s, community health workers (CHWs) have worked within US public health and community-based organizations to promote health and wellness (1–6). The American Public Health Association defines a CHW as “a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served” (7). This trusting relationship facilitates CHWs’ ability to connect people and communities with health and social services. CHWs can also help improve service delivery to people with different backgrounds. CHWs are known by other titles; Hispanic/Latino communities use the term *promotoras (*or promotores) de salud.
The Centers for Disease Control and Prevention (CDC) has long recognized the contributions of CHWs in clinical and public health practices. Research has demonstrated that CHWs are effective in increasing cancer screening rates for breast, colorectal, and cervical cancers; helping manage chronic conditions, such as diabetes and cardiovascular disease; and helping manage risk factors, such as high blood pressure and cholesterol (8–12). Hispanic or Latino people in the US have a higher incidence and higher death rates of cervical cancer and liver cancer than the general population (13–15). They also have higher rates of other chronic diseases such as diabetes and hypertension compared with other demographic groups (13,16). CHWs promote health and wellness by addressing nonmedical factors that affect health (6,12,17–21) and are increasingly being engaged to address these challenges in various settings and among various populations (22).
Recognition of CHWs’ contributions to improving health has prompted several large national workforce studies in the last 3 decades (1,23–26). The CHW field now has information about the role of CHWs in the workforce, their demographic characteristics, and their employment characteristics, such as the various agencies where they work (3,5). Also, a recent study of primary care providers found that just over half of providers surveyed had worked with a CHW (27); however, no national studies, to our knowledge, describe the public’s familiarity with CHWs. We used national-level surveys to examine and describe the public’s familiarity and interactions with CHWs, including settings (eg, health care, community) where people encountered CHWs and what services CHWs provided. Understanding how the public interacts with CHWs can help future efforts to educate the public and incorporate CHWs in public health programs.
Methods
We analyzed data from the 2022 Porter Novelli FallStyles and Estilos surveys, online national market research surveys fielded from September 1 through September 24, 2022 (FallStyles) and September 29 through November 25, 2022 (Estilos) (28). FallStyles was fielded in English to the general public. Estilos was fielded to a respondent panel of people who identified as Hispanic or Latino and was offered primarily in Spanish but also in English, based on respondent preference. The surveys included 4 questions related to CHWs. These questions were initially written in English for FallStyles and then translated into Spanish for Estilos and further reviewed by a native Spanish speaker for accuracy. Data did not include identifiable information. This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy.
Survey respondents
FallStyles is part of the Porter Novelli ConsumerStyles surveys conducted via the Ipsos Knowledge Panel, an online panel designed to be representative of the noninstitutionalized US population. Recruitment and other methodologic details are available for FallStyles (https://styles.porternovelli.com/consumer-youthstyles) and Estilos (https://styles.porternovelli.com/estilos). FallStyles respondents were recruited from a sample of 4,514 panelists aged 18 years or older who completed the SpringStyles survey. A total of 3,526 adults completed the FallStyles survey, for a participation rate of 78.1%. The unweighted demographic profile of FallStyles respondents was similar to the profile of SpringStyles respondents, with the exception of household size, in which more FallStyles respondents were from households with 2 or fewer people.
Estilos is an annual web-based survey administered by Offerwise through its QueOpinas panel, the largest online panel of Hispanic people in the US, with more than 220,000 active panelists. QueOpinas recruits panels via English-language and Spanish-language network television. Estilos respondents were recruited from a sample of 2,884 panelists aged 18 years or older, and participation was capped at 1,000 participants.
Data collection
The CHW-related questions included questions about familiarity with CHWs, settings in which respondents met with CHWs, and activities with which CHWs helped respondents (Appendix). Questions about settings and activities were derived from previous literature defining CHW roles and core competencies (1,5).
Variables
Familiarity with CHWs. Respondents were provided a standard definition of a CHW and asked, “Prior to this survey, how familiar were you with what CHWs do?” Response options were on a 5-point scale (from 1 = extremely familiar to 5 = not at all familiar). We grouped respondents who selected responses 1, 2, 3, or 4 into the “familiar” category. Those who selected a response of 5 were categorized as “not familiar.”
Settings. Respondents were asked in what settings (if any) CHWs had helped them. Response options were the following: clinic or hospital, social service system, community or place of worship, at home, at a job, no involvement, or “I am a CHW.” Respondents who indicated no involvement with CHWs or identified as CHWs were not asked about receiving CHW services.
Services. Respondents who had been helped by a CHW were asked a series of yes/no/don’t know items about how a CHW helped within the health care system (eg, get the medical care I needed, enroll in health insurance) and the types of social services CHWs helped people obtain (eg, housing/shelter, food, employment).
Data analysis
For both surveys, we calculated descriptive statistics overall and by level of familiarity with CHWs and interactions with CHWs, comparing respondents by demographic characteristics. We used χ^2^ tests for statistical comparisons. We analyzed each survey separately, given differences in recruitment strategies and panel designs; however, we tabulated findings from both surveys together for nonstatistical comparisons. We used SAS 9.4 (SAS Institute, Inc) to conduct analyses. P values ≤.05 were considered significant. We incorporated into both analyses survey weights designed to weight the data to match proportions of either the US Current Population Survey or the American Community Survey. We used SAS survey procedures for analysis, producing weighted counts and percentages. We excluded from the analysis 43 FallStyles and 45 Estilos respondents (unweighted count) who reported being CHWs themselves. Fifty-three FallStyles respondents did not respond to the question about being helped by a CHW, leaving an unweighted count of 3,430 respondents remaining in the analysis. All results are reported as weighted counts.
Results
Among FallStyles respondents, 65.4% identified as White, 13.0% as Hispanic or Latino, and 11.8% as Black (Table 1). Nearly one-third (31.8%) were aged 60 years or older, and 26.4% were aged 30 to 44 years. Fifty-one percent of respondents were female, 35.7% had at least a college diploma, 28.2% had only a high school diploma, and 45.9% reported a household income less than 50,000, 27.1% had less than a high school diploma, and 27.4% had only a high school diploma.
Of FallStyles respondents, 52.1% were familiar with CHWs, and 16.7% reported having interacted with a CHW (Table 2). By age, rates of familiarity with CHWs were highest among FallStyles respondents aged 60 years or older and lowest among respondents aged 18 to 29 years (54.1% vs 45.0%; P = .01). FallStyles respondents reporting household income levels of 25,000 (56.2% vs 47.9%; P = .02). Conversely, FallStyles respondents in the lowest income category, compared with respondents in the highest income category, more frequently reported interactions with CHWs (24.6% vs 12.6%; P < .001). Familiarity with CHWs was greater among FallStyles respondents reporting a college diploma or more than among those reporting less than a high school diploma (60.6% vs 39.6%; P < .001).
Of Estilos respondents, 62.4% were familiar with CHWs, and 42.0% reported having interacted with a CHW. The percentage of Estilos respondents who interacted with CHWs was higher among respondents with a college diploma or more than those with less than a high school diploma (53.7% vs 49.4%, P = .05). The only other significant difference in demographic characteristics among Estilos respondents was that those residing in the West and Midwest reported more familiarity with CHWs than respondents in other regions (range across all regions, 46.0%–73.4%; P = .01).
Settings in which respondents had interactions with CHWs
The majority of both FallStyles and Estilos respondents who indicated they had been helped by a CHW reported that their interactions occurred in health care settings (60.8% and 64.2%, respectively) (Figure 1). Less than a quarter of respondents who had been helped by a CHW reported interactions in their community or place of worship (21% FallStyles; 22.2% Estilos).
Settings in which community health workers were encountered, US, 2022. Data were obtained from respondents in 2 national surveys: FallStyles, conducted in English in September 2022 among the general public, and Estilos, conducted among a panel of people who identified as Hispanic or Latino and offered primarily in Spanish, in September through November 2022. Data are from a subset of respondents who indicated they had been helped by a community health worker (FallStyles, n = 570; Estilos n = 401).
Activities in which CHWs assisted respondents
Among survey respondents indicating CHW involvement, respondents from both surveys reported that CHWs helped them with various activities across health-related and social service–related issues; however, some activities were cross-cutting. For example, 15.7% of FallStyles respondents reported that CHWs helped them communicate across cultures to better access health and social services, 16.9% reported CHWs helped them communicate their needs with health care or social service providers, and 25.4% reported CHWs helped them communicate their community’s needs (Figure 2). Nearly half (45.1%) of Estilos respondents that reported CHWs helped them communicate across cultures to better access health and social services and communicate needs with health care or social service providers. One-third (32.9%) of Estilos respondents reported CHWs helped them communicate their community’s needs.
Activities in which community health workers assisted survey respondents, US, 2022. Data were obtained from 2 national surveys: FallStyles, conducted in English in September 2022 among the general public and Estilos, conducted among a panel of people who identified as Hispanic or Latino in September through November 2022. Data are from a subset of respondents who indicated they had been helped by a community health worker. For the question on social services, FallStyles n = 565 and Estilos n = 401. For the question on health-related and cross-cutting activities, FallStyles n = 570, and Estilos n = 401. For social services–related items, only items for which at least 10% of either group (FallStyles or Estilos) indicated being helped with are shown.
FallStyles respondents indicating they had been helped by CHWs reported that CHWs helped them obtain medical care (45.1%), increase physical activity (24.9%), and manage chronic health conditions (24.1%) (Figure 2). Fewer FallStyles respondents reported that CHWs helped them quit smoking (6.6%), obtain substance use treatment (5.3%), obtain home visits during pregnancy and/or help with parenting (4.8%), or manage cancer (4.6%). Most Estilos respondents indicating they had been helped by CHWs reported that CHWs helped them obtain medical care (59.8%), obtain linguistically and culturally concordant health information (57.0%), increase physical activity (52.7%), and enroll in health insurance (46.9%). Fewer Estilos respondents reported receiving assistance from CHWs to obtain home visits during pregnancy or help with parenting (16.1%) or manage cancer (10.8%).
FallStyles respondents indicating they had been helped by a CHW reported that CHWs helped them obtain connections with agencies (12.2%), food (11.4%), and elder care (7.5%) (Figure 2). Estilos respondents indicating they had been helped by a CHW reported that CHWs helped them obtain connections with agencies (25.0%), food (23.8%), and transportation (18.7%).
Discussion
We analyzed data from 2 nationally derived surveys to conduct the first, to our knowledge, large-scale assessment of familiarity with CHWs among the general public (FallStyles) and the Hispanic or Latino population (Estilos). Overall, we found that FallStyles respondents with higher incomes and greater education were more familiar with CHWs, while those with lower incomes more often reported interacting with CHWs.
Our study has several implications. Although the surveys are not directly comparable, the finding that a higher percentage of Estilos respondents than FallStyles reported being familiar with and having received support from a CHW suggest that CHWs have established inroads into reaching Hispanic or Latino populations. The finding that Estilos respondents interacted with CHWs at higher rates than FallStyles respondents across all response categories may indicate that Hispanic or Latino populations need more support to navigate multiple complex health and social needs and may lack trust in the health care system (29).
Overall, our findings suggest that public health programs focused on preventing chronic diseases may consider engaging CHWs to provide outreach and education. For example, CHWs may be helpful in promoting cancer screening among Hispanic or Latino populations, since Hispanic adults have been found to be less likely than non-Hispanic adults to be up-to-date with cervical and colorectal cancer screening (30). CHWs have long been part of outreach and recruitment efforts in CDC’s cancer prevention and control programs as an evidence-based strategy (8,9) to help individuals across the cancer continuum, from screening to treatment referral to long-term survivorship.
Our findings align with recent studies of the CHW workforce that pointed to a need for greater public awareness and understanding of CHWs’ multifaceted roles, scope, and locations of employment (26,31). Although FallStyles and Estilos respondents most frequently identified receiving CHW support in health care settings, a recent survey of US-based CHWs found that most CHW work took place in community-based settings, rather than clinical settings (26). Further studies could help explain this discrepancy. Even when individuals are familiar with and benefit from community-level public health activities, they may not realize that a CHW, as opposed to another professional, performed the work. Greater public awareness of CHWs’ community-level roles could help ensure that individuals seek CHW support for social and community needs, rather than strictly medical needs.
Additionally, education for health providers about CHWs’ roles could support improved interprofessional collaboration and health care team integration. A recent survey of primary care providers revealed that those who had not previously worked with CHWs believed having additional information about CHW roles and functions would be helpful (27). Even providers who were familiar with CHWs believed lack of information about how CHWs can collaborate with other health professionals was a barrier to team integration (27). Ensuring that health care providers understand CHWs’ scope of practice, the extent of their professional training, and their unique skills may promote uptake of CHW services and alleviate common misconceptions about CHWs’ activities.
Strengths and limitations
This study has several strengths. To our knowledge, this is the first study using nationally derived samples of individuals to understand their familiarity and interactions with CHWs. The Estilos survey was administered to Hispanic/Latino adults, with the option of responding in either Spanish or English, allowing for an examination of a population with health disparities across several chronic conditions. In addition, the FallStyles survey had a high participation rate and a relatively large sample size.
This study has several limitations. First, self-reported data can be subject to recall bias and social desirability bias. Second, we could not capture all possible places that an individual can encounter a CHW (eg, health departments) because free text is not a feature of Porter Novelli surveys. Third, although FallStyles and Estilos surveys are weighted to match the US Census Bureau’s proportions, people who agree to participate in online survey panels could be systematically different from others, so our findings may not be generalizable given that population-based probability sampling methods were not used. Finally, because of differences in survey methodology and population sampled between FallStyles and Estilos, we could not perform statistical tests to assess differences between the 2 groups of survey respondents. Despite these limitations, this study contributes to our understanding of the degree to which the general public and Hispanic or Latino people are familiar with and how they interact with CHWs.
Conclusion
A strategic focus on including CHWs in public health awareness campaigns, coupled with the reach of public health programs already engaging CHWs, could enhance the public’s knowledge of the CHW workforce and ultimately increase public engagement with CHWs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wiggins N , Borbon IA . Core roles and competencies of community health workers. In: Final Report of the National Community Health Advisor Study. Annie E. Casey Foundation; 1998.
- 2Rosenthal EL . The evolution of the CHW field in the United States. In: Berthold T, Avila A, Miller J, eds. Foundations for Community Health Workers. Vol 35. John Wiley & Sons; 2009:23–44.
- 3Rosenthal EL , Wiggins N , Ingram M , Mayfield-Johnson S , De Zapien JG . Community health workers then and now: an overview of national studies aimed at defining the field. J Ambul Care Manage. 2011;34(3):247–259. 10.1097/JAC.0b 013e 31821 c 64d 7 21673523 · doi ↗ · pubmed ↗
- 4Brownstein JN , Hirsch GR , Rosenthal EL , Rush CH . Community health workers “101” for primary care providers and other stakeholders in health care systems. J Ambul Care Manage. 2011;34(3):210–220. 10.1097/JAC.0b 013e 31821 c 645d 21673520 · doi ↗ · pubmed ↗
- 5Rosenthal ELMP , St. John J , Fox D , Holderby-Fox LR , Redondo F , Hirsch G , . The Community Health Worker Core Consensus (C 3) Project reports and website. 2014–2022. Accessed July 21, 2023. https://www.c 3project.org/roles-competencies
- 6Kangovi S , Grande D , Trinh-Shevrin C . From rhetoric to reality—community health workers in post-reform U.S. health care. N Engl J Med. 2015;372(24):2277–2279. 10.1056/NEJ Mp 1502569 26061832 PMC 4689134 · doi ↗ · pubmed ↗
- 7American Public Health Association. Support for community health workers to increase health access and to reduce health inequities. November 10, 2009. Accessed July 3, 2023. https://www.apha.org/Policies-and-Advocacy/Public-Health-Policy-Statements/Policy-Database/2014/07/09/14/19/Support-for-Community-Health-Workers-to-Increase-Health-Access-and-to-Reduce-Health-Inequities
- 8Guide to Community Preventive Services. Cancer screening: interventions engaging community health workers — breast cancer. March 10, 2020. Accessed March 31, 2023. https://www.thecommunityguide.org/findings/cancer-screening-interventions-engaging-community-health-workers-breast-cancer.html