Interplay Between Childhood Maltreatment, Subclinical Post‐Traumatic Stress Symptoms, and IQ: Findings From the EU‐GEI Multicentre Case–Control Study
Lucia Sideli, Monica Aas, Luis Alameda, Giulia Trotta, Daniele La Barbera, Caterina La Cascia, Laura Ferraro, Eva Velthorst, Giada Tripoli, Adriano Schimmenti, Andrea Fontana, Diego Quattrone, Charlotte Gayer‐Anderson, Victoria Rodriguez, Edoardo Spinazzola, Simona Stilo

TL;DR
The study explores how childhood maltreatment and post-traumatic stress symptoms affect IQ in people with psychosis and controls.
Contribution
It reveals a unique interaction between maltreatment and PTSS impacting IQ only in psychosis patients.
Findings
PTSS were linked to lower IQ in community controls but not in psychosis patients.
An interaction between PTSS and childhood maltreatment affected IQ in first-episode psychosis patients.
No such interaction was found in community controls.
Abstract
Evidence suggests that childhood maltreatment affects cognitive performance in both patients with psychosis and community controls. However, the interplay between childhood maltreatment, post‐traumatic stress symptoms (PTSS), and intelligence has not been investigated. This study investigated the relationship between childhood maltreatment, subclinical PTSS, and intelligence among patients with first‐episode psychosis (FEP) and community controls. Patients with FEP (N = 602) and controls (N = 853) from the EU‐GEI study were assessed for childhood maltreatment, PTSS, and intelligence quotient (IQ). PTSS were associated with lower IQ among community controls but not among patients with FEP. In the FEP group, an interaction (p = 0.044) between PTSS and childhood maltreatment on IQ was found, such that the association between PTSS and lower IQ was only present among those exposed to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
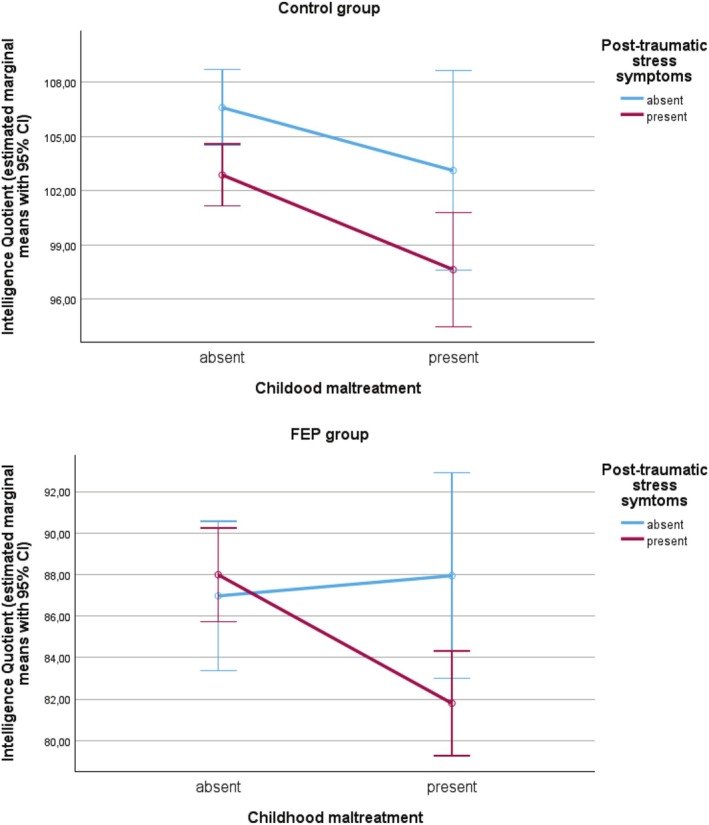 FIGURE 1
FIGURE 1| Crude model | Adjusted model | |||||
|---|---|---|---|---|---|---|
|
| 95% CI |
|
| 95% CI |
| |
| Unstandardized models | ||||||
| Controls |
|
| ||||
| Childhood maltreatment | −3.48 | −9.38; 2.43 | 0.248 | −2.50 | −7.71; 2.70 | 0.345 |
| Subclinical PTSS |
|
|
|
|
|
|
| Childhood maltreatment × subclinical PTSS | −1.76 | −8.67; 5.15 | 0.617 | 0.68 | −5.36; 6.71 | 0.826 |
| FEP patients |
|
| ||||
| Childhood maltreatment | 0.97 | −5.15; 7.09 | 0.755 | 2.78 | −3.03; 8.59 | 0.348 |
| Subclinical PTSS | 1.02 | −3.22; 5.26 | 0.637 | −0.96 | −4.98; 3.07 | 0.641 |
| Childhood maltreatment × subclinical PTSS |
|
|
|
| − |
|
| Standardised models | ||||||
| Controls |
|
| ||||
| Childhood maltreatment | −0.19 | −0.52; 0.14 | 0.248 | −0.14 | −0.43; 0.15 | 0.345 |
| Subclinical PTSS |
|
|
|
|
|
|
| Childhood maltreatment × subclinical PTSS | −0.10 | −0.48; 0.29 | 0.617 | 0.04 | −0.30; 0.37 | 0.826 |
| FEP patients |
|
| ||||
| Childhood maltreatment | 0.05 | −0.28; 0.39 | 0.755 | 0.15 | −0.17; 0.47 | 0.348 |
| Subclinical PTSS | 0.06 | −0.18; 0.29 | 0.637 | −0.05 | −0.27; 0.17 | 0.641 |
| Childhood maltreatment × subclinical PTSS |
|
|
|
|
|
|
- —European Community’s Seventh Framework Programme
- —São Paulo Research Foundation10.13039/501100001807
- —Medical Research Council10.13039/501100000265
- —Fondation Adrian et Simone Frutiger
- —Carigest SA10.13039/100031252
- —Spanish Ministry of Science, Innovation and Universities
- —Instituto de Salud Carlos III (ISCIII)10.13039/501100004587
- —European Union10.13039/501100000780
- —European Regional Development Fund10.13039/501100008530
- —European Union NextGenerationEU
- —CIBERSAM10.13039/501100006751
- —Government of the Community of Madrid
- —European Union Structural Funds
- —European Union Seventh Framework Program
- —European Union10.13039/501100000780
- —Horizon Europe10.13039/100018693
- —National Institute of Mental Health10.13039/100000025
- —Fundación Familia Alonso
- —Fundación Alicia Koplowitz10.13039/100008062
- —Economic and Social Research Council (ESRC) Centre for Society and Mental Health at King’s College London10.13039/501100000269
- —Lord Leverhulme’s Charitable Trust
- —Velvet Foundation
- —Dutch Research Council10.13039/501100003246
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Abuse and Trauma · Migration, Health and Trauma · Posttraumatic Stress Disorder Research
Introduction
1
Accumulating research has consistently demonstrated that childhood maltreatment is associated with psychosis, but the mediators and moderators of this association are still unclear and suggest that cognition and post‐traumatic stress symptoms (PTSS) may play a role (Alameda et al. 2020; Sideli et al. 2020).
Findings on both general and clinical populations indicate that childhood maltreatment may impair cognitive performance (Rosa et al. 2023; Vargas et al. 2019), which is particularly detrimental for people suffering from psychosis as it reduces social and occupational functioning (Fares‐Otero et al. 2023; Montaner‐Ferrer et al. 2023). However, the association between childhood maltreatment and cognition is weaker among people with psychosis compared with controls (Dauvermann and Donohoe 2019; Vargas et al. 2019), arguably because of floor effects (Sideli et al. 2014; van Os et al. 2017). Furthermore, the impact of childhood maltreatment on cognition may vary by type of traumatic exposure. We previously found that both childhood abuse and neglect were associated with lower Intelligence Quotient (IQ) among controls without a psychotic disorder, whereas only childhood neglect was associated with lower IQ among people with first‐episode psychosis (FEP) (Sideli et al. 2022, 2023).
People with psychosis also report a greater prevalence of Post Traumatic Stress Disorders (PTSD) (Seong et al. 2023; Seow et al. 2016) and more frequent subclinical PTSS (Berry et al. 2013), that is PTSD symptoms not satisfying the clinical threshold for PTSD, according to established criteria (American Psychiatric Association 2022; World Health Organization 2019). PTSD and PTSS in psychosis may arise from childhood maltreatment (Bendall et al. 2008; Schäfer and Fisher 2011), adult life events (Beards et al. 2013; D'Andrea et al. 2023; van Zelst 2008) and the experience of psychosis itself (Buswell et al. 2021). Some community studies suggest that PTSS may increase the negative impact of childhood maltreatment on cognition (Burri et al. 2013; De Bellis et al. 2009, 2013). However, among people with psychosis, the association between PTSS and cognitive impairment has not been consistently replicated (Duke et al. 2010; Goodman et al. 2007; Peleikis et al. 2013). Furthermore, to the best of our knowledge, no study has examined the interplay between childhood maltreatment, PTSS and cognition in psychosis.
Using data from a large multi‐national study of psychosis, we sought to investigate the relationship between childhood maltreatment, subclinical PTSS and IQ among FEP patients and community controls. We hypothesised that: (1) compared to community controls, FEP patients would report a greater prevalence of PTSS; (2) PTSS would be associated with lower IQ in both patients and controls; and (3) PTSS would moderate the effect of childhood maltreatment on IQ in both groups, such that the association between exposure to maltreatment and lower IQ would be stronger among those with PTSS.
Methods
2
Sample
2.1
People with FEP and community controls participated in the EU‐GEI study, a multi‐centre incidence, case–control study carried out between May 2010 and April 2015 in five European countries and Brazil. The study was approved by the local Institutional Review Board and carried out in line with International Ethical Standards. Information about inclusion and exclusion criteria and sampling strategies was previously described (Gayer‐Anderson et al. 2020; van Os et al. 2008). The current study was conducted on a subset of 602 FEP and 853 controls with complete information about childhood maltreatment, PTSS and IQ (see Table S1 and Supporting Information 1).
Measures
2.2
Childhood maltreatment prior to age 18 was assessed using the Childhood Trauma Questionnaire (Bernstein et al. 1997). An overall ‘childhood maltreatment’ score, and separate ‘childhood abuse’ and ‘childhood neglect’ scores were calculated from the mean score of the respective items (rated 1 = never to 5 = very often). Consistent with previous studies (Sideli et al. 2022; van Os et al. 2017), three dichotomous variables for overall childhood maltreatment, abuse and neglect were then calculated using the 80th percentile of the control group as a cut‐off value (equal to 1.64, 1.40 and 2.00, respectively).
Presence of any PTSS in the week prior to study assessment was assessed in participants reporting any traumatic experience using the Impact of Events Scale‐6 (Thoresen et al. 2010) with two additional items to capture persistent re‐experiencing (‘I had dreams about it’ and ‘Pictures about it popped into my mind’) from the IES‐R (Weiss and Marmar 1997) (see Supporting Information). Items were rated on a 4‐point scale (0 = not at all to 4 = extremely), with total scores ranging from 0 to 32 (FEP: α = 0.86; controls: α = 0.89). To capture subclinical PTSS, we dichotomised the total score (0 = absent, 1+ = present).
IQ was assessed using an abbreviated version of the Wechsler Adult Intelligence Scale (WAIS‐III) (Blyler et al. 2000), including selected items of the following subtests: digit symbol coding (a measure of processing speed), arithmetic (working memory), block design (visuospatial processing), and information (verbal knowledge) (Velthorst et al. 2013, 2021).
Information about socio‐demographic characteristics (i.e., sex, age, country, education and ethnicity), lifetime cannabis use and current use of antipsychotics was collected using the MRC sociodemographic questionnaire (Mallet 1997), Cannabis Experience Questionnaire (Di Forti et al. 2014), and patients' clinical records.
Analyses
2.3
General linear regression models stratified for patients and controls were used to investigate the multiplicative interaction between childhood maltreatment and PTSS (independent dichotomous variables) on IQ (dependent continuous variable). Analyses were adjusted for the following covariates: sex, age, ethnicity (white vs. non‐white), education (from no education to post‐degree), study country, lifetime cannabis use (yes vs. no) and, only in the FEP group, current use of antipsychotics (none vs. one vs. > 1 antipsychotic medications). Results are reported as regression coefficients (B) and standardised betas (β). Analyses were carried out using SPSS v27.0.
Results
3
Associations Between Childhood Maltreatment, PTSS and IQ
3.1
Average IQ was significantly lower among FEP patients and prevalence of childhood maltreatment and PTSS were higher (Table S2). In both patients and controls, childhood maltreatment was associated with PTSS. In both groups, childhood maltreatment was associated with lower IQ, but PTSS was associated with lower IQ only in the control group (Table S3).
Interaction Between Childhood Maltreatment × PTSS on IQ
3.2
An interaction between childhood maltreatment and PTSS on IQ was evident in the FEP group (Table 1 and Figure 1). Among patients exposed to childhood maltreatment, a lower IQ was found in those where PTSS was present (M = 81.80, SD = 15.87) versus absent (M = 87.94, SD = 21.97). No association was found in the corresponding unexposed group (PTSS+ M = 86.97, SD = 19.30 vs. PTSS− M = 87.99, SD = 18.62).
Interaction between childhood maltreatment and subclinical post‐traumatic stress symptoms. CI, confidence intervals; FEP, first‐episode psychosis.
By contrast, among community controls, PTSS was associated with lower IQ, without interaction with childhood maltreatment (Table 1; Figure 1). In this group, the association was evident both in those exposed to childhood maltreatment (PTSS+ M = 97.64, SD = 17.05 vs. PTSS− M = 103.13, SD = 19.39) and in those unexposed (PTSS+ M = 102.88, SD = 17.53 vs. PTSS− M = 106.60, SD = 18.24).
Effect of Specific Types of Childhood Adversities
3.3
No childhood abuse × PTSS interaction on IQ was observed in either the FEP or control groups. Only in the FEP group was a childhood neglect × PTSS interaction detected (unadj. B = −8.82, p = 0.013; adj. B = −7.82, p = 0.018) (Tables S4 and S5).
In the control group there was an association between PTSS and lower IQ independent of and without interaction with childhood abuse (unadj. B = −3.36, p = 0.015; adj. B = −2.27, p = 0.069) and childhood neglect (unadj. B = −4.20, p = 0.002; adj. B = −2.87 p = 0.021). The findings were consistent when a measure of moderate to extreme PTSS symptoms was used (Supporting Information: Sensitivity analyses).
Discussion
4
This study found that subclinical PTSS were associated with lower IQ among community controls but not among patients with FEP. In the FEP group, an interaction between PTSS and childhood maltreatment was found, such that the association between PTSS and lower IQ was only present among those maltreated in childhood. No interaction was found among controls. The findings suggest that PTSS might be differently related to IQ among FEP patients and controls. In the FEP group, the lack of association between PTSS and IQ is consistent with some of the previous studies on PTSD and cognition (Duke et al. 2010; Peleikis et al. 2013). However, in this group, PTSS symptoms might modify the impact of childhood maltreatment on intelligence (Aas et al. 2014; Dauvermann and Donohoe 2019). Furthermore, among controls, the impact of PTSS on IQ seemed partially independent from the exposure to childhood maltreatment (Burri et al. 2013).
We found that the moderating effect of PTSS on IQ was only evident for neglect. Literature has suggested that, among people with psychosis, the impact of neglect on IQ might be more consistent than that of abuse (Aas et al. 2012; Garcia et al. 2016; Li et al. 2017; Mørkved et al. 2020). In line with studies revealing an association between childhood neglect, PTSS, and greater symptom severity in psychotic disorders (Cakir et al. 2016; Vogel et al. 2011), we speculate that PTSS might increase the detrimental impact of childhood neglect on cognition both directly, through memory impairment, and indirectly by amplifying emotion dysregulation (Liu et al. 2020) which in turn affects cognitive performance (Romano et al. 2015).
The findings of this study should be interpreted considering some limitations. First, consistent with previous literature (Vargas et al. 2019), childhood maltreatment could be considered to contribute to the lower IQ observed in FEP patients, which is affected by numerous factors, including genetic liability, developmental abnormalities, and social disadvantage. Second, although childhood maltreatment and PTSS were assessed with reference to non‐overlapping timeframes (i.e., up to age 18 for childhood maltreatment; over the past 7 days for PTSS), the retrospective study design prevents any inference about temporal order. Third, the sample size and missing data might have adversely affected the study's power to detect interactions. Fourth, the high prevalence of PTSS among FEP patients and their particularly low mean IQ might have obscured any potential association between PTSS and IQ in this group. In addition, the association of childhood maltreatment with lower IQ may involve other psychopathological factors (e.g., depression) not assessed here. Fifth, we were unable to include the PTSS score as a continuous variable in analyses as it was extremely skewed, thus limiting the conclusions that can be drawn. Finally, mediation analyses were not performed since we could not rule out that PTSS resulted from later life events, or the psychosis experience itself.
Nonetheless, these findings confirm the importance of adequately assessing (Carr et al. 2018; Redmond et al. 2025) and treating PTSD and subclinical PTSS among people with psychosis (Schäfer and Fisher 2011; Swan et al. 2017) and suggest an interplay between childhood maltreatment and PTSS on cognition (Christy et al. 2023; Rodriguez et al. 2021). If the results are replicated in larger, longitudinal samples, they could indicate the need for cognitive rehabilitation for FEP patients with childhood maltreatment histories and PTSS.
Supporting information
Data S1: eip70079‐sup‐0001‐Supinfo.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aas, M. , P. Dazzan , V. Mondelli , I. Melle , R. M. Murray , and C. M. Pariante . 2014. “A Systematic Review of Cognitive Function in First‐Episode Psychosis, Including a Discussion on Childhood Trauma, Stress, and Inflammation.” Frontiers in Psychiatry 4: 182. 10.3389/fpsyt.2013.00182.24409157 PMC 3884147 · doi ↗ · pubmed ↗
- 2Aas, M. , N. E. Steen , I. Agartz , et al. 2012. “Is Cognitive Impairment Following Early Life Stress in Severe Mental Disorders Based on Specific or General Cognitive Functioning?” Psychiatry Research 198, no. 3: 495–500. 10.1016/j.psychres.2011.12.045.22472845 · doi ↗ · pubmed ↗
- 3Alameda, L. , V. Rodriguez , E. Carr , et al. 2020. “A Systematic Review on Mediators Between Adversity and Psychosis: Potential Targets for Treatment.” Psychological Medicine 50, no. 12: 1966–1976. 10.1017/S 0033291720002421.32744193 · doi ↗ · pubmed ↗
- 4American Psychiatric Association . 2022. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association. 10.1176/appi.books.9780890425787. · doi ↗
- 5Beards, S. , C. Gayer‐Anderson , S. Borges , M. E. Dewey , H. L. Fisher , and C. Morgan . 2013. “Life Events and Psychosis: A Review and Meta‐Analysis.” Schizophrenia Bulletin 39, no. 4: 740–747. 10.1093/schbul/sbt 065.23671196 PMC 3686461 · doi ↗ · pubmed ↗
- 6Bendall, S. , H. J. Jackson , C. A. Hulbert , and P. D. Mc Gorry . 2008. “Childhood Trauma and Psychotic Disorders: A Systematic, Critical Review of the Evidence.” Schizophrenia Bulletin 34, no. 3: 568–579.18003630 10.1093/schbul/sbm 121PMC 2632421 · doi ↗ · pubmed ↗
- 7Bernstein, D. P. , T. Ahluvalia , D. Pogge , and L. Handelsman . 1997. “Validity of the Childhood Trauma Questionnaire in an Adolescent Psychiatric Population.” Journal of the American Academy of Child and Adolescent Psychiatry 36, no. 3: 340–348. 10.1097/00004583-199703000-00012.9055514 · doi ↗ · pubmed ↗
- 8Berry, K. , S. Ford , L. Jellicoe‐Jones , and G. Haddock . 2013. “PTSD Symptoms Associated With the Experiences of Psychosis and Hospitalisation: A Review of the Literature.” Clinical Psychology Review 33, no. 4: 526–538. 10.1016/j.cpr.2013.01.011.23500156 · doi ↗ · pubmed ↗