Carvedilol vs. Metoprolol Effectiveness in Patients With Left Ventricular Assist Devices: A TriNetX Analysis
Karldon I Nwaezeapu, Godbless Ajenaghughrure, Ekow Essien, Smith Frimpong, Chukwuemeka C Aghasili, God-dowell O Odukudu, Henna Qadri, Yash B Patel, Andrew Ndakotsu, Taraneh Zamani

TL;DR
This study compares carvedilol and metoprolol in patients with heart pumps, finding that carvedilol reduces deaths and some complications, though it increases heart failure flare-ups and kidney issues.
Contribution
The study provides new comparative effectiveness data for beta-blockers in patients with left ventricular assist devices using a large federated health network.
Findings
Carvedilol was associated with lower all-cause mortality compared to metoprolol in LVAD patients.
Carvedilol reduced cardiac arrest, cardiogenic shock, sepsis, and atrial fibrillation but increased heart failure exacerbation and acute kidney injury.
Abstract
Background: Beta-blockers are a cornerstone of heart failure management, but comparative effectiveness data for different beta-blockers in patients with mechanical circulatory support remain limited. This study aimed to compare clinical outcomes between carvedilol and metoprolol in patients with left ventricular assist devices (LVADs). Methods: We performed a retrospective cohort study using the TriNetX Research Network (Cambridge, MA: TriNetX, LLC), a global federated health research platform providing access to electronic medical records across 104 healthcare organizations. Patients with left ventricular assist devices (ICD-10 code Z95.81) who were prescribed either carvedilol or metoprolol were identified. After propensity score matching for baseline characteristics, including cardiac and non-cardiac comorbidities, cohorts of 5,166 patients each receiving carvedilol or metoprolol…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
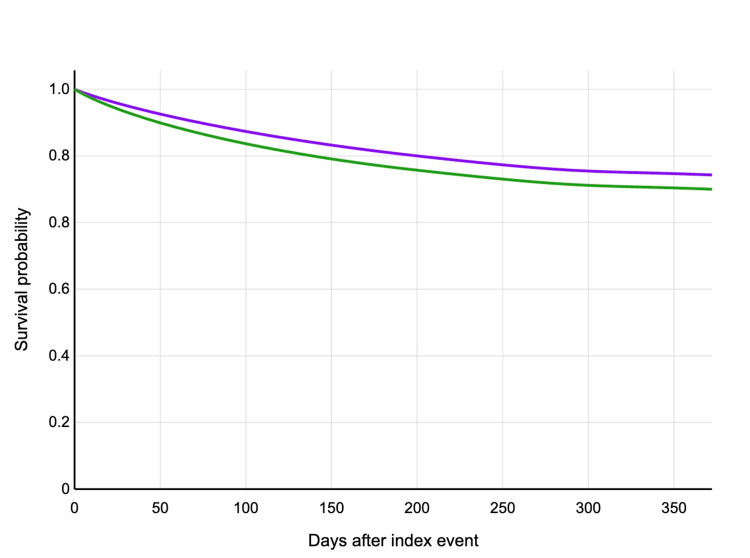 Figure 1
Figure 1| Characteristic | Carvedilol group (n=5,166) | Metoprolol group (n=5,166) | p-Value |
| Cardiac conditions | |||
| Heart failure | 78.8% | 77.5% | 0.105 |
| Atrial fibrillation | 40.6% | 39.7% | 0.356 |
| Dilated cardiomyopathy | 21.1% | 20.5% | 0.452 |
| Other cardiomyopathies | 40.4% | 38.3% | 0.028 |
| Non-cardiac comorbidities | |||
| Hypertension | 59.5% | 56.6% | 0.003 |
| Diabetes mellitus | 41.6% | 40.6% | 0.308 |
| Chronic kidney disease | 16.6% | 15.6% | 0.164 |
| Outcome | Carvedilol group (n=5,166) | Metoprolol group (n=5,166) | Hazard ratio (95% CI) | p-Value |
| Primary outcome | ||||
| All-cause mortality | 795 (15.4%) | 879 (17.0%) | 0.879 (0.799-0.968) | 0.009 |
| Secondary outcomes | ||||
| Heart failure exacerbation | 3,684 (71.3%) | 3,405 (65.9%) | 1.149 (1.097-1.204) | <0.001 |
| Cardiac arrest | 257 (5.0%) | 314 (6.1%) | 0.799 (0.677-0.942) | 0.007 |
| Cardiogenic shock | 915 (17.7%) | 1,084 (21.0%) | 0.817 (0.748-0.892) | <0.001 |
| Sepsis | 457 (8.8%) | 536 (10.4%) | 0.821 (0.724-0.930) | 0.002 |
| Acute kidney injury | 1,645 (31.8%) | 1,454 (28.1%) | 1.132 (1.055-1.214) | 0.001 |
| Atrial fibrillation | 1,411 (27.3%) | 1,584 (30.7%) | 0.850 (0.792-0.914) | <0.001 |
| Ventricular tachycardia | 1,199 (23.2%) | 1,181 (22.9%) | 0.991 (0.915-1.074) | <0.001 |
| Sick sinus syndrome | 446 (8.6%) | 454 (8.8%) | 0.951 (0.834-1.084) | 0.450 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Mechanical Circulatory Support Devices · Cardiac pacing and defibrillation studies
Introduction
Advanced heart failure represents a significant global health burden, with increasing prevalence and high morbidity and mortality rates despite optimal medical therapy [1]. Left ventricular assist devices (LVADs) have become an established therapeutic option for patients with end-stage heart failure, serving as a bridge to transplantation, bridge to recovery, or destination therapy [2]. The expanding use of LVADs has improved survival and quality of life for many patients with advanced heart failure, though complications remain common and medical management continues to evolve [3,4].
Beta-blockers are a cornerstone of heart failure management, with established benefits in reducing mortality and morbidity in patients with reduced ejection fraction [5]. However, the optimal choice of beta-blocker in patients with LVADs remains unclear. While guidelines recommend specific beta-blockers (carvedilol, metoprolol succinate, or bisoprolol) for heart failure patients with reduced ejection fraction, these recommendations are extrapolated from studies in patients without mechanical circulatory support [6,7].
Carvedilol and metoprolol represent two commonly prescribed beta-blockers with distinct pharmacological profiles. Carvedilol is a non-selective beta-blocker with additional alpha-1 blocking and antioxidant properties, while metoprolol is a selective beta-1 adrenergic receptor antagonist [8]. These pharmacological differences could potentially impact clinical outcomes in LVAD patients, who have unique physiological considerations related to continuous-flow hemodynamics and altered neurohormonal activation [9].
Previous studies comparing carvedilol and metoprolol in heart failure patients without LVADs have shown mixed results. The Carvedilol Or Metoprolol European Trial (COMET) trial demonstrated superior survival benefits with carvedilol compared to immediate-release metoprolol tartrate [10], while other studies comparing carvedilol to extended-release metoprolol succinate have shown comparable effects on left ventricular function and clinical outcomes [11]. However, data specifically examining beta-blocker selection in LVAD recipients remain scarce.
LVAD patients face unique challenges, including altered hemodynamics, a high risk of arrhythmias, and susceptibility to right ventricular dysfunction, which may influence beta-blocker response. Additionally, the risk profiles for complications such as atrial fibrillation, ventricular tachycardia, and cardiogenic shock may differ from those of heart failure patients without mechanical support [12,13].
Given the limited comparative effectiveness data for different beta-blockers in LVAD recipients, we conducted this study to compare clinical outcomes between carvedilol and metoprolol in this unique population. Understanding the optimal beta-blocker choice for LVAD patients may help improve outcomes in this high-risk group and inform future clinical guidelines.
Materials and methods
Data source
This study utilized data from the TriNetX Research Network (Cambridge, MA: TriNetX, LLC), a global federated health research platform providing access to electronic medical records (diagnoses, procedures, medications, laboratory values, and genomic information) across 104 healthcare organizations. The platform allows for real-time queries and robust analysis of patient data while maintaining privacy and security through de-identification. For this study, we analyzed data from the Research Network of the TriNetX platform.
Study population
We identified patients with left ventricular assist devices using the International Classification of Diseases, 10th Revision (ICD-10) code Z95.81 (presence of heart assist device). From this population, we selected patients who were prescribed either carvedilol or metoprolol after LVAD implantation.
Participants were eligible if they were aged 18 years or older at the time of LVAD implantation, had documented LVAD placement, and were prescribed either carvedilol or metoprolol after implantation with at least one year of follow-up data available. Participants were excluded if they used both carvedilol and metoprolol concurrently, underwent heart transplantation before the index date, had documented contraindications to beta-blocker therapy, were pregnant during the study period, or had incomplete clinical data.
Exposure and outcomes
The primary exposure of interest was the type of beta-blocker prescribed (carvedilol vs. metoprolol) after LVAD implantation. The primary outcome was all-cause mortality within one year after the index date. Secondary outcomes included several events within one year after the index date. These comprised heart failure exacerbation (requiring hospitalization or emergency department visit), cardiac arrest, cardiogenic shock, sepsis, acute kidney injury, atrial fibrillation (new-onset or recurrent), ventricular tachycardia, and sick sinus syndrome. All outcomes were identified using appropriate ICD-10 diagnosis codes from the electronic health records.
Covariates
To account for potential confounding, we collected multiple baseline characteristics. Demographic information included age, sex, race, and ethnicity. For cardiac comorbidities, we documented ischemic cardiomyopathy, non-ischemic cardiomyopathy, prior myocardial infarction, atrial fibrillation, ventricular tachycardia, previous cardiac arrest, valvular heart disease, pulmonary hypertension, and previous cardiac surgery. Non-cardiac comorbidities were also collected, including hypertension, diabetes mellitus, chronic kidney disease, chronic obstructive pulmonary disease, obstructive sleep apnea, stroke, peripheral vascular disease, liver disease, and malignancy. Laboratory values assessed included hemoglobin, creatinine, blood urea nitrogen, sodium, potassium, and liver function tests. We also documented concomitant medications, such as angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, mineralocorticoid receptor antagonists, diuretics, amiodarone, digoxin, anticoagulants, and antiplatelet agents.
Statistical analysis
We employed propensity score matching to minimize confounding by indication and create comparable cohorts. Propensity scores were calculated using logistic regression, with the type of beta-blocker as the dependent variable and the covariates listed above as independent variables. Patients in the carvedilol and metoprolol groups were matched 1:1 using nearest-neighbor matching with a caliper width of 0.2 standard deviations of the logit of the propensity score [14].
Balance between the matched cohorts was assessed using standardized mean differences, with values <0.1 considered indicative of good balance. Baseline characteristics were compared between the matched groups using standardized mean differences and appropriate statistical tests (chi-square test for categorical variables and t-test or Mann-Whitney U test for continuous variables).
Time-to-event analyses were performed using Kaplan-Meier survival curves and Cox proportional hazards models to estimate hazard ratios (HR) with 95% confidence intervals (CI) for the primary and secondary outcomes. The proportional hazards assumption was tested using Schoenfeld residuals. Analyses were conducted using R version 4.0.3 (Vienna, Austria: R Foundation for Statistical Computing). A two-sided p-value <0.05 was considered statistically significant.
Ethical considerations
This study utilized de-identified data from the TriNetX Research Network, which complies with all relevant patient privacy regulations. The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board. As the study used only de-identified data, informed consent was waived.
Results
Before propensity score matching, 5,300 patients with LVADs who were prescribed carvedilol and 14,324 patients prescribed metoprolol met the inclusion criteria. Following propensity score matching, 5,166 patients remained in each group. The baseline characteristics of the matched cohorts are presented in Table 1. The matched groups were well-balanced in terms of demographics, comorbidities, and concomitant medications, with all standardized mean differences <0.1.
Table 1: Baseline conditions of patients in the study.P-values were calculated using the chi-square test for categorical variables. Statistical significance was set at p<0.05.
The cohorts were well-matched for key cardiac conditions, including heart failure (78.8% vs. 77.5%; p=0.105), atrial fibrillation (40.6% vs. 39.7%; p=0.356), dilated cardiomyopathy (21.1% vs. 20.5%; p=0.452), and other cardiomyopathies (40.4% vs. 38.3%; p=0.028). Important non-cardiac comorbidities were also similarly distributed between groups, including hypertension (59.5% vs. 56.6%; p=0.003), diabetes mellitus (41.6% vs. 40.6%; p=0.308), and chronic kidney disease (16.6% vs. 15.6%; p=0.164).
Primary outcome
The primary outcome of all-cause mortality within one year occurred in 795 patients (15.4%) in the carvedilol group and 879 patients (17.0%) in the metoprolol group (HR: 0.879, 95% CI: 0.799-0.968; p=0.009) (Figure 1). The survival benefit associated with carvedilol became apparent after approximately three months and persisted throughout the follow-up period.
Kaplan-Meier curve showing survival probability in a year after index event.Purple line represents carvedilol and green line represents metoprolol.
Secondary outcomes
The incidence of secondary outcomes in both groups is presented in Table 2. Carvedilol was associated with a significantly lower risk of several important clinical outcomes. The incidence of cardiac arrest was lower in the carvedilol group compared to the metoprolol group (257 {5.0%} vs. 314 {6.1%}; HR: 0.799, 95% CI: 0.677-0.942; p=0.007). Similarly, cardiogenic shock occurred less frequently in patients receiving carvedilol (915 {17.7%} vs. 1,084 {21.0%}; HR: 0.817, 95% CI: 0.748-0.892; p<0.001). The carvedilol group also demonstrated reduced rates of sepsis (457 {8.8%} vs. 536 {10.4%}; HR: 0.821, 95% CI: 0.724-0.930; p=0.002) and atrial fibrillation (1,411 {27.3%} vs. 1,584 {30.7%}; HR: 0.850, 95% CI: 0.792-0.914; p<0.001).
Table 2: Primary and secondary outcomes of patients in this study.Statistical analysis performed using Cox proportional hazards models. Statistical significance was set at p<0.05.
However, patients in the carvedilol group experienced significantly higher rates of certain adverse outcomes. Heart failure exacerbation was more common in the carvedilol group (3,684 {71.3%} vs. 3,405 {65.9%}; HR: 1.149, 95% CI: 1.097-1.204; p<0.001), as was acute kidney injury (1,645 {31.8%} vs. 1,454 {28.1%}; HR: 1.132, 95% CI: 1.055-1.214; p=0.001). No significant difference was observed in the incidence of sick sinus syndrome between the two groups (446 {8.6%} vs. 454 {8.8%}; HR: 0.951, 95% CI: 0.834-1.084; p=0.450). The difference in ventricular tachycardia rates was not clinically significant despite statistical significance (1,199 {23.2%} vs. 1,181 {22.9%}; HR: 0.991, 95% CI: 0.915-1.074; p<0.001).
Discussion
In this large propensity-matched cohort study of LVAD recipients, we found that carvedilol was associated with significantly lower all-cause mortality compared to metoprolol. Additionally, carvedilol use was associated with reduced risks of cardiac arrest, cardiogenic shock, sepsis, and atrial fibrillation. However, these benefits came with increased risks of heart failure exacerbation and acute kidney injury. To our knowledge, this is the largest study comparing the effectiveness of different beta-blockers specifically in LVAD patients.
Our findings regarding reduced mortality with carvedilol align with some, but not all, previous studies in the general heart failure population. The COMET trial, which compared carvedilol to immediate-release metoprolol tartrate in heart failure patients without LVADs, demonstrated a 17% relative risk reduction in all-cause mortality with carvedilol [10]. However, the COMET trial has been criticized for using lower than target doses of metoprolol and employing the immediate-release formulation rather than the extended-release formulation typically used in heart failure [15]. Other studies comparing carvedilol to metoprolol succinate have shown similar effects on left ventricular function and clinical outcomes [16].
The survival benefit observed with carvedilol in our study may be explained by several mechanisms. Carvedilol's additional alpha-1 blocking effects can reduce afterload and improve peripheral circulation, which may be particularly beneficial in LVAD patients with altered hemodynamics. Furthermore, carvedilol's antioxidant properties may help mitigate oxidative stress and inflammation, which are elevated in heart failure and potentially exacerbated by the mechanical circulatory support interface [17,18].
The additional alpha-blocking and antioxidant properties of carvedilol may contribute to this benefit by reducing atrial stretch, inflammation, and oxidative stress - all of which are implicated in the pathogenesis of atrial fibrillation [19].
The reduction in cardiogenic shock associated with carvedilol is particularly relevant in LVAD patients, who remain at risk for right ventricular failure and cardiogenic shock despite left ventricular support [20]. Carvedilol's vasodilatory effects may help maintain right ventricular-pulmonary artery coupling and reduce pulmonary vascular resistance, potentially preserving right ventricular function better than selective beta-blockade alone [21].
The finding of reduced sepsis in the carvedilol group is intriguing and warrants further investigation. It is possible that carvedilol's anti-inflammatory and antioxidant properties may modulate the systemic inflammatory response, potentially reducing susceptibility to or severity of infections [22]. LVAD patients are at high risk for infections, and any intervention that reduces this risk could have significant clinical implications [23].
However, the increased risk of heart failure exacerbation and acute kidney injury observed with carvedilol requires careful consideration. The increased risk of acute kidney injury could be attributed to carvedilol's greater vasodilatory effects, which might induce hypotension and subsequently lead to a pre-renal acute kidney injury in susceptible individuals. These findings emphasize the importance of individualized beta-blocker selection based on patient characteristics and comorbidities.
Several limitations of our study should be acknowledged. First, despite propensity score matching, residual confounding may exist due to unmeasured variables. Second, the observational nature of the study precludes causal inferences. Third, we could not assess adherence to prescribed medications beyond prescription fills, which may affect the observed outcomes. Fourth, the TriNetX database may not capture all clinical outcomes if patients received care outside the participating healthcare systems. Fifth, we could not comprehensively evaluate hemodynamic parameters or device settings that might influence outcomes. Finally, while we included both metoprolol succinate and tartrate formulations, differences between these formulations might impact the comparison with carvedilol. Despite these limitations, our study has important strengths, including the large sample size specific to LVAD recipients, robust propensity matching, and comprehensive assessment of clinical outcomes.
Conclusions
In this large propensity-matched study of LVAD recipients, carvedilol was associated with lower all-cause mortality and reduced incidence of cardiac arrest, cardiogenic shock, sepsis, and atrial fibrillation compared to metoprolol, despite higher rates of heart failure exacerbation and acute kidney injury. These findings suggest that carvedilol may be the preferred beta-blocker for many LVAD patients, though individualized consideration of heart failure status, renal function, and right ventricular function remains important for optimizing outcomes.
Future prospective randomized trials specifically in LVAD recipients are needed to confirm these findings and better define the optimal beta-blocker choice for this unique and growing patient population. Additionally, mechanistic studies exploring the physiological effects of different beta-blockers in the context of continuous-flow mechanical circulatory support would enhance our understanding of the observed clinical differences.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heart disease and stroke statistics - 2020 update: a report from the American Heart Association Circulation Virani SS Alonso A Benjamin EJ 139596141202010.1161/CIR.000000000000075731992061 · doi ↗ · pubmed ↗
- 2A fully magnetically levitated left ventricular assist device - final report N Engl J Med Mehra MR Uriel N Naka Y 1618162738020193088305210.1056/NEJ Moa 1900486 · doi ↗ · pubmed ↗
- 3Eighth Annual INTERMACS Report: special focus on framing the impact of adverse events J Heart Lung Transplant Kirklin JK Pagani FD Kormos RL 108010863620172894278210.1016/j.healun.2017.07.005 · doi ↗ · pubmed ↗
- 4The Society of Thoracic Surgeons Intermacs database annual report: evolving indications, outcomes, and scientific partnerships J Heart Lung Transplant Kormos RL Cowger J Pagani FD 1141263820193069159310.1016/j.healun.2018.11.013 · doi ↗ · pubmed ↗
- 52017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America Circulation Yancy CW Jessup M Bozkurt B 137161136201710.1161/CIR.000000000000050928455343 · doi ↗ · pubmed ↗
- 62016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC Eur Heart J Ponikowski P Voors AA Anker SD 212922003720162720681910.1093/eurheartj/ehw 128 · doi ↗ · pubmed ↗
- 72022 AHA/ACC/HFSA Guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation Heidenreich PA Bozkurt B Aguilar D 8951032145202210.1161/CIR.000000000000106335363499 · doi ↗ · pubmed ↗
- 8Meta-analysis of carvedilol versus beta 1 selective beta-blockers (atenolol, bisoprolol, metoprolol, and nebivolol)Am J Cardiol Di Nicolantonio JJ Lavie CJ Fares H Menezes AR O'Keefe JH 7657691112013 https://doi.org/10.1016/j.amjcard.2012.11.0312329092510.1016/j.amjcard.2012.11.031 · doi ↗ · pubmed ↗