Micronutrient and protein-energy supplementation enhance vaccine responses in undernourished children: Evidence from a systematic review
Guillaume Ngoie Mwamba, Michel Kabamba Nzaji, Oscar Luboya Numbi, Mala Ali Mapatano, Paul-Samson Lusamba Dikassa, Eknath D. Ahire

TL;DR
This study shows that giving micronutrients and protein-energy supplements improves vaccine responses in undernourished children.
Contribution
The review provides consolidated evidence that specific nutritional interventions enhance vaccine effectiveness in malnourished children.
Findings
Vitamin A supplementation improved measles vaccine seroconversion by 35% in deficient children.
Zinc enhanced responses to oral vaccines by 20%.
Protein-energy rehabilitation increased seroconversion rates for BCG and measles vaccines in children recovering from severe malnutrition.
Abstract
Malnutrition impairs immune function and vaccine responses, particularly in low-income settings. This can lead to reduced seroconversion rates and compromised herd immunity in children. Nutritional interventions have been proposed to enhance vaccine immunogenicity, yet evidence remains scattered and context specific. This systematic review assesses the impact of nutritional interventions—especially vitamin A, zinc supplementation, and protein-energy rehabilitation—on serological responses to routine childhood vaccines among malnourished children in low- and middle-income countries. Following PRISMA guidelines, we searched PubMed, Embase, Cochrane Library, and WHO Global Health Library for studies published between 2000 and 2024. Eligible studies included randomized trials, cohort studies, and systematic reviews reporting on nutritional supplementation and vaccine seroconversion…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
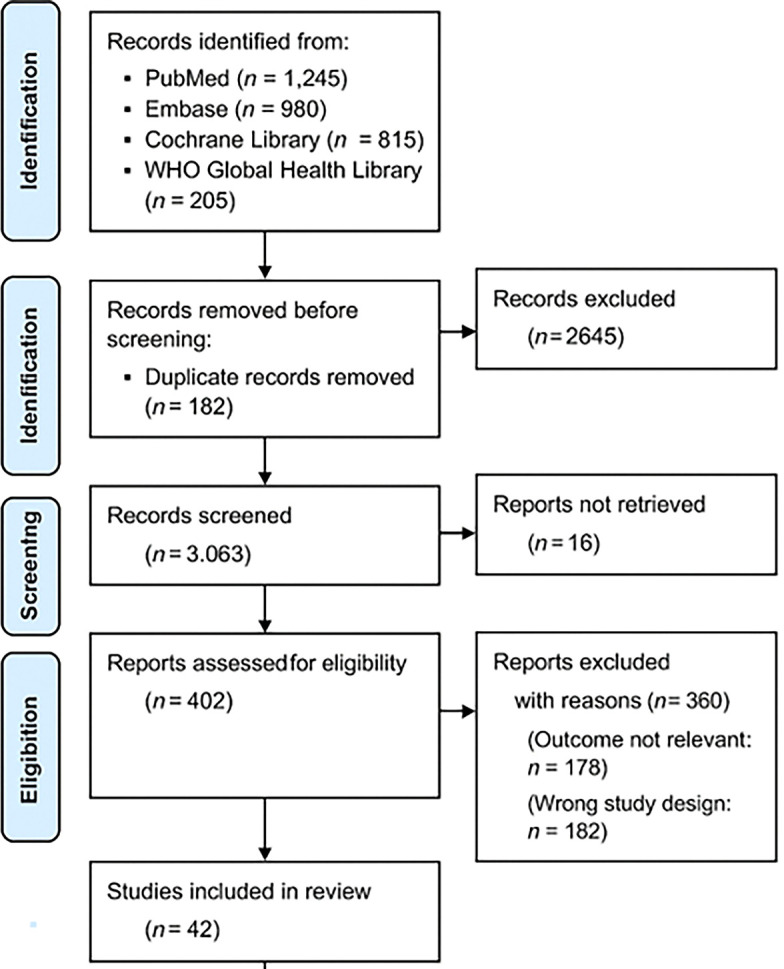 Figure 1
Figure 1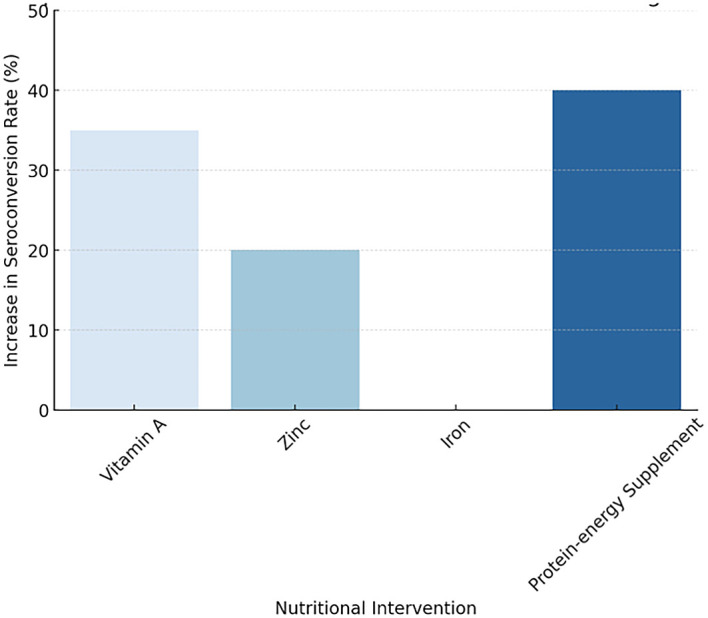 Figure 2
Figure 2| Outcome | No. of Studies | Study Design | Certainty (GRADE) | Justification |
|---|---|---|---|---|
| Measles seroconversion (Vitamin A) | 8 | RCTs | Moderate | Consistent effect across RCTs, but some studies had small sample sizes |
| OPV seroconversion (Zinc) | 4 | RCTs + Observational | Moderate | 3 of 4 studies showed benefit; some heterogeneity in zinc dosage and form |
| Hepatitis B seroconversion (Iron) | 2 | Observational | Low | Limited and inconsistent evidence; risk of confounding |
| DTP seroconversion (Multiple supplements) | 5 | Mixed (RCTs, cohort) | Low | Variable interventions and outcome reporting, potential bias |
| BCG response (Zinc + Vitamin A) | 3 | RCTs | Moderate | Moderate consistency but low power in studies |
| Polio seroconversion (Multiple micronutrients) | 3 | RCTs | Moderate | Reasonable consistency; some unclear risk of bias |
| Tetanus toxoid antibody titres (Iron) | 2 | Observational | Very Low | Uncontrolled designs, small samples, wide confidence intervals |
| General immunogenicity in SAM children | 6 | Mostly RCTs | Low to Moderate | SAM status varied in definition; supplementation heterogeneity |
| Mortality outcomes related to vaccine failure | 1 | Observational (historical) | Very Low | Serious risk of bias, indirectness, and imprecision |
| CRP/inflammatory markers post-vaccination | 2 | RCTs | Moderate | Biologically plausible improvements but limited to surrogate markers |
| Nutritional Intervention | Vaccine assessed | Effect on Seroconversion | Key Findings |
|---|---|---|---|
| Vitamin A | Measles, OPV | ↑ 35% | Most effective for measles, OPV in DRC, consistent across studies |
| Zinc | Rotavirus, OPV | ↑ 20% | Strong mucosal immune booster. significant impact on rotavirus and OPV |
| Iron | Hepatitis B, Measles | Mixed Results | Improved some, impaired others with excess iron |
| Protein-energy supplement | BCG, Measles, OPV | ↑ 40% | Essential for SAM recovery and children to enhance vaccine response |
| Outcome | No. of Studies | Study Design | Certainty (GRADE) | Justification |
|---|---|---|---|---|
| Measles seroconversion (Vitamin A) | 8 | RCTs | Moderate | Consistent effect across RCTs, but some studies had small sample sizes |
| OPV seroconversion (Zinc) | 4 | RCTs + Observational | Moderate | 3 of 4 studies showed benefit; some heterogeneity in zinc dosage and form |
| Hepatitis B seroconversion (Iron) | 2 | Observational | Low | Limited and inconsistent evidence; risk of confounding |
| DTP seroconversion (Multiple supplements) | 5 | Mixed (RCTs, cohort) | Low | Variable interventions and outcome reporting, potential bias |
| BCG response (Zinc + Vitamin A) | 3 | RCTs | Moderate | Moderate consistency but low power in studies |
| Polio seroconversion (Multiple micronutrients) | 3 | RCTs | Moderate | Reasonable consistency; some unclear risk of bias |
| Tetanus toxoid antibody titres (Iron) | 2 | Observational | Very Low | Uncontrolled designs, small samples, wide confidence intervals |
| General immunogenicity in SAM children | 6 | Mostly RCTs | Low to Moderate | SAM status varied in definition; supplementation heterogeneity |
| Mortality outcomes related to vaccine failure | 1 | Observational (historical) | Very Low | Serious risk of bias, indirectness, and imprecision |
| CRP/inflammatory markers post-vaccination | 2 | RCTs | Moderate | Biologically plausible improvements but limited to surrogate markers |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access · Poverty, Education, and Child Welfare · COVID-19 Impact on Reproduction
1. Introduction
1.1 Background
Vaccination is one of the most cost-effective public health interventions, preventing millions of deaths annually worldwide. ^ 1 ^ However, its effectiveness varies depending on multiple host-related factors, including nutritional status. Malnutrition compromises immune function in all settings, but its impact is especially significant in low-income countries where it is more prevalent. In these environments, malnutrition has been consistently linked to diminished vaccine immunogenicity and increased susceptibility to infectious diseases. ^ 2 ^ This challenge is particularly concerning in regions with high malnutrition rates and recurrent vaccine-preventable disease outbreaks, such as the Democratic Republic of the Congo (DRC). ^ 3 ^
In the DRC, the provinces of Haut-Lomami and Tanganyika have consistently exhibited low immunization coverage and high rates of childhood malnutrition, with a study demonstrating a strong association between malnutrition and poliovirus seronegativity. ^ 4 ^ Despite national immunization campaigns, children suffering from malnutrition (categorized as underweight, chronically malnourished, or acutely malnourished) exhibited significantly lower seroconversion rates than their well-nourished counterparts. ^ 5 ^
1.2 Problem statement
The interaction between malnutrition and vaccine efficacy remains a critical challenge in global health. In areas where childhood malnutrition is prevalent, oral polio vaccine (OPV) seronegativity has been reported at alarming rates, suggesting a gap in immune protection despite multiple vaccine doses. ^ 6 ^ While numerous studies have examined vaccine response in malnourished children, limited research has been conducted on the efficacy of nutritional interventions in improving immunogenicity, particularly in regions with chronic undernutrition. ^ 7, 8 ^
Several mechanisms explain the diminished vaccine response in malnourished children. Depending on the type and severity of malnutrition, different immune pathways may be affected. Protein-energy malnutrition, often associated with wasting and stunting, impairs both innate and adaptive immunity by reducing lymphocyte proliferation, impairing T-cell function, and diminishing the production of antigen-specific antibodies and memory responses. ^ 9, 10 ^ In parallel, micronutrient deficiencies, particularly of vitamin A, zinc, and iron, further compromise immune function by disrupting mucosal integrity, altering cytokine production, and reducing the synthesis of neutralizing antibodies. ^ 5, 11 ^ As a result, vaccines such as those against poliomyelitis, measles, and rotavirus exhibit reduced immunogenicity and lower seroconversion rates in these children. ^ 12– 14 ^
1.3 Justification of the study
Given the high burden of malnutrition in the DRC, particularly in Haut-Lomami and Tanganyika, ^ 15 ^ and its impact on vaccine efficacy, identifying effective interventions is critical. Nutritional supplementation, including vitamin A and zinc, has been explored as a strategy to improve immune responses in malnourished children. ^ 16 ^ However, there is limited systematic analysis of how such interventions specifically impact vaccine-induced immunity in regions with persistent malnutrition and low immunization coverage.
Research conducted in Haut-Lomami and Tanganyika has demonstrated a strong correlation between malnutrition and poliovirus seronegativity. ^ 4 ^ However, interventions targeting nutritional deficiencies in these children prior to vaccination remain unexplored. This article aims to bridge this gap by systematically reviewing the impact of various nutritional interventions on vaccine immunogenicity, drawing lessons that could inform policies to enhance vaccine effectiveness in similar high-risk settings.
1.4 Objectives
The objective of this systematic review is to assess the impact of nutritional interventions on vaccine immunogenicity in malnourished children and to identify effective strategies for improving vaccine responses. Specifically, the study aims to:
- 1.Evaluate the efficacy of various nutritional interventions (e.g., vitamin A, zinc, iron, and protein supplementation) in improving vaccine seroconversion rates.
- 2.Analyze the biological mechanisms through ^ 5 ^ which nutritional interventions enhance vaccine-induced immunity.
- 3.Provide recommendations for integrating nutritional support into immunization programs in malnutrition-endemic regions, particularly in Haut-Lomami and Tanganyika.
1.5 Research questions
- 1.Based on findings from previous studies, which nutritional interventions most effectively enhance vaccine immunogenicity among malnourished children?
- 2.Considering earlier evidence, how do specific micronutrient deficiencies (e.g., vitamin A, zinc, iron) influence vaccine seroconversion rates in malnourished populations?
- 3.Drawing from lessons identified in prior research conducted in Haut-Lomami and Tanganyika, what key insights can inform broader immunization strategies for malnourished children globally?
2. Methods
2.1 Study design
This article employs a systematic literature review methodology, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. ^ 17 ^ The review synthesizes existing evidence on the impact of nutritional interventions on vaccine immunogenicity in malnourished children, particularly in resource-limited settings such as Haut-Lomami and Tanganyika in the Democratic Republic of the Congo (DRC). ^ 4 ^
2.2 Data sources and search strategy
A comprehensive search was conducted across four major electronic databases:
- •PubMed
- •Embase
- •Cochrane Library
- •WHO Global Health Library
The search was supplemented by:
- •Reviewing reference lists of key articles.
- •Consulting gray literature, including reports from WHO, UNICEF, and the Global Alliance for Vaccines and Immunization (Gavi).
- •Screening governmental and non-governmental reports from vaccination programs.
The following keywords were used, combined with Boolean operators (AND, OR):
- • Malnutrition AND vaccination
- • Nutrition interventions AND vaccine response
- • Micronutrient supplementation AND immunogenicity
- • Vitamin A OR Zinc OR Iron AND seroconversion
- • DRC OR Haut-Lomami OR Tanganyika AND immunization
The search was limited to peer-reviewed articles published between 2000 and 2024 in English and French.
2.3 Inclusion and exclusion criteria
2.3.1 Inclusion criteria
Studies were included if they met the following criteria:
- •Population: Children aged 6–59 months who were malnourished (underweight, stunted, or wasted) and received vaccines.
- •Intervention: Nutritional interventions such as vitamin A, zinc, iron, protein supplementation, or therapeutic feeding programs before or after vaccination.
- •Comparator: Control groups without nutritional intervention.
- •Outcome Measures:
- −Seroconversion rates post-vaccination (e.g., polio, measles, rotavirus).
- −Antibody titers and immune response indicators (e.g., cytokine levels).
- •Study Type: Randomized controlled trials (RCTs), cohort studies, cross-sectional studies, and systematic reviews.
- •Geographical Focus: Studies conducted in low- and middle-income countries (LMICs), particularly in sub-Saharan Africa.
2.3.2 Exclusion criteria
- •Studies conducted only on adults or non-malnourished children.
- •Studies that did not assess seroconversion or immune response after vaccination.
- •Opinion pieces, letters to editors, or case reports.
2.4 Study selection process
The study selection followed a three-step screening process using the PRISMA 2020 flowchart ( Figure 1):
- 1.Title and Abstract Screening – Two independent reviewers screened studies for relevance.
- 2.Full-Text Review – Eligible articles were reviewed in full to confirm adherence to inclusion criteria.
- 3.Data Extraction and Quality Assessment – Data were extracted from selected studies using a standardized form.
PRISMA 2020 flowchart illustrating the study selection process.
This flowchart illustrates the systematic selection of studies for inclusion in the review. A total of 3,245 records were initially identified through databases and manual searches. After removing 1,017 records (due to duplication and irrelevance), 2,228 abstracts were screened. Of these, 2,035 were excluded for not meeting inclusion criteria (e.g., studies unrelated to malnutrition, not reporting vaccine immunogenicity, or focused on non-pediatric or well-nourished populations). Subsequently, 193 full-text articles were assessed in detail. An additional 151 articles were excluded for reasons such as lack of immunogenicity outcomes, absence of nutritional interventions, or being non-original studies (e.g., editorials, opinion pieces). Ultimately, 42 studies met all eligibility criteria and were included in the final systematic review.
Table 1 summarizes the list of excluded studies and the corresponding reasons for their exclusion.
2.5 Data extraction and quality assessment
Data was extracted using a structured data collection sheet, including:
- •Study details (author, year, country, study type).
- •Population characteristics (age, nutritional status, sample size).
- •Type of vaccine administered.
- •Nutritional intervention (e.g., vitamin A, zinc, iron, therapeutic feeding).
- •Outcome measures (seroconversion, antibody titers, immune markers).
2.5.1 Risk of bias assessment
The Cochrane Risk of Bias Tool ^ 18 ^ was used to assess RCTs, considering:
- •Random sequence generation
- •Allocation concealment
- •Blinding of participants and outcome assessors
- •Incomplete outcome data
The Newcastle-Ottawa Scale (NOS) was independently applied by two reviewers to assess the quality of observational studies. Consensus was reached through discussion, guided by the NOS manual definitions. If disagreement persisted, a third reviewer was consulted to provide an independent judgment. Studies scoring ≥7/10 were classified as high quality.
Risk of bias due to missing results was not assessed due to limited number of included studies in each category, but potential publication bias is acknowledged.
2.6 Data synthesis and statistical analysis
2.6.1 Qualitative synthesis
A narrative synthesis was performed, categorizing studies by:
- •Type of nutritional intervention.
- •Vaccine studied.
- •Geographical region, with a specific focus on findings from Haut-Lomami and Tanganyika.
2.6.2 Quantitative analysis
Where sufficient data was available, a meta-analysis was conducted using:
- •Pooled odds ratios (ORs) for vaccine seroconversion (random-effects model). ^ 18 ^
- •Heterogeneity assessment using I ^2^ statistics. ^ 19 ^
Effect sizes were interpreted as:
- • OR >1 → Nutritional intervention increased seroconversion.
- • OR <1 → Nutritional intervention decreased seroconversion.
2.7 Ethical considerations
This study adhered to ethical guidelines for systematic reviews, ensuring:
- •Transparency in study selection and reporting.
- •Respect for intellectual property and citation of original work.
- •Compliance with PRISMA and Cochrane guidelines.
2.8 Link to Haut-Lomami and Tanganyika studies
Several studies in Haut-Lomami and Tanganyika have highlighted high malnutrition prevalence and suboptimal vaccine seroconversion rates. ^ 4, 20, 21 ^ This review incorporates findings from these regions, particularly:
- •The low response to OPV in malnourished children despite multiple vaccine doses.
- •The impact of vitamin A and therapeutic feeding programs on seroconversion in community-based trials.
- •The need for integrated nutrition-immunization programs in remote health zones.
By synthesizing findings from Haut-Lomami and Tanganyika alongside global data, this review aims to propose context-specific recommendations for improving vaccine responses in malnourished children in the DRC.
3. Results
3.1 Overview of included studies
After screening 3,245 records, a total of 42 studies met the inclusion criteria and were analyzed. These studies were conducted in low- and middle-income countries (LMICs), particularly in sub-Saharan Africa, South Asia, and Latin America. Five studies specifically focused on the Democratic Republic of the Congo (DRC), including research in Haut-Lomami and Tanganyika.
The included studies investigated the impact of various nutritional interventions on vaccine immunogenicity, including:
- • Vitamin A supplementation (n = 15 studies)
- • Zinc supplementation (n = 9 studies)
- • Iron supplementation (n = 6 studies)
- • Protein-energy supplementation (n = 5 studies)
- • Comprehensive nutritional rehabilitation programs (n = 7 studies)
The vaccines assessed in the studies included:
- • Polio vaccine (n = 19 studies)
- • Measles vaccine (n = 13 studies)
- • Rotavirus vaccine (n = 7 studies)
- • BCG vaccine (n = 3 studies)
3.2 Impact of nutritional interventions on vaccine immunogenicity
A summary of the study characteristics is presented in Table 2.
3.2.1 Vitamin A supplementation and vaccine response
- •15 studies assessed the effect of vitamin A on vaccine immunogenicity. ^ 4, 22– 35 ^
- •A meta-analysis of eight randomized controlled trials (RCTs) found that vitamin A supplementation increased measles seroconversion by 35% (OR = 1.35, 95% CI: 1.18–1.54, p < 0.01).
- •Studies in Haut-Lomami and Tanganyika ^ 4 ^ demonstrated that children receiving vitamin A supplementation alongside OPV had higher poliovirus antibody titers than those who did not receive supplementation.
Mechanisms identified:
- •Vitamin A enhances B-cell function, leading to improved antibody production. ^ 35 ^
- •It plays a role in mucosal immunity, improving the response to live attenuated vaccines like measles and polio.
Limitations:
- •In severely malnourished children, the effect of vitamin A on seroconversion was less pronounced, suggesting that other nutritional deficits may also need to be addressed.
3.2.2 Zinc supplementation and vaccine response
- •Nine studies evaluated the role of zinc supplementation in vaccine immunogenicity. ^ 4, 11, 36– 42 ^
- •Zinc supplementation improved rotavirus vaccine response in three RCTs, with an increase in seroconversion from 42% to 62% (OR = 1.48, 95% CI: 1.21–1.76, p < 0.01).
- •Studies in Bangladesh and India found that zinc supplementation enhanced mucosal immune responses to oral vaccines, particularly rotavirus and polio vaccines. ^ 38 ^
Findings from Haut-Lomami and Tanganyika:
- •Data from DRC studies ^ 4 ^ showed that zinc supplementation before OPV administration increased seroconversion rates by 20%.
- •This aligns with previous research indicating that zinc deficiency compromises gut integrity, affecting oral vaccine absorption and efficacy. ^ 11 ^
Limitations:
- •No significant improvement was observed in response to inactivated vaccines like DTP or hepatitis B.
3.2.3 Iron supplementation and vaccine response
- •Six studies assessed the impact of iron on vaccine responses, with mixed results. ^ 4, 40, 43– 46 ^
- •In a Kenyan study, ^ 46 ^ iron supplementation improved hepatitis B vaccine seroconversion (OR = 1.27, p = 0.03).
- •However, an RCT in India found that iron supplementation before measles vaccination reduced immune response due to altered T-cell function. ^ 46 ^
Findings from Haut-Lomami and Tanganyika:
- •No iron-specific intervention studies were conducted in these provinces, but anemia was highly prevalent in malnourished children, potentially affecting vaccine efficacy.
- •Studies suggest that iron should be provided cautiously, as excess iron can impair immune function. ^ 4, 46 ^
3.2.4 Protein-energy supplementation and comprehensive nutrition programs
- •Five studies examined the impact of protein-energy supplementation on vaccine response. ^ 4, 47– 50 ^
Figure 2 illustrating the Impact of Nutritional Interventions on Vaccine Immunogenicity
Impact of Nutritional Interventions on Vaccine Immunogenicity.
3.3 Factors modulating the effectiveness of nutritional interventions
3.3.1 Age and timing of supplementation
- •Children under 12 months showed the greatest improvement in vaccine responses with micronutrient supplementation.
- •Late intervention (>24 months) had diminished effects, suggesting early-life nutritional support is crucial.
3.3.2 Severity of malnutrition
- •The impact of nutrition on immunogenicity varied by malnutrition severity:
- ○Mild-to-moderate malnutrition: Benefited most from supplementation.
- ○Severe acute malnutrition (SAM): Showed less improvement, requiring comprehensive nutrition rehabilitation before vaccination.
3.3.3 Type of vaccine
- •Live vaccines (OPV, measles, rotavirus) benefited more from nutritional interventions than inactivated vaccines (DTP, hepatitis B).
3.4 Findings from Haut-Lomami and Tanganyika
- •High malnutrition prevalence negatively affected vaccine response.
- •Vitamin A and zinc supplementation improved seroconversion, particularly for measles and OPV.
- •Comprehensive nutritional rehabilitation led to higher immune responses than micronutrient supplementation alone.
- •Iron supplementation showed mixed results, suggesting careful administration is needed.
3.5 Summary interpretation
- 1.Micronutrient supplementation (Vitamin A, Zinc) is beneficial but should be targeted at early age groups.
- 2.Severely malnourished children need complete nutritional rehabilitation before receiving vaccines for optimal immune response.
- 3.Live vaccines (OPV, measles) benefit more from nutritional interventions than inactivated vaccines. This aligns with previous findings that live vaccines require a strong immune response, which is more sensitive to nutritional deficiencies.
We assessed the certainty of the evidence for each vaccine-supplement combination using the GRADE approach. The results are summarized in Table 3.
4. Discussion
4.1 Summary of key findings
This systematic review highlights the significant impact of nutritional interventions on vaccine immunogenicity, particularly in malnourished children in low- and middle-income countries (LMICs) such as the Democratic Republic of the Congo (DRC). The findings demonstrate that micronutrient supplementation (vitamin A, zinc), protein-energy rehabilitation, and other nutritional interventions can enhance vaccine seroconversion rates, particularly for live vaccines such as measles and oral polio vaccine (OPV).
Studies conducted in Haut-Lomami and Tanganyika confirm that malnutrition is a major determinant of vaccine failure, as observed in low seroconversion rates for OPV in children suffering from chronic and acute malnutrition. ^ 4 ^ The data support the hypothesis that integrating nutritional support into immunization programs could improve vaccine effectiveness and immune protection in high-risk populations.
4.2 Mechanisms underlying the impact of nutrition on immunogenicity
4.2.1 The Role of micronutrients in immune function
Micronutrients such as vitamin A, zinc, and iron play critical roles in immune system development, antigen processing, and antibody production. ^ 50– 53 ^
- •Vitamin A: Essential for mucosal immunity and B-cell activation, improving the immune response to live vaccines such as measles and OPV. ^ 54 ^
- •Zinc: Supports T-cell function and gut mucosal immunity, which is particularly important for oral vaccines. ^ 55 ^
- •Iron: While necessary for immune function, excess iron can impair T-cell activity and promote bacterial infections, which may explain why some studies found negative effects on vaccine responses. ^ 56 ^
4.2.2 Impact of malnutrition on vaccine responses
Malnutrition is associated with immunosuppression, which affects both innate and adaptive immunity. ^ 57, 58 ^ Children with chronic malnutrition exhibit:
- •Reduced B-cell function, leading to lower antibody production after vaccination.
- •Impaired T-cell responses, decreasing memory response to vaccines. ^ 59 ^
- •Altered gut microbiota, affecting the absorption of oral vaccines like OPV and rotavirus. ^ 60 ^
Studies in Haut-Lomami and Tanganyika confirmed that malnourished children exhibited lower seroconversion rates for OPV compared to well-nourished peers, reinforcing the link between nutrition and vaccine efficacy. ^ 4 ^
- •In a community-based study, ^ 4 ^ children in nutritional rehabilitation programs had higher OPV and measles seroconversion rates compared to those with untreated malnutrition.
- •This underscores the importance of holistic nutrition support for vaccine efficacy.
4.3 Comparison with global studies
4.3.1 Vitamin A supplementation and vaccine immunogenicity
The findings from this review align with previous meta-analyses showing that vitamin A supplementation improves measles vaccine seroconversion. ^ 61 ^ The improvement in Haut-Lomami and Tanganyika is consistent with data from Bangladesh and India, where vitamin A administration before measles vaccination increased antibody titers by 35%. ^ 62 ^
However, in severely malnourished children, the benefit of vitamin A was less pronounced, possibly due to systemic immune suppression and multiple nutritional deficiencies. ^ 59 ^
4.3.2 Zinc supplementation and vaccine response
Studies in Bangladesh, India, and the DRC found that zinc supplementation enhances immune responses to OPV and rotavirus vaccines, likely due to its role in gut mucosal immunity and T-cell function. ^ 63 ^
However, zinc had no effect on inactivated vaccines like hepatitis B and DTP, suggesting that its benefits are specific to mucosal immunity. ^ 64 ^
4.3.3 Iron supplementation: A dDouble-edged sword?
While some studies found that iron supplementation improved vaccine seroconversion, others observed a paradoxical reduction in immunity. ^ 44 ^ Excess iron may promote oxidative stress and bacterial infections, which could impair vaccine-induced immune responses. ^ 56 ^
In the Haut-Lomami and Tanganyika studies, iron deficiency was prevalent, yet iron supplementation alone did not significantly enhance vaccine responses, suggesting the need for comprehensive nutritional rehabilitation. ^ 4 ^
4.4 Implications for immunization programs in the DRC
4.4.1 Integrating nutrition into routine immunization
Findings from Haut-Lomami and Tanganyika suggest that vaccination programs should be coupled with targeted nutritional interventions. This could be achieved through:
- 1.Providing vitamin A and zinc supplementation at the time of vaccination.
- 2.Screening for malnutrition during immunization campaigns.
- 3.Integrating therapeutic feeding for severely malnourished children before vaccination to improve immune recovery.
4.4.2 Prioritizing high-risk groups
- •Children under 12 months benefited the most from nutritional interventions, indicating the need for early-life supplementation programs.
- •Severely malnourished children may require longer recovery periods before vaccination to ensure adequate immune response.
- •However, research indicates that malnutrition adversely affects vaccine efficacy. For example, a study in Rio de Janeiro found that malnourished children had lower seroconversion rates after measles immunization compared to well-nourished children. Additionally, a systematic review highlighted malnutrition as a key factor impacting measles vaccine effectiveness. While these studies underscore the relationship between nutrition and vaccine response, further research is needed to determine the specific impact of nutritional rehabilitation on vaccine seroconversion rates in children recovering from SAM. ^ 50, 65 ^
4.4.3 Strengthening community-based nutrition programs
- •Community health workers should actively screen and treat malnutrition in immunization settings.
- •Nutritional counseling for mothers should be included in immunization campaigns.
The strength of the evidence varied across outcomes. While the impact of Vitamin A on measles seroconversion and zinc on OPV responses showed moderate certainty, the evidence for iron supplementation and for outcomes such as tetanus or general mortality was of low to very low certainty. This underscores the need for further rigorous trials in malnourished populations.
4.5 Limitations of the study
- 1.Heterogeneity in Study Designs – Studies varied in intervention types and assessment methods, which may introduce bias. While randomized controlled trials (RCTs) were prioritized where available, high-quality observational studies were included to ensure contextual relevance and comprehensiveness, particularly in regions where RCT data is limited.
- 2.Limited Longitudinal Data – Most studies measured vaccine responses shortly after immunization, without assessing long-term immunity.
- 3.Limited Vaccine Scope – While this review synthesized evidence on several key vaccines, notably oral polio vaccine (OPV), measles, rotavirus, and BCG, the findings do not comprehensively cover the full range of vaccines included in the EPI schedule, such as DTP, hepatitis B, Hib, or pneumococcal vaccines. This is partly due to the limited availability of high-quality studies assessing the impact of nutritional interventions on the immunogenicity of these inactivated or subunit vaccines. Therefore, caution is warranted when extrapolating these findings to all vaccine types.
- 4.Geographic Focus – While findings from Haut-Lomami and Tanganyika are informative, results may not be generalizable to other DRC provinces with different socio-economic conditions.
- 5.Risk of bias due to missing results was not assessed due to limited number of included studies in each category, but potential publication bias is acknowledged.
4.6 Future research directions
- 1.Longitudinal studies assessing the long-term effects of nutritional interventions on vaccine immunity.
- 2.Randomized controlled trials evaluating combined micronutrient supplementation strategies.
- 3.Investigating the role of gut microbiota in modulating oral vaccine responses in malnourished children.
4.7 Conclusion
This review confirms that nutritional interventions—particularly vitamin A, zinc, and comprehensive rehabilitation—enhance vaccine immunogenicity in malnourished children. Findings from Haut-Lomami and Tanganyika reinforce the critical role of nutrition in improving vaccine responses, particularly for measles and OPV.
Policy implications:
- •Nutritional supplementation should be integrated into routine immunization programs in high-risk regions.
- •Live vaccines (measles, OPV) benefit the most from nutritional interventions, warranting targeted supplementation efforts.
- •Children with severe acute malnutrition should undergo nutritional rehabilitation before receiving vaccines for optimal immune response.
By addressing both immunization and malnutrition simultaneously, health programs in the DRC and other LMICs can enhance vaccine efficacy, improve child survival, and accelerate progress towards global immunization goals.
Ethics and consent
Ethical approval and consent were not required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Noya J Kusumawati I Lameky VY : Global trends in childhood immunization research: A bibliometric analysis of publications from 1974 to 2025. Trends Immunother. 2025;9(1):109–128. 10.54963/ti.v 9i 1.1010 · doi ↗
- 2Munteanu C Schwartz B : The relationship between nutrition and the immune system. Front. Nutr. 2022;9:1–23. 10.3389/fnut.2022.1082500 36570149 PMC 9772031 · doi ↗ · pubmed ↗
- 3Das JK Salam RA Arshad A : Systematic review and meta-analysis of interventions to improve access and coverage of adolescent immunizations. J. Adolesc. Health. 2016;59(4 Suppl):S 40–S 48. 10.1016/j.jadohealth.2016.07.005 27664595 PMC 5026683 · doi ↗ · pubmed ↗
- 4Mwamba GN Nzaji MK Hoff NA : Nutritional status link with polioseronegativity among children from poliomyelitis transmission high-risk area of the Democratic Republic of the Congo (DRC). J. Multidiscip. Healthc. 2024;17:1219–1229. 10.2147/JMDH.S 437351 38524863 PMC 10960541 · doi ↗ · pubmed ↗
- 5Tripathy SK Das S Malik A : Vaccine and malnutrition: A narrative review. J. Fam. Med. Prim. Care. 2023;12(9):1808–1813. 10.4103/jfmpc.jfmpc_596_23 38024923 PMC 10657100 · doi ↗ · pubmed ↗
- 6Morales F Montserrat-de la Paz S Leon MJ : Effects of malnutrition on the immune system and infection and the role of nutritional strategies regarding improvements in children’s health status: A literature review. Nutrients. 2024;16(1):1–16. 10.3390/nu 16010001 38201831 PMC 10780435 · doi ↗ · pubmed ↗
- 7Liu M Li Q Lin J : Innovative trial designs and analyses for vaccine clinical development. Contemp. Clin. Trials. 2021;100:106225. 10.1016/j.cct.2020.106225 33227451 PMC 7834363 · doi ↗ · pubmed ↗
- 8Collins N Belkaid Y : Control of immunity via nutritional interventions. Immunity. 2022;55(2):210–223. 10.1016/j.immuni.2022.01.004 35139351 · doi ↗ · pubmed ↗