An Unusual Etiology of Presyncopal Episodes: Dynamic Left Ventricular Outflow Tract Obstruction Secondary to an Elongated Anterior Mitral Valve Leaflet
Stylianos Karvounaris, Ioannis Michaelides, Theodoros Ntoskas, Konstantinos Ritsatos, Georgios Papaetis

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
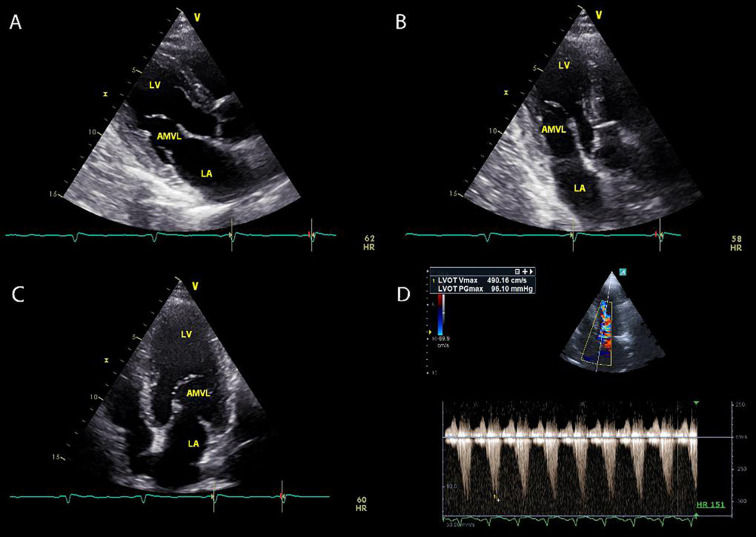 Figure 1
Figure 1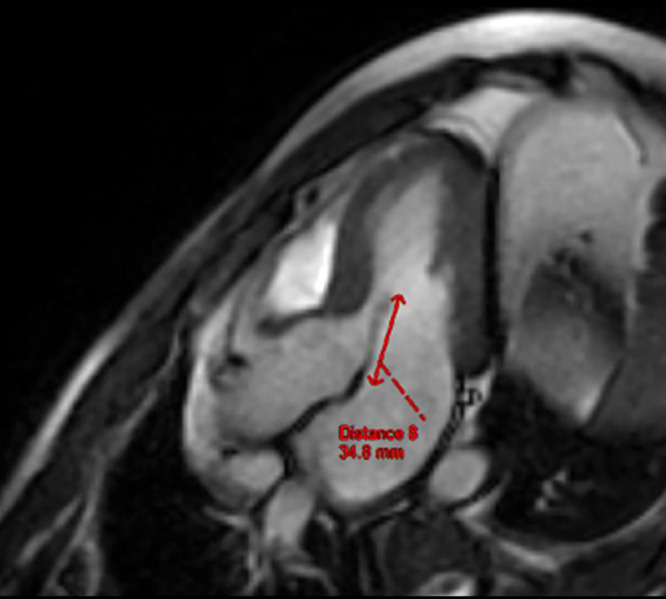 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Arrhythmias and Treatments · Infective Endocarditis Diagnosis and Management
Dynamic left ventricular outflow tract obstruction (LVOTO) refers to the restriction of blood flow from the left ventricle (LV) to the aortic arch. LVOTO can be classified as valvular, sub-valvular, or supravalvular. ^ 1 ^ Hemodynamically, it is defined by an instantaneous peak pressure gradient (PPG) at the LV outflow of ≥30 mmHg, either at rest or upon provocation. ^ 1 , 2 ^ Gradients ≥50 mmHg, whether at rest or provoked, are considered clinically significant, as they are associated with symptom development and serve as the threshold for initiating standard therapy. ^ 2 , 3 ^ In refractory cases, advanced pharmacological or invasive interventions might be required. ^ 3 ^ Although LVOTO is most commonly described in patients with hypertrophic cardiomyopathy (HCM), it can also be congenital or secondary to other conditions, such as bicuspid aortic valve with coarctation of the aorta and cardiac amyloidosis. ^ 2 , 3 ^
A 45-year-old man with a medical history of dyslipidemia presented with presyncopal episodes occurring during exertion over the past 18 months. He reported near-fainting episodes lasting for seconds to several minutes during physical activity, accompanied by generalized fatigue, lightheadedness, dizziness, and rarely, blurry vision. The patient was on atorvastatin 20 mg daily (Viatris Inc., USA) for dyslipidemia. Clinical examination, including supine and standing blood pressure and heart rate measurements, lung auscultation, palpitation of the peripheral pulses, and neurological examination was unremarkable except for a 2/6 systolic murmur best heard at the apex. Initial cardiological evaluations, including an electrocardiogram and 48-hour Holter monitoring, revealed no abnormalities. Transthoracic echocardiogram (TTE) (GE Vivid 9, USA, and Alpinion ECUBE 8, South Korea) demonstrated preserved LV contractility (ejection fraction: 65%), normal cardiac chamber dimensions, and no evidence of hypertrophy. However, an elongated anterior mitral valve leaflet (AMVL) with mild mitral valve regurgitation (MR) was observed (figure 1 A-C).
Laboratory investigations, including complete blood count (cbc), erythrocyte sedimentation rate (ESR), C-reactive protein, thyroid indices, electrolytes, blood gas analysis, troponin, D-dimer concentrations, and cortisol levels were all within normal limits. Computed tomography (CT) scans of the chest and abdomen (North Star Imaging Inc., USA) and magnetic resonance imaging (MRI) of the brain (Philips Ingenia MRI 3T, Germany) revealed no abnormalities. An exercise stress test was performed, which showed no evidence of ischemia. However, the test was terminated prematurely due to the patient experiencing near-fainting episodes accompanied by dizziness and lightheadedness. Subsequently, a dobutamine stress echocardiogram (DSE) was conducted, which also revealed no signs of ischemia but reproduced the same symptoms. During the DSE, dynamic LVOTO was identified, caused by the motion of the AMVL, with a PPG of 96 mmHg (figure 1D). A cardiac MRI scan (GE SIGNA EXCITE II, USA) confirmed the presence of an elongated AMVL (34.8 mm, normal range: 22-23 mm) with no other additional abnormalities (figure 2). The patient was initiated on bisoprolol (Merck KGaA, Darmstadt, Germany) 5 mg daily, which resulted in significant symptomatic improvement.
To our knowledge, this study is the first published case of dynamic LVOT obstruction caused by an abnormally elongated AMVL leading to presyncopal episodes in a patient without HCM or any other obvious cardiac pathology. Although most cases of exercise-induced syncope or presyncope are of neurocardiogenic origin and are benign, persistent symptoms warrant the exclusion of structural cardiovascular abnormalities and/or cardiac arrhythmias. ^ 4 ^
Several studies suggested that an abnormally elongated AMVL was closely related to the severity of LVOTO in patients with HCM. ^ 5 , 6 ^ However, the flow dynamics and drag forces generated by an abnormally elongated AMVL can interact with the interventricular septum, leading to systolic anterior motion (SAM) of the MV. This mechanism can result in LVOTO and MR even in the absence of cardiac hypertrophy, potentially precipitating presyncopal episodes. ^ 5 , 6 ^ Several diagnostic maneuvers, such as the Valsalva maneuver and exercise testing combined with simultaneous echocardiography, were employed to diagnose LVOTO. ^ 3 , 7 ^ Although DSE is not routinely used to identify latent LVOTO, it was instrumental in this case for establishing a definitive diagnosis. ^ 4 , 7 ^ Additionally, the potential association between syncope or presyncope and occult malignancy (particularly lung and brain cancers) or paraneoplastic phenomena (e.g., carcinoid syndrome or pheochromocytoma) prompted further investigation with CT scans of the chest and abdomen, as well as MRI of the brain in this patient. ^ 8 ^
Written informed consent was obtained from the patient for the publication of all data included in this report, with the condition of maintaining anonymity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aboulhosn J Child JS Left ventricular outflow obstruction: subaortic stenosis, bicuspid aortic valve, supravalvar aortic stenosis, and coarctation of the aorta Circulation 200611424122210.1161/CIRCULATIONAHA.105.59208917130357 · doi ↗ · pubmed ↗
- 2Maron MS Olivotto I Zenovich AG Link MS Pandian NG Kuvin J Tetal Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction Circulation 20061142232910.1161/CIRCULATIONAHA.106.64468217088454 · doi ↗ · pubmed ↗
- 3Ommen SR Ho CY Asif IM Balaji S Burke MA Day S Metal 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines Circulation 2024149 e 1239 e 31110.1161/CIR.000000000000125038718139 · doi ↗ · pubmed ↗
- 4Mc Award KJ Moriarity JM Exertional syncope and presyncope: faint signs of underlying problems Phys Sportsmed 20053372010.3810/psm.2005.11.24520086338 · doi ↗ · pubmed ↗
- 5Morant K Mikami Y Nevis I Mc Carty D Stirrat J Scholl Detal Contribution of mitral valve leaflet length and septal wall thickness to outflow tract obstruction in patients with hypertrophic cardiomyopathy Int J Cardiovasc Imaging 20173312011110.1007/s 10554-017-1103-528391581 · doi ↗ · pubmed ↗
- 6Henein M Arvidsson S Pilebro B Backman C Morner S Lindqvist P Long mitral valve leaflets determine left ventricular outflow tract obstruction during exercise in hypertrophic cardiomyopathy Int J Cardiol 2016212475310.1016/j.ijcard.2016.03.04127031819 · doi ↗ · pubmed ↗
- 7Harris KM Spirito P Maron MS Zenovich AG Formisano F Lesser J Retal Prevalence, clinical profile, and significance of left ventricular remodeling in the end-stage phase of hypertrophic cardiomyopathy Circulation 20061142162510.1161/CIRCULATIONAHA.105.58350016831987 · doi ↗ · pubmed ↗
- 8Lorenzen MOB Farkas DK Adelborg K Sundboll J Sorensen HT Syncope as a sign of occult cancers: a population-based cohort study Br J Cancer 202012259560010.1038/s 41416-019-0692-231857722 PMC 7029007 · doi ↗ · pubmed ↗