Removal of FIGO V and VI fibroids with a combined size greater than 5 cm quadruples spontaneous fecundity relative to myomectomy for those with smaller fibroids
Magdalena Boegl, Johannes Ott, Elena Seidl, Tal Goldstein, John Preston Parry, Marlene Hager

TL;DR
Removing large fibroids (greater than 5 cm) significantly increases the chance of spontaneous pregnancy compared to smaller fibroid removal.
Contribution
The study shows that larger fibroid removal is associated with higher spontaneous pregnancy rates after myomectomy.
Findings
Almost half of the women became pregnant within 12 months after myomectomy.
Fibroid size was significantly associated with pregnancy odds.
Larger fibroids (greater than 5 cm) led to higher pregnancy rates.
Abstract
Fibroids are the most common gynecological pathology in reproductive aged women and contribute to 2–3% of infertility cases. After hysteroscopic removal of submucosal FIGO 0 and I fibroids, pregnancy rates of 60% to 90% can be achieved. Pregnancy rates after non-hysteroscopic removal of subserosal FIGO V and VI fibroids remain controversial. We examined all myomectomies per laparoscopy/laparotomy for FIGO V and VI fibroids performed at the Clinical Division of Gynecological Endocrinology and Reproductive Medicine, Medical University of Vienna, from 2012 to 2021. All women with primary and secondary infertility between the ages of 18 and 40 years with 1–3 subserous fibroids without additionally identified causes for infertility were included. The outcome was the clinical pregnancy rate within 12 months after a postoperative non-conception window. A logistic regression model was used to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
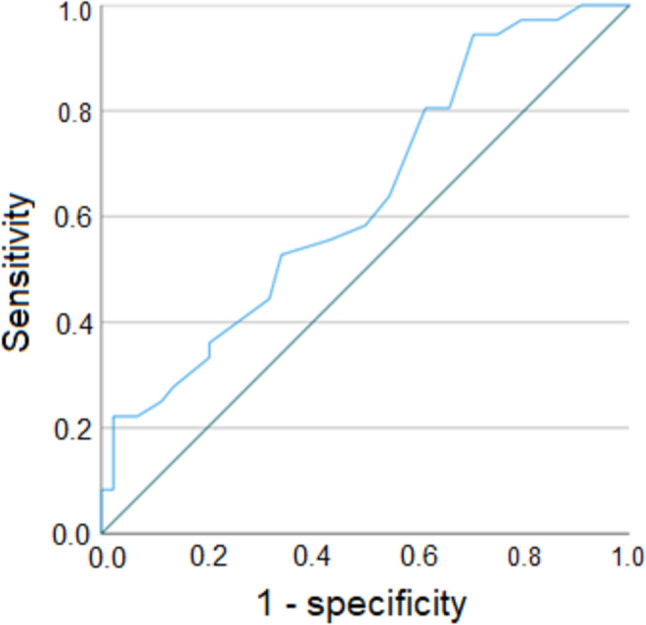 Figure 1
Figure 1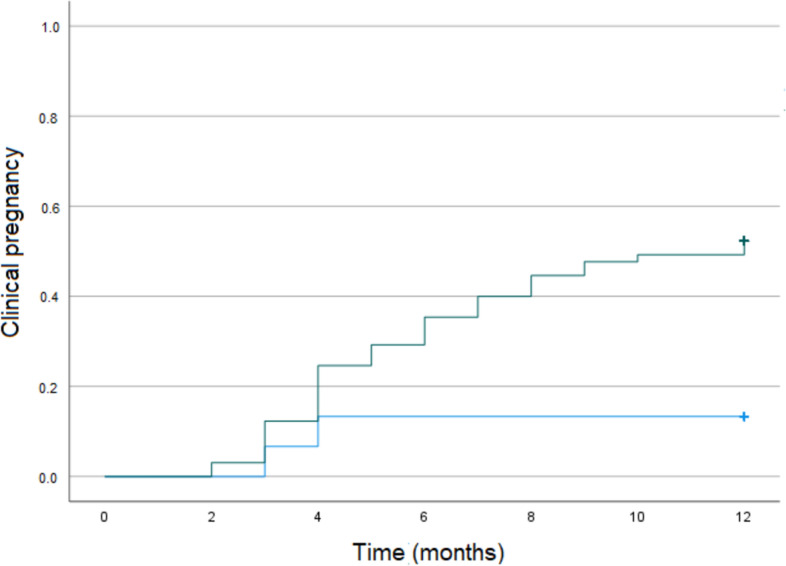 Figure 2
Figure 2- —Medical University of Vienna
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Gynecological conditions and treatments · Endometriosis Research and Treatment
What does this study add to the clinical work
The effects of subserosal fibroid removal on fertility are still unknown. This observational study found that the removal of FIGO V and VI fibroids with a combined size greater than 5cm quadruples spontaneous conception compared to myomectomy in those with smaller fibroids.
Background
Uterine fibroids are the most common gynecological pathology in reproductive aged women with an estimated lifetime prevalence of up to 70% [1, 2]. Although they are benign tumors that often remain asymptomatic, uterine fibroids are a notable cause of recurrent pregnancy loss and contribute to 2–3% of all cases of infertility [3, 4].
Fibroids are classified by the International Federation of Gynecology and Obstetrics (FIGO) [4] into nine types (0–8), depending on the location (submucosal, intramural, subserosal, and transmural) and the degree of intramural or intracavitary protrusion. Submucosal fibroids (FIGO 0-III) are most frequently associated with infertility. Several hypotheses have already been put forward to explain the connection between fibroids and infertility. One hypothesis suggests that the mechanical deformation of the uterine cavity may hinder the transport of germ cells and embryos, subsequently impairing implantation [5, 6]. Another hypothesis posits that fibroids could alter the expression patterns of angiogenic factors (such as basic fibroblast growth factor and platelet-derived growth factor) [7, 8]. Additional hypotheses why patients with fibroids experience fertility problems include inflammation [7, 9] and alterations of the endometrial lining [9]. As published by the American Society for Reproductive Medicine [5], there is a recommendation surgical removal if a desired pregnancy does not occur after all other causes for infertility have been ruled out. Pregnancy rates of up to 60–89.2% can be achieved with hysteroscopic myectomy [10, 11].
In contrast, the association of fibroids with subserosal localization (FIGO V-VI) and infertility is less clear. Consequently, there are no clear recommendations as to whether FIGO V-VI fibroids should be surgically removed to improve fecundity rates due to heterogeneous study designs, inconsistent nomenclature, diversity of leiomyoma, and patient characteristics including superimposed sources for subfertility, such as male subfertility and endometriosis among others. In addition, subserosal fibroids cannot be treated hysteroscopically instead requiring laparoscopic or laparotomic surgery, reflecting greater effort in intervention. Some data suggest that larger fibroids > 2.85 cm [12, 13] or > 3 cm [12] restrict reproduction, while other findings suggest that fibroids < 5 cm do not [14, 15]. Thus, one could hypothesize that only women with larger FIGO V-VI fibroids might benefit from myomectomy in terms of fertility.
Given the fact that there are little data on the chances of pregnancy after surgery for subserosal fibroids [16, 17], we examined the pregnancy rates of all women with at least 1 year of infertility who underwent laparoscopic or open surgery for subserosal fibroids at our clinic in the last 12 years. In addition, the focus was also on parameters influencing clinical pregnancy, first and foremost being fibroid size.
Methods
Study design
We conducted a cohort study to investigate the clinical pregnancy rates within 12 months after myomectomy by laparoscopy/laparotomy and a postoperative non-conception window of 6–9 months after the operation in infertile women with FIGO V and FIGO VI fibroids.
Study setting and participants
The study was performed at the Clinical Division of Gynecological Endocrinology at the Medical University of Vienna, Austria. All women between 18 and 40 years of age with a history of primary or secondary infertility and ≤ 3 subserous FIGO V and VI fibroids who underwent laparoscopy or laparotomy between January 2012 and December 2021, after all other cases of infertility had been ruled out, were eligible for participation (complete case analysis). We chose to not include women with four or more fibroids due to the small number of such patients in our retrospective data set as well as to keep the patient population as consistent as possible. In each of these patients, all fibroids which had been visible with preoperative transvaginal ultrasound were removed during the operation. Infertility was defined as the inability to conceive within 1 year (or 6 months, if older than 35 years), of regular unprotected intercourse. Primary infertility referred to the inability to achieve pregnancy in individuals who had never achieved a pregnancy before, while secondary infertility was deemed when at least one prior pregnancy had been achieved [18]. Women with FIGO I, II, III, IV, and VII fibroids as well as other possible causes of infertility, which included endometriosis, adenomyosis, fallopian tube obstruction, sexually transmitted diseases, ovulatory disorders (hypogonadotropic hypogonadism, polycystic ovary syndrome, functional hypothalamic amenorrhea, and oligo- or anovulation), diminished ovarian reserve, and an abnormal semen analysis of the partner, were excluded.
All operations, either via laparotomy or laparoscopy, were performed under general anesthesia. The techniques had been described previously [19] and had also been used for prospective studies at the Medical University of Vienna [20]. The decision for either laparoscopy or laparotomy was based on the size and numbers of the fibroids as well as on the patients’ and surgeons’ preference.
Study outcomes
All patients were recommended to avoid pregnancy for 6–9 months after the operation (non-conception window). The primary study outcome was the clinical pregnancy rate within 12 months after surgical recovery once pregnancy was permitted. Clinical pregnancy was defined as a pregnancy confirmed by a heartbeat on ultrasound. In an exploratory data analysis, possible associations between patient and fibroid characteristics and fecundity were investigated.
The following relevant parameters were included: patient’s age at the time of operation; body mass index (BMI); primary versus secondary infertility; the number and the size (maximum diameter) of the fibroids as well as the sum of the maximum diameter of all fibroids; the type of surgery; and the time to conceive (date from which the patient was allowed to become pregnant to positive pregnancy test, in months). In accordance with the data protection regulations applicable in Austria, all information collected was pseudonymized and transferred to a Microsoft Excel (Microsoft Corporation, Redmon, WA, USA) data processing table. All data were retrieved from the AKIM-software (SAP-based patient management system at the Medical University of Vienna).
Statistical analysis
Categorical variables are presented as absolute numbers (n) and frequencies (%), and continuous variables as median and interquartile range (IQR). For the pregnancy rate, the corresponding 95% CI was calculated. We used a logistic regression model to analyze associations of patient characteristics [including age, body mass index (BMI), and type of infertility] and surgery/fibroid characteristics [including type of myomectomy (laparoscopy versus laparotomy), diameter of the largest fibroid (cm), and the sum of fibroid diameters (cm)] with successful pregnancy. The associations were estimated as odds ratio (OR) with the respective 95% confidence intervals (CI). A two-sided p value < 0.05 was considered statistically significant. The optimal cut-off for fibroid size for the ability to achieve a pregnancy was calculated using receiver-operator characteristic (ROC) curve and was defined at the cut-off value optimizing sensitivity and specificity. For missing data, no data imputation was performed. All outcome data were available for all participants. All statistical analyses were performed using SPSS version 28.0.
This study was approved by the local ethics committee (EK 1271/2023) and conducted in accordance with the Declarations of Helsinki. The graphical abstract was created using PowerPoint by Microsoft Office 365, version 2406.
Results
A total of 80 women with a median age of 34.6 years (IQR, 31.4–37.8) and a median BMI of 23.7 kg/m^2^ (IQR, 21.7–27.5) were included in the study. About half of women (52.5%, n = 42) had primary infertility. Forty-six women (57.5%) had exactly one fibroid, 26.3% (n = 21) had two fibroids, and 16% (n = 13) had three fibroids. Laparoscopy was performed in the majority of patients (63.7%, n = 51), whereas 36.3% (n = 29) of patients underwent laparotomy.
Overall, 45.0% (n = 36) of women spontaneously achieved clinical pregnancy at a median of 4 months (IQR, 3–7) after the postoperative period, in which pregnancy was not permitted. In a binary logistic regression model (Table 1), the following two parameters were significantly associated with clinical pregnancy in the univariable and the multivariable model: patient age (adjusted OR 0.718, 95% CI 0.608–0.849; p > 0.001) and the sum of fibroid size (OR 1.245, 95% CI 1.072–1.446; p = 0.004). BMI, type of infertility, type of surgery, and maximum fibroid size had no effect on the association.Table 1. Patient and fibroid characteristics and associations with clinical pregnancy estimated as odds ratio (OR) with 95% confidence intervalPregnancy achievedPregnancy not achievedUnivariate analysisAdjusted analysisn = 36n = 44Crude OR (95%CI)p valueAdjusted OR (95%CI)p valueAge (years), median (IQR))32.4 (28.1;35.6)36.7 (33.7;38.4)0.766 (0.667;0.880) < 0.0010.718 (0.608;0.849) < 0.001BMI (kg/m^2^), median (IQR)23.1 (20.6;25.4)24.4 (21.8;28.2)0.926 (0.817;1.050)0.230––Secondary infertility, n (%)14 (38.9)24 (54.5)0.530 (0.217;1.298)0.165––Laparotomy, n (%)16 (44.4)13 (29.5)1.908 (0.758;4.800)0.170––Number of fibroids, n (%)118 (50.0)28 (63.6)Reference0.472––211 (30.6)10 (22.7)1.711 (0.604;4.847)–37 (19.4)6 (13.6)1.185 (0.525;6.726)–Largest fibroid size (cm), median (IQR)6.3 (5.0;8.9)5.0 (4.0;8.0)1.175 (0.995;1.388)0.057––Sum of fibroid size (cm), median (IQR)8.5 (6.0;11.8)7.3 (4.1;9.0)1.152 (1.021;1.299)0.0211.245 (1.072;1.446)0.004
Since the sum of fibroid size was a significant parameter for clinical pregnancy, its optimized cut-off value was calculated. The according ROC curve is shown in Fig. 1. The maximum sum of sensitivity and specificity for pregnancy was at a sum of fibroid diameter of ≥ 5 cm (p = 0.008). Using this cut-off, the sensitivity was 94.4% (95% CI 81.3–99.3), whereas the specificity was 29.5% (95% CI 16.8–45.2). Thirty-four/65 patients with a sum of fibroid size ≥ 5 cm became pregnant (positive predictive value, PPV, 52.3%, 95% CI 39.6–98.3%), whereas thirteen/15 women with a sum of fibroid size < 5 cm did not achieve a pregnancy (negative predictive value, NPV, 86.7%, 95% CI 59.5–98.3%). The according Kaplan–Meier curve is shown in Fig. 2.Fig. 1ROC curve for the sum of fibroid size and clinical pregnancyFig. 2Kaplan–Meier curve for clinical pregnancy according to the sum of fibroid size (≥ 5 cm: gray line versus < 5 cm: blue line). Clinical pregnancy rates quadruples when removal of FIGO V and VI fibroids with a combined size greater than 5 cm compared to those with smaller fibroids
Discussion
We present a cohort of 80 infertile women of childbearing age, who underwent laparoscopy or laparotomy for the removal of subserosal FIGO V and VI fibroids. While postoperative pregnancy outcomes for submucosal FIGO 0–3 fibroids are well studied and clear treatment recommendations are available, there are limited data on pregnancy rates following surgical removal of subserosal fibroids. The prevailing literature suggests that fibroids that distort the cavity (classified as International Federation of Gynecology and Obstetrics [FIGO] types 0–3 [21]) have a greater impact on fertility, with surgical interventions mostly restoring fecundity [22]. For all other fibroids, however, there is controversy. The existing literature is imprecise, contradictory, and of low quality [23].
In our study cohort of infertile women with subserous FIGO 5 and 6 fibroids, we observed an unassisted pregnancy rate of 45% within 12 months after non-hysteroscopic surgery. The postoperative odds of clinical pregnancy were higher in younger women and in women with larger fibroids (Table 1). The significant association between increasing age and decreasing pregnancy rates is well known and in accordance with preexisting data [24, 25]. However, the fact that women with a higher sum of fibroid size were more likely to benefit from myomectomy in terms of clinical pregnancy rates seems relevant and rather new. Some data suggest that leiomyomas > 2.85 cm [13] and > 3.0 cm [12], respectively, negatively impact conception, whereas other studies report clinical significance only in fibroids exceeding 5 cm. In our patient population, the latter could be confirmed as the maximum sum of sensitivity and specificity for pregnancy was at a sum of fibroid diameter of ≥ 5 cm (p = 0.008). Finding optimal sensitivity and specificity through an ROC should not be interpreted as fibroids only of a fixed size having an impact (a threshold). In contrast, the larger they are, the more probable seems their negative effect. Taking these findings a step further, where enucleation of smaller fibroids did not restore fertility, one of the most important takeaways should be that thorough exploration for other superimposed etiologies for subfertility is critical when the combined fibroid diameter is < 5 cm, since fecundity is less likely to be restored through myomectomy. However, our clear, direct finding is that myomectomy should be considered when the combined fibroid size is ≥ 5 cm, because it quadruples fecundability relative to those having removal of smaller fibroids. Specifically, only 13.3% of patients with a sum of fibroid size < 5 cm achieved clinical pregnancy compared to 52.3% of patients with a sum of fibroid size ≥ 5 cm. Myomectomy for FIGO V and VI fibroids for infertility should be considered for women when the size exceeds 5 cm, even though future studies will hopefully provide additional insight.
Several limitations must be acknowledged. As is common to similar studies, we were unable to record the number of live births or miscarriages. With the goal being live birth and not just conception, future research ideally should capture live birth data. We should also acknowledge that the best metric for fibroid burden is volume or mass of fibroid removed. Neither of these parameters were available. In addition, the retrospective study design is susceptible to confounding potentially limiting generalizability. However, the currently available evidence on pregnancy rates after non-hysteroscopic surgery for subserosal fibroids is based exclusively on small observational studies that included heterogeneous patient populations, used non-standardized fibroid classifications, and described fibroids only vaguely (e.g., location, size, and number of fibroids). We lowered this heterogeneity for our sample by including only FIGO-V and FIGO-VI fibroids and excluding patients over 40 years of age, reducing the impact of oocyte aneuploidy as a superimposed ovarian factor.
Regarding study strengths, we determined the clinically relevant parameter “time to pregnancy”. Moreover, strict exclusion criteria were applied. All women/couples with other causes for sub-/infertility were excluded. Furthermore, most existing publications blur the mode of conception postoperatively. We report an unassisted pregnancy rate of 45% in our population. Last but not least, an advantage of our study is the homogeneity of fibroid location (FIGO V and FIGO VI) that supports clear clinical recommendations, where almost 50% of all infertile women aged 18–40 years became pregnant within 24 months following the surgical removal of FIGO V and FIGO VI fibroids via laparoscopy or laparotomy.
Conclusion
Women with a combined sum of fibroid diameters ≥ 5 cm are four times more likely to spontaneously conceive after myomectomy than similar women with smaller fibroids. These findings support a dose–response effect for how we look at fibroids, where the impact of pathology is likely probabilistic and on a continuum. Not only do the results support myomectomy for larger type V and VI fibroids, but also they speak to the importance of a more thorough workup for other factors in women with smaller type V and VI fibroids and otherwise unexplained infertility, since they are far less likely to benefit from surgical intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organization WH. Infertility 2024 [Available from: https://www.who.int/news-room/fact-sheets/detail/infertility. Accessed 30 Nov 2024