Femoral artery calcification predicts hip fracture in maintenance hemodialysis patients
Shun-Neng Hsu, Jhao-Jhuang Ding, Ping-Huang Tsai, Chia-Lin Yang, Chun-Liang Hsu, Yu-Juei Hsu

TL;DR
Femoral artery calcification is a strong predictor of hip fractures in hemodialysis patients and is linked to worse survival outcomes.
Contribution
This study identifies femoral artery calcification as an independent risk factor for hip fractures in hemodialysis patients.
Findings
Higher femoral artery calcification scores are associated with increased hip fracture risk in hemodialysis patients.
Femoral artery calcification remains a significant predictor of hip fractures even after adjusting for traditional risk factors.
Patients with higher femoral artery calcification scores and hip fractures have worse survival outcomes.
Abstract
Femoral artery calcification (FAC) is a significant predictor of hip fractures in hemodialysis patients. A higher FAC score is associated with increased fracture risk and poor survival outcomes. Identifying FAC through radiographic assessment may improve fracture risk stratification and clinical management in this high-risk population. Patients with end-stage renal disease (ESRD) on hemodialysis (HD) are at increased risk for vascular calcification (VC) and bone fractures. While previous studies have linked aortic calcification with hip fractures, the relationship between medium-caliber artery-femoral artery calcification (FAC) and fall-related hip fractures in HD patients remains unclear. We retrospectively analyzed 170 HD patients who experienced falls and sought treatment in the emergency department (ED) between 2007 and 2014. The FAC score, representing the severity of femoral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
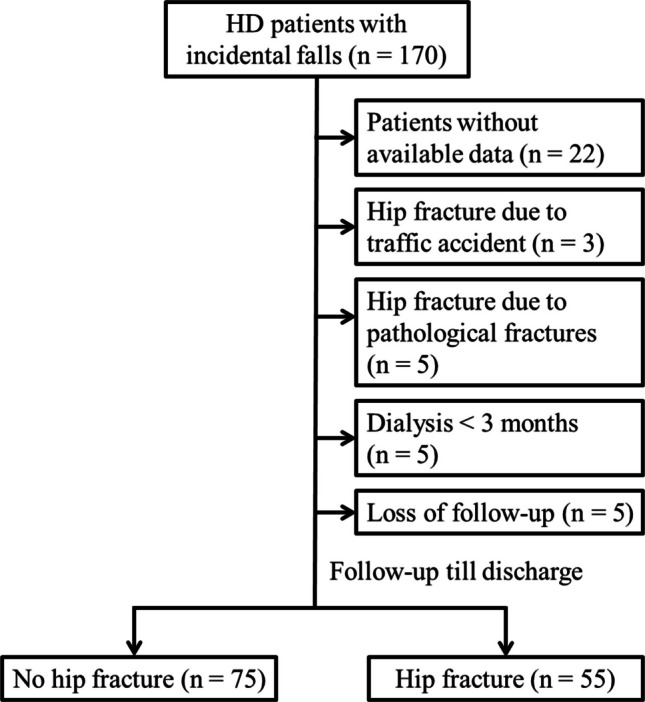 Figure 1
Figure 1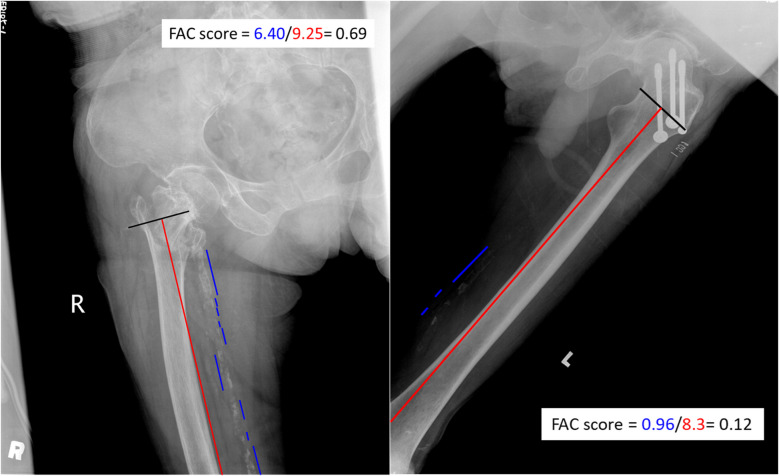 Figure 2
Figure 2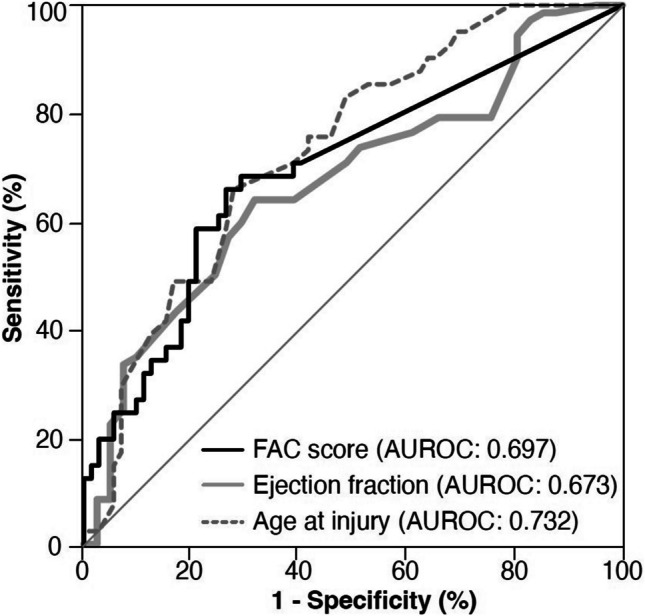 Figure 3
Figure 3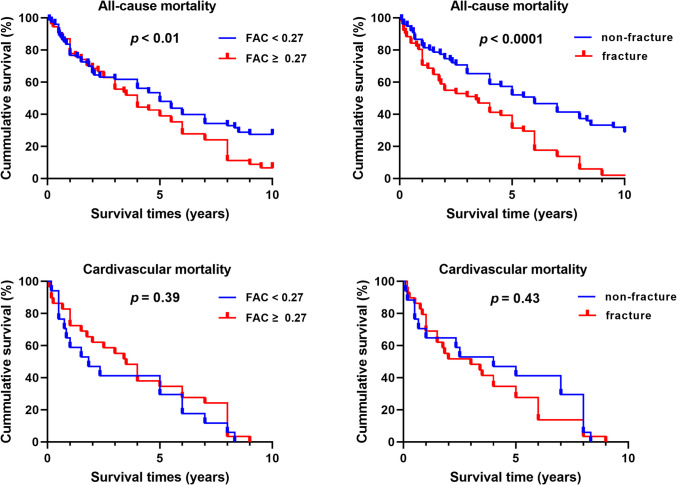 Figure 4
Figure 4- —http://dx.doi.org/10.13039/100007225Ministry of Science and Technology
- —http://dx.doi.org/10.13039/501100010425Tri-Service General Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Bone and Joint Diseases · Dialysis and Renal Disease Management
Introduction
Chronic kidney disease-mineral bone disorder (CKD-MBD) is a prevalent complication among CKD patients, especially those progressing to end-stage renal disease (ESRD) requiring dialysis. This condition encompasses a spectrum of clinical presentations involving vascular calcification (VC) and bone abnormalities, both of which increase the risk of fracture in CKD patients compared to the general population [1–3]. As expected, hip fractures in CKD patients are associated with substantial healthcare costs and increased mortality [4], underscoring the necessity to identify at-risk individuals and prevent fractures in this vulnerable population.
Emerging studies indicate that CKD patients share similar fracture risk factors with the general population but exhibit unique characteristics such as abnormal serum Pi levels, hyperparathyroidism, vitamin D deficiency, and elevated FGF-23 levels [5, 6]. VC, a hallmark of CKD-MBD, is associated with cardiovascular morbidity and mortality in ESRD patients and has been linked to an increased risk of fractures [7, 8]. Meta-analyses and observational studies in the general population have shown significant correlations between aortic calcification and skeletal fractures, as well as between coronary artery calcification (CAC) and hip fractures [9–12]. However, few studies have examined the link between VC and the risk of fractures in ESRD patients [13, 14]. One prospective study found aortic arch calcification predicted major fractures (hip, pelvis, humerus, proximal forearm, lower leg, or vertebrae) in dialysis patients [14], while another study observed a strong association between vertebral fractures and VC in medium-caliber arteries (femoral, uterine/spermatic, and radial) but no correlation with non-vertebral osteoporotic fractures [15]. Currently, the relationship between medium-caliber arterial VC and non-vertebral fractures remains under investigation.
In this study, we aimed to explore whether there is an association between femoral artery calcification (FAC) and the risk of hip fracture in hemodialysis (HD) patients. A simple calcification score of the femoral artery, which is the ratio of the total length of calcification plaques to the vessel length on plain radiographs of the hip and femur, was used to quantify FAC severity. Our study demonstrated that the FAC score predicts HD patients’ hip fracture risk independent of traditional risk factors.
Methods
Patient enrollment and group assignment
This study was performed at a single medical center in Northern Taiwan. The dialysis patients participating in this study consistently underwent maintenance HD at the same hospital. We conducted a retrospective analysis of the medical records of 170 HD patients who sustained falls and received treatment in the emergency department (ED) from January 2007 to December 2014. Plain X-rays of the pelvis or femur were employed to identify hip fractures, and only patients with femoral neck fractures and intertrochanteric hip fractures resulting from these falls were evaluated. All fractures analyzed in the study were low-trauma injuries, typically caused by falls from standing height or lower. Based on pelvic or hip radiographs, the HD patients were categorized into groups with hip and no hip fractures. This study aimed to investigate the risk factors for and impacts of FAC on hip fractures and the long-term clinical outcomes for up to 10 years after hip fractures in HD patients. This study was conducted in compliance with the Declaration of Helsinki. Data were collected from electronic medical records, and the study was approved by the Institutional Review Board of the Tri-Service General Hospital (TSGH), National Defense Medical Center, Taiwan (TSGHIRB No.: A202305066).
Inclusion and exclusion criteria
The inclusion criteria were as follows: (i) 20 years of age or older; (ii) ESRD on maintenance HD; (iii) a radiograph diagnosis with and without hip fracture; (iv) available clinical and laboratory data. The exclusion criteria were as follows: (i) fractures due to high-energy trauma (e.g., traffic accidents or falls from heights); (ii) pathological fractures caused by underlying malignancies, primary bone disorders, and metabolic bone diseases other than CKD-MBD; (iii) previous history of hip surgery; (iv) on HD for less than 3 months. A total of 130 patients with available demographics and laboratory data were enrolled (Fig. 1). Fig. 1. Flowchart depicting the selection process of hemodialysis patients without and with hip fractures
Demographic data and laboratory parameters
All relevant clinical data, including gender, age, duration of dialysis, comorbidities, and echocardiography data, were extracted from the medical records of all eligible subjects. The laboratory data collected during patient check-ups and admission for incident hip fractures included hemoglobin (Hb), serum creatinine (Cr), blood urea nitrogen (BUN), sodium (Na), potassium (K), total calcium (Ca), phosphorus (P), alkaline phosphatase (ALP), intact parathyroid hormone (iPTH), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and albumin levels. These parameters were measured by standard laboratory techniques using an automatic analyzer. Ejection fraction (EF) was assessed via transthoracic echocardiography during routine outpatient evaluations or hospital admissions. EF data were collected in the same year that the HD patients suffered falls. The treatment of hip fracture included intramedullary nailing, hemiarthroplasty, dynamic hip screw, or conservative therapies, and the choice of surgery depends on factors such as age, functional level, bone quality, and fracture type. All follow-up data and survival outcomes were acquired by a retrospective chart review during the study period.
Measurement of FAC scores in the hip region
All patients underwent posterior-anterior and lateral X-rays of the hip at the ED. These X-rays were interpreted by orthopedic physicians consulted in the ED, and all images were adequately qualified and of sufficient length for further assessment of the FAC score. The FAC score, representing the severity of femoral artery calcification, was calculated as the ratio of the total length of calcification plaques to the length of the femoral vessel visible on plain radiographs of the hip and femur. The femoral arteries were chosen for scoring because these arteries supplied the femoral head, intertrochanteric territory, and femoral diaphyseal shaft via the branched femoral nutrient artery (FNA) [16]. FAC scores were calculated using a standardized protocol and verified by another trained clinician to minimize intra- and inter-reader variability. The measurement was performed using the ImageJ software (Fiji package), as illustrated in Fig. 2. The FAC scores were expressed as the median and interquartile range (IQR), and the receiver operating characteristic (ROC) curve analysis was employed to determine the most predictive threshold for the FAC score. The threshold was established by identifying the value that maximized sensitivity and specificity, resulting in the maximum area under the curve (AUC). Fig. 2A representative radiographic image illustrates the measurement of the FAC score. The FAC score was calculated as the total length of calcification plaques divided by the length of the femoral vessel seen on plain radiographs
Statistical analyses
Data are presented as means ± standard deviation (SD) and percentages (%). Differences in study variables were analyzed using two-tailed unpaired Student’s t-tests or chi-square tests. Logistic regression models were used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) to assess the risk factors associated with hip fractures. Variables with p-values < 0.05 in the multivariate analysis were considered independent risk factors. The optimal threshold value for the FAC score was determined using the Youden index, a standard method for maximizing sensitivity and specificity. The ROC curve analysis identified 0.27 as the most predictive threshold for distinguishing patients at higher risk of hip fractures. Additionally, a ROC curve analysis was conducted to evaluate the predictive ability of each identified variable for hip fractures in HD patients. A retrospective Kaplan–Meier survival analysis was conducted to assess all-cause and cardiovascular mortality in patients with elevated FAC scores or hip fractures. Hazard ratios for survival were calculated by the Cox proportional hazards model. Statistical analysis was performed using IBM SPSS Statistics version 29.0, and significance was set at a* p*-value < 0.05.
Results
Baseline demographic characteristics in HD patients with and without fractures
A total of 130 HD patients who met the inclusion criteria were enrolled in the study. The study cohort consisted of 69 female participants (53%) and 61 male participants (47%), with an average age of 69.6 years (range 49 – 92). Among these patients, 75 individuals (58%), 95 individuals (74%), and 17 individuals (13%) were diagnosed with diabetes, hypertension, and cancer, respectively. Prior to enrollment, the average length of dialysis was 4.5 years, with a range of 0.4 to 27.0 years. FAC was present in around half of the study population (67/130, 52%). Ten percent of them (13/130, 10%) had an intertrochanteric hip fracture, while a third (42/130, 32%) suffered a femur neck fracture. The incidence rate of hip fractures among dialysis patients was calculated as 6.18 cases per 1000 person-years. The fracture group exhibited a higher proportion of females (69% vs. 41%, p < 0.01) and an advanced age (75.04 vs. 65.06 years, p < 0.0001) compared to the no-fracture group. However, no statistically significant differences were observed in the occurrence of chronic comorbidities or the duration of dialysis treatment between the two groups (Table 1). Table 1. Comparison of baseline demographics, clinical features, and laboratory data between no-hip fracture and hip fracture groupsVariableNo-fracture groupFracture groupp-valuen = 75n = 55Patient characteristicsGender < 0.01 Men, n (%)44 (59)17 (31) Women, n (%)31 (41)38 (69)Age, years65.56 ± 13.3875.04 ± 9.28 < 0.0001Duration on dialysis, years4.56 ± 3.324.38 ± 5.46NSHypertension, %8066NSDiabetes, %5758NSCancer, %918NSEchocardiographyEF, %62 ± 1055 ± 14 < 0.01PAP, mmHg37.32 ± 17.6440.00 ± 17.07NSFAC measurementFAC score (IQR)0.00 (0.00 – 0.40)0.47 (0.28 – 0.76) < 0.001Laboratory dataCr (mg/dL)8.60 ± 3.276.09 ± 2.90 < 0.0001Na (mEq/L)137.31 ± 2.96135.89 ± 4.23 < 0.05Ca (mg/dL)9.26 ± 0.929.00 ± 1.04NSP (mg/dL)4.96 ± 1.644.18 ± 1.75NSiPTH (pg/ml)438.62 ± 427.75291.21 ± 250.82NSALP (U/L)103.48 ± 98.3891.34 ± 48.97NSAST (U/L)20.25 ± 11.9626.42 ± 14.80 < 0.05Albumin (g/dL)3.79 ± 0.523.49 ± 0.59 < 0.001EF ejection fraction, PAP pulmonary artery pressure, FAC femoral artery calcification, Cr creatinine, Na sodium, Ca calcium, P phosphorus, iPTH intact parathyroid hormone, ALP alkaline phosphatase, AST aspartate aminotransferase
Comparative analysis of FAC scores and laboratory parameters
As shown in Table 1, the FAC score (0.47 [IQR, 0.28 – 0.76] vs. 0.00 [IQR, 0.00 – 0.40], p < 0.001) and serum AST level (26.42 vs. 20.25 U/L, p < 0.05) were significantly higher in the fracture group as compared to the no-fracture group. In contrast, the fracture group had a notable reduction in systolic ejection fraction ([EF], 55 vs. 62%, p < 0.01), along with decreased levels of serum Cr (6.09 vs. 8.60 mg/dL, p < 0.0001), Na (135.89 vs. 137.31 mEq/L, p < 0.05), and albumin (3.49 vs. 3.79 g/dL, p < 0.001). While there was no significant difference in the prevalence of diabetes between the fracture and no-fracture groups, it was observed that fracture patients with diabetes had the highest FAC score compared to both fracture patients without diabetes and no-fracture patients with or without diabetes (Supplementary Fig. 1).
Univariate and multivariate analysis on predictors for hip fracture in HD patients
Univariate analysis showed that female gender, age, EF, FAC score, Cr, Na, AST, and albumin were significantly associated with hip fracture. In the multivariate analysis, age (odds ratio [OR] per year, 1.116; 95% confidence interval [CI], 1.034 – 1.204, p < 0.01), EF (OR per 1% increase, 0.946; 95% CI, 0.898 – 0.997, p < 0.05), and FAC score (OR per 0.1 increment, 1.243; 95% CI, 1.015 – 1.524, p < 0.05) were identified as independent predictors of hip fractures (Table 2). Table 2. Univariate and multivariate logistic regression analysis of risk factors for incidental hip fracturesVariableUnivariableMultivariableOR95% CIp-valueOR95% CIp-valueGender, female3.1731.523 – 6.608 < 0.012.3070.603 – 8.832NSAge (year)1.0781.039 – 1.118 < 0.0011.1161.034 – 1.204 < 0.01EF (%)0.9510.918 – 0.984 < 0.010.9460.898 – 0.997 < 0.05FAC score (per 0.1)1.2161.083 – 1.366 < 0.0011.2431.015 – 1.524 < 0.05Cr (mg/dL)0.7650.671 – 0.873 < 0.0010.8190.619 – 1.085NSNa (mEq/L)0.8930.806 – 0.989 < 0.050.9030.755 – 1.080NSAST (U/L)1.0391.008 – 1.070 < 0.051.0150.972 – 1.060NSAlbumin (g/dL)0.3810.184 – 0.788 < 0.010.4830.140 – 1.667NS^*^The FAC score is unitless, calculated as the ratio of the total length of calcification plaques to the length of the femoral vessel visible on plain radiographs
The predictive performance of age, EF, and FAC score for hip fracture was assessed using ROC analysis. The resulting AUC values for age, EF, and FAC score were 0.732, 0.673, and 0.697, respectively. The cutoff value of 0.27 for the FAC score, identified through ROC curve analysis, provides a clinically meaningful threshold for stratifying hip fracture risk in HD patients, with a sensitivity of 75% and specificity of 82% (Fig. 3). Patients were subsequently categorized based on the cutoff value of the FAC score (0.27). Patients with FAC scores ≥ 0.27 had a significantly higher risk of hip fractures compared to those with FAC scores < 0.27. The OR for hip fractures in individuals with FAC ≥ 0.27 was 3.391 (95% CI: 1.635 – 7.032, p < 0.05). There were significant differences in the prevalence of diabetes (43 vs. 77%, p < 0.0001) and serum total calcium levels (9.10 mg/dL vs. 9.39 mg/dL, p < 0.05) among individuals with low and high FAC scores (Supplementary Table 1). Patients with a low FAC score (< 0.27) had a median survival time of 5 years, while those with a high FAC score (≥ 0.27) had a median survival time of 4 years (p < 0.01). The Kaplan–Meier survival analysis revealed a higher HR of 1.57 (95% CI: 1.04 – 2.37, p < 0.01, Fig. 4) for increased overall mortality in those with higher FAC scores. However, there was no statistically significant association between FAC score and cardiovascular mortality (HR, 95% CI: 0.29 – 0.95, p = 0.39). The median survival time for fracture and no-fracture patients after hip fracture was 3.4 and 6.0 years, respectively. Fracture patients had a twofold higher mortality risk than their no-fracture counterparts (HR 2.48, 95% CI: 1.60 – 3.85, p < 0.0001, Fig. 4). Fig. 3ROC curve analysis for the prediction of a hip fracture. ROC curves using three different parameters to predict hip fractures. The AUC for each color represents the overall performance of that parameter in predicting hip fracturesFig. 4Kaplan–Meier survival curves for all-cause and cardiovascular mortality in hemodialysis patients. Patients with FAC scores ≥ 0.27 had significantly lower cumulative survival for all-cause mortality (p < 0.01), but no significant difference was observed for cardiovascular mortality. Fracture patients showed significantly lower cumulative survival for all-cause mortality (p < 0.0001), while no significant difference was observed for cardiovascular mortality (p = 0.43)
Discussion
This study represents the first to investigate the relationship between FAC and hip fractures in HD patients. We identified a hip fracture incidence rate of 6.18 cases per 1000 person-years among dialysis patients, a rate consistent with previously reported findings [3, 17, 18]. Risk factors for hip fractures included female gender, advanced age, heart failure, FAC scores, and malnutrition. The multivariate-adjusted analyses revealed advanced age, reduced EF, and higher FAC scores as independent predictors of hip fracture risk. Additionally, both higher FAC scores and hip fractures exhibited independent correlations with poorer overall survival outcomes.
FAC, a common manifestation of VC, affected 40–70% of advanced CKD and dialysis patients. In this study, we established a significant association between FAC scores and hip fractures, even after controlling for confounding variables [19, 20]. Our results indicate that calcification in the abdominal aorta, carotid artery, coronary artery, and peripheral artery calcification (PAC) is associated with health outcomes [21]. In line with our observation, Szulc et al. reported that severe PAC is associated with a higher risk of acute coronary syndrome and major adverse cardiovascular events in older men [22]. Furthermore, HD patients with iliac artery calcifications are at high risk of vertebral fractures [23]. The mechanisms linking FAC and hip fractures remain incompletely elucidated; however, they likely involve ischemia-induced weakening of bone structure, contributing to diminished bone density by disrupting essential metabolic processes, including nutrient transport, waste removal, tissue repair, and bone remodeling [16, 24, 25]. These effects, compounded by systemic factors such as secondary hyperparathyroidism, mineral dysregulation, and malnutrition, can weaken bone integrity and elevate fracture risk [26, 27]. Additionally, previous studies have highlighted that vascular calcification, through its association with CKD-MBD, significantly alters bone metabolism and quality, as evidenced by localized mineralized bone loss in dialysis patients and its histomorphometric appraisal [28, 29]. This multifactorial interaction underscores the complexity of vascular and skeletal abnormalities in this patient population.
VC is a component of CKD-MBD, associated with disturbances in Pi and Ca homeostasis, as well as mineralotropic hormones like PTH, FGF23, and 1,25-dihydroxyvitamin D_3_ (1,25(OH)2_D_3). In addition to ischemia caused by VC, disturbed mineral metabolism in CKD patients may contribute to increased fracture susceptibility [30, 31]. Phosphorus accumulation begins in CKD Stage 3b, with hyperphosphatemia firmly linked to VC. High Pi exposure in vitro induces osteogenic transformation of vascular smooth muscle cells (VSMCs) via RUNX2 overexpression and mineral deposition [32]. Conversely, the knockdown of type III sodium‐dependent phosphate co-transporters (PiT 1) inhibits calcification and osteogenic markers. High Pi also stimulates matrix vesicle (MV) synthesis, oxidative stress, and mitochondrial dysfunction, all contributing to progressive VC [32]. Dialysis patients often develop hypercalcemia from high-Ca dialysate, vitamin D therapy, Ca-based Pi binders, and tertiary hyperparathyroidism, further promoting MV-mediated mineralization of VSMCs [33]. However, our study found comparable serum Pi and Ca levels in fracture and no-fracture groups, suggesting additional factors at play.
FGF23 and PTH decrease renal Pi reabsorption by downregulating the type IIa sodium-phosphate co-transporter expression in proximal tubules [34]. Previous studies have demonstrated that both hormones are associated with VC and fracture risk in CKD patients. The Longitudinal Aging Study Amsterdam reported a higher cardiovascular risk and abdominal aortic calcifications (AAC) in men with elevated serum PTH [35]. Another clinical trial found that nondialysis CKD patients exhibiting elevated AAC or pelvic arterial calcification scores presented with increased serum Pi and PTH [36]. In contrast, the role of increased FGF23 in VC progression is debatable. While some studies associate elevated FGF23 with aortic calcification [37, 38], others, such as the Chronic Renal Insufficiency Cohort (CRIC) study, found no association with CAC [39]. These clinical discrepancies are supported by some in vitro experiments. PTH-induced VSMC calcification involves apoptosis and endoplasmic reticulum stress via C/EBP Homologous Protein (CHOP) and Jun-N-terminal kinase (JNK) signaling [40]. In contrast, FGF23 may inhibit calcification through Wnt7b/β-catenin modulation [41]. Collectively, elevated PTH likely contributes to VC, heightening fracture risk; however, comparable PTH levels between fracture and non-fracture groups in our study suggest a negligible role of PTH in FAC and hip fractures.
Malnutrition is linked to frailty fractures and contributes to VC and bone fractures through the malnutrition-inflammation complex syndrome (MICS), which is prevalent in CKD and chronic heart failure (CHF). MICS affects 40–60% of HD patients, particularly those with elevated C-reactive protein (CRP) levels [42, 43]. Similarly, CHF patients exhibit high rates of inflammation and malnutrition [44–46]. Antioxidant deficiencies in malnourished CKD patients promote oxidative stress and inflammation, while proinflammatory cytokines accelerate protein degradation, malnutrition, and VC [47, 48]. In uremic rats, low dietary protein raised serum osteocalcin, a marker of high bone turnover and augmented arterial calcification [49]. Inflammatory cytokines (TNF-α, IL-1β, IL-6) initiate VC by upregulating BMP2 and downregulating SMα-actin expression [50–52]. These cytokines also accelerate bone resorption, linking MICS to fractures [53–56]. Consistent with these findings, we observed lower EF and serum albumin levels in HD patients with hip fractures and identified reduced EF as an independent fracture risk factor. These findings suggest that inflammations induced by lower EF and malnutrition are significant contributors to VC and bone fractures.
As VC is linked to increased cardiovascular events and mortality [15, 57], the Kidney Disease Improving Global Outcome (KDIGO) study group recommends VC screening in CKD patients using lateral abdominal radiography or CT [58]. Plain X-rays are a simple, widely used tool, with various grading systems predicting adverse CKD outcomes [59–61]. In this study, we introduced a FAC scoring system based on calcification plaque length relative to vessel length in plain hip radiographs. This score significantly differed between the fracture and no-fracture groups, correlating with increased fracture risk and mortality. Kaplan–Meier survival analysis revealed a mortality HR of 1.57 for patients with higher FAC scores (> 0.27), aligning with prior studies [36, 57, 62, 63]. These findings suggest that FAC is an important factor for hip fractures in dialysis patients, warranting further research to confirm and clarify underlying mechanisms.
Limitations
This study has several limitations that should be acknowledged. First, its retrospective nature and the relatively small sample size from a single medical institution may introduce biases and uncontrolled confounding variables. Second, we did not assess proinflammatory cytokines or hormones such as FGF23 and 25-hydroxyvitamin D (25-OHD) levels, which are known to influence VC and fracture risk. Third, the lack of detailed treatment data regarding the use of active vitamin D analogs or calcimimetics and the absence of bone biopsies restrict our ability to determine the precise bone turnover status or the specific causes of fractures. Fourth, we only calculated FAC scores and did not analyze calcification in other major arteries, assess sarcopenia status, or account for patients’ medications, which may affect hip fracture events in vulnerable dialysis patients. Fifth, the FAC score is significantly correlated with overall mortality, underscoring its clinical relevance. The insignificance of cardiovascular mortality may be attributed to several factors, such as the limited sample size for cardiovascular death events and the complex nature of mortality among dialysis patients. Sixth, the performance of FAC may restrict its efficacy as a standalone predictor and incorporating additional markers or composite models is essential to improve predictive accuracy.
Conclusion
In summary, our findings suggest that the FAC score is a key factor linked to an increased risk of hip fractures and mortality in dialysis patients. Further investigations are warranted to elucidate the underlying mechanisms and explore whether interventions targeting FAC could enhance bone health and overall outcomes in this high-risk population.
Supplementary Information
Below is the link to the electronic supplementary material.
ESM 1(PNG 903 KB)High Resolution Image (TIF 5.97 MB)
ESM 2(DOCX 15.4 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duang S, Zhang M, Liu C, Dong Q (2022) Parathyroid hormone-induced vascular smooth muscle cells calcification by endoplasmic reticulum stress. J Physiol Pharmacol 73(5). 10.26402/jpp.2022.5.0310.26402/jpp.2022.5.0336942806 · doi ↗ · pubmed ↗
- 2Bellasi A, Di Lullo L, Russo D, Ciarcia R, Magnocavallo M, Lavalle C, Ratti C, Fusaro M, Cozzolino M, Di Iorio BR (2021) Predictive value of measures of vascular calcification burden and progression for risk of death in incident to dialysis patients. J Clin Med 10(3):376. 10.3390/jcm 1003037610.3390/jcm 10030376 PMC 786391833498192 · doi ↗ · pubmed ↗
- 3Ohtake T, Mitomo A, Yamano M et al (2023) Impact of arterial calcification of the lower limbs on long-term clinical outcomes in patients on hemodialysis. J Clin Med 12(4):1299. 10.3390/jcm 1204129910.3390/jcm 12041299 PMC 996785936835836 · doi ↗ · pubmed ↗