Enteroscopic direct drainage for submucosal intestinal juice leakage due to afferent loop syndrome in Roux-en-Y anatomy
Mitsuru Okuno, Tsuyoshi Mukai, Fumiya Kataoka, Hiroshi Araki, Eiichi Tomita, Hisataka Moriwaki, Masahito Shimizu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
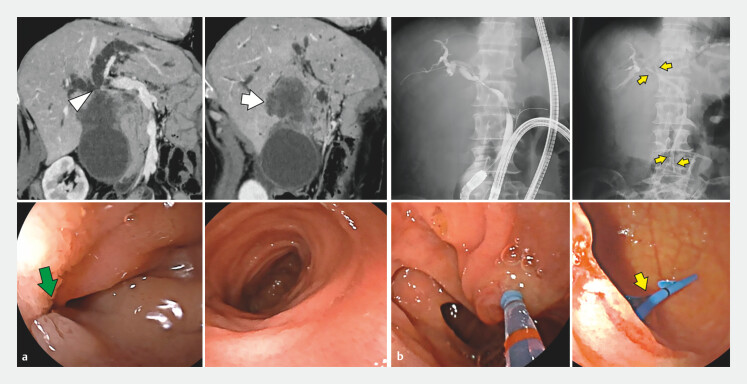 Fig. 1
Fig. 1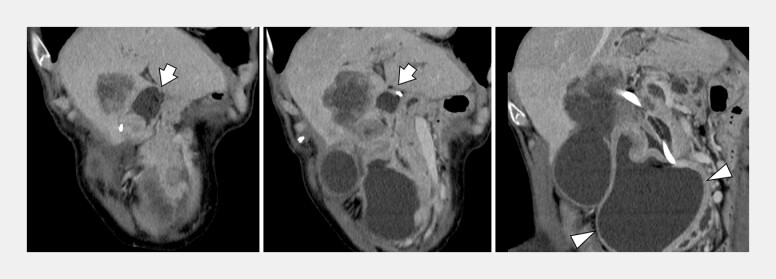 Fig. 2
Fig. 2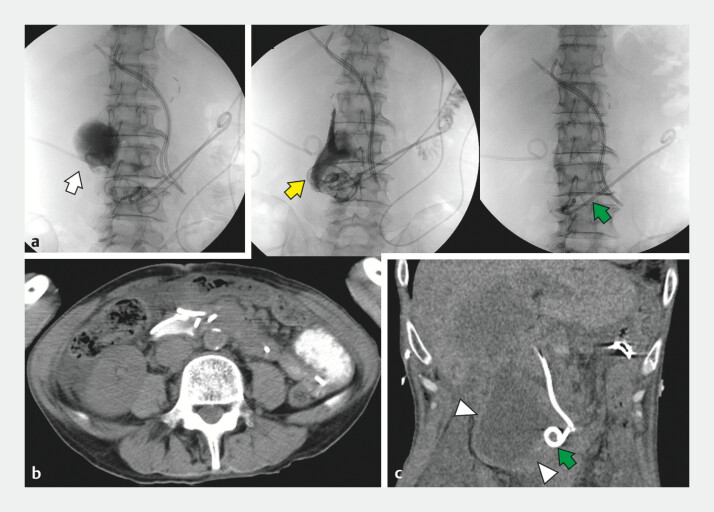 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastrointestinal disorders and treatments · Gastroesophageal reflux and treatments
We report a case of intestinal fluid accumulation secondary to afferent loop syndrome, successfully treated via enteroscopic submucosal drainage.
A 66-year-old man with a history of gastric resection and Roux-en-Y reconstruction for gastric cancer 6 years earlier presented with fever. Computed tomography (CT) revealed liver metastasis invading the bile duct near the duodenal end loop ( Fig. 1 ). Enteroscopy confirmed tumor invasion near the end loop of the duodenum, with no additional intestinal abnormalities. Suspecting cholangitis, bilateral biliary plastic stent (PS) drainage was performed using an enteroscope (EI-580BT; Fujifilm, Tokyo, Japan), and the patient was discharged after clinical improvement.
a Computed tomography reveals a liver metastasis (arrow) with invasion to the bile duct (arrowhead) in a patient with Roux-en-Y reconstruction. Enteroscopy shows tumor invasion near the duodenal end loop (green arrow) without other intestinal abnormalities. b Bilateral biliary plastic stent drainage (yellow arrow) was performed under enteroscopic guidance.
Three weeks later, he developed abdominal pain. CT revealed a distended end loop and submucosal expansion in the horizontal part of the duodenum ( Fig. 2 ), suggesting leakage of accumulated intestinal fluid from the end-loop cavity into the duodenal submucosal space. Endoscopic ultrasound failed to access the site. Therefore, an enteroscope was used, and the tensed mucosa was punctured with a precut needle knife, with the elasticity of the mucosal surface assessed prior to entry. A 6-mm dilation balloon was used to expand the puncture tract, and both 7-Fr PS and 6-Fr drainage tubes were placed in the fluid collection cavity. One week later, fluoroscopy confirmed collapse of the fluid collection, and the 6-Fr tube was removed ( Video 1 ).
Computed tomography shows a tensed end loop (arrow) and expansion of the submucosal space in the horizontal part of the duodenum (arrowhead).
Massive submucosal fluid collection in the duodenum was drained using a precut needle knife under enteroscopy in a case of afferent loop syndrome with Roux-en-Y anatomy.Video 1
Although endoscopic ultrasound-guided gastroenterostomy is a safe option for afferent loop syndrome, as it allows the evaluation of blood vessels and needle access to the afferent limb 1 2 3 , access was limited in this case due to Roux-en-Y anatomy. Direct enteroscopic puncture poses a perforation risk but was safely performed with mucosal elasticity assessment. Fluid accumulated after drainage tube removal, though the patient remained asymptomatic, with partial drainage via the remaining 7-Fr PS ( Fig. 3 ).
a PTGBD (arrow) is performed. No communication was observed between the gallbladder and the duodenal submucosal cavity. b Fluoroscopy and computed tomography demonstrate collapse of the fluid collection. After which, the 6-Fr drainage tube (yellow arrow) was removed. c Following drainage tube removal, fluid retention reappeared (arrowhead), although the patient remained asymptomatic. It was considered that intestinal juice continued to drain partially through the remaining 7-Fr plastic stent (green arrow). PTGBD: percutaneous transhepatic gallbladder drainage.
Endoscopy_UCTN_Code_TTT_1AP_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tanikawa T Urata N Ishii K Afferent-Loop Syndrome Treated with Endoscopic Ultrasound-Guided Drainage of the Afferent Loop with a Plastic Stent Case Rep Gastroenterol 20221612212810.1159/00052201935528775 PMC 9035941 · doi ↗ · pubmed ↗
- 2Shiomi H Sakai A Nakano R Endoscopic Ultrasound-Guided Gastroenterostomy for Afferent Loop Syndrome Clin Endosc 20215481081710.5946/ce.2021.23434775697 PMC 8652169 · doi ↗ · pubmed ↗
- 3Matsubara S Takahashi S Takahara N Endoscopic Ultrasound-Guided Gastrojejunostomy for Malignant Afferent Loop Syndrome Using a Fully Covered Metal Stent: A Multicenter Experience J Clin Med 20231210.3390/jcm 12103524 PMC 1021955237240629 · doi ↗ · pubmed ↗