Endoscopic ultrasound-guided cyanoacrylate injection for the treatment of gastric variceal bleeding after failed endoscopic embolization
Lu Yang, Zhuang Kangmin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
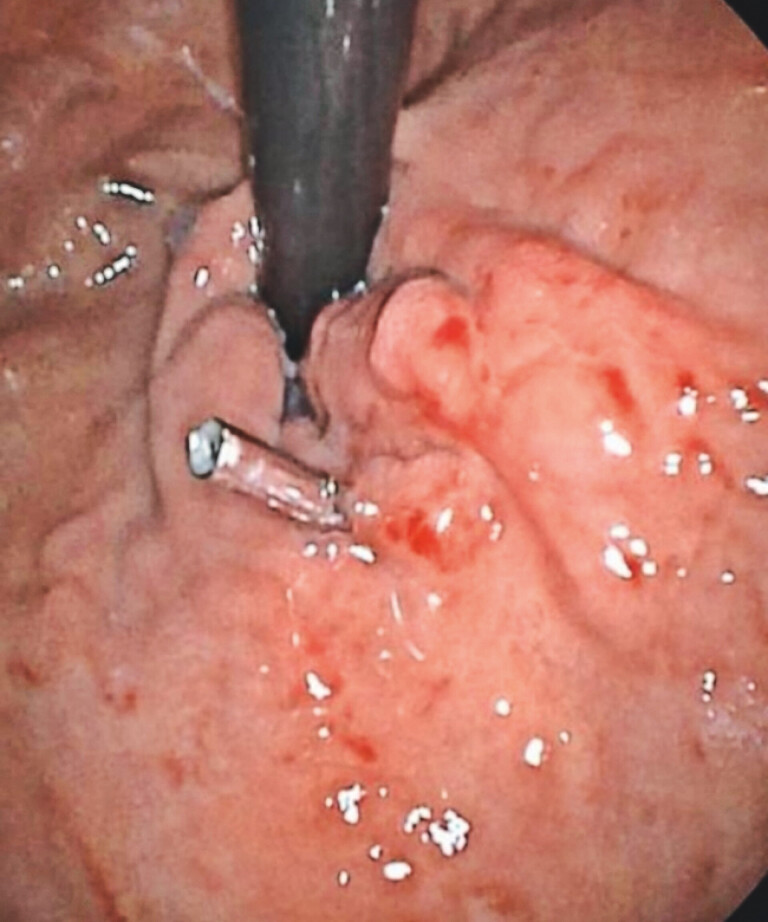 Fig. 1
Fig. 1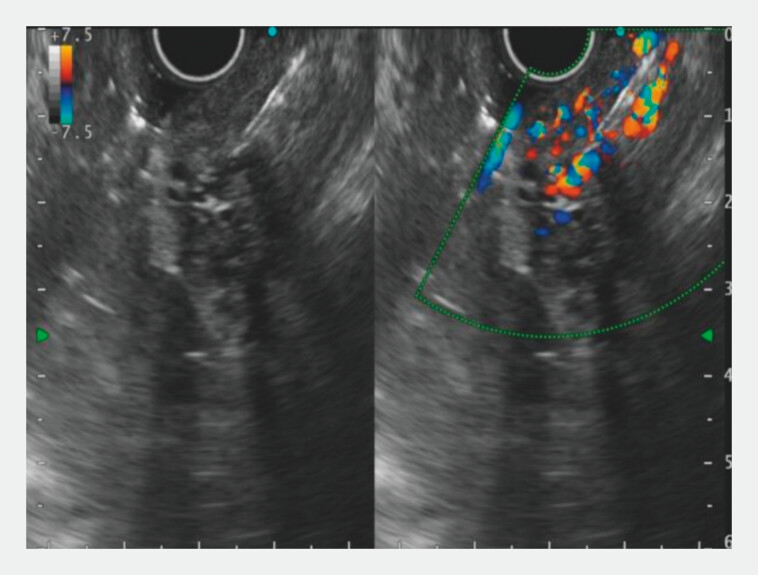 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Liver Disease Diagnosis and Treatment · Organ Transplantation Techniques and Outcomes
Gastric variceal (GV) hemorrhage is one of the most life-threatening adverse events in cirrhotic patients with portal hypertension, with an annual incidence of 5–15% 1 . Although less common than esophageal variceal bleeding, GV bleeding is associated with higher severity and mortality, reaching a 6-week mortality rate of 20% 2 . Endoscopic cyanoacrylate (CYA) injection remains the standard treatment for GV bleeding. However, failure occurs in 15–30% of cases due to factors such as obscured deep perforating veins, inadequate glue dispersion, or vascular anatomical variations 3 . Endoscopic ultrasound-guided selective variceal devascularization (EUS-SVD) has emerged as a salvage therapy, offering real-time visualization of vascular structures and hemodynamics. While EUS-SVD is primarily used for prophylactic management, this case demonstrates its efficacy in achieving hemostasis after failed conventional endoscopic CYA injection.
A 49-year-old male with a history of hepatitis C-related cirrhosis (18 years) and prior GV bleeding treated with CYA injection in 2016 presented with hematemesis and melena. Laboratory tests revealed thrombocytopenia (platelets: 64 × 109/L; reference: 125–350 × 109/L). Abdominal CT confirmed cirrhosis, splenomegaly, and splenic vein collaterals. Endoscopy showed severe GOV1 type varices (The titanium clip was left in place during a previous endoscopy treatment at an external hospital) ( Fig. 1 ). Under general anesthesia, the patient underwent endoscopic gastric variceal obturation (GVO). Persistent active bleeding from the target vein was observed during the procedure ( Video 1 ). Conversion to EUS-guided intervention was performed. EUS identified a gastric fundal variceal cluster (8 mm diameter). Using a 19-G needle (COOK), the variceal vein at the greater curvature was punctured under Doppler guidance to avoid perforators, and 1.0 mL of CYA was injected ( Fig. 2 , Video 1 ). Post-procedural EUS confirmed cessation of blood flow, and follow-up endoscopy demonstrated complete variceal obliteration ( Video 1 ). The patient experienced no complications (e.g., fever, embolism) and was discharged on day 3. No rebleeding occurred during the 6-month follow-up.
Endoscopic view of type 1 gastroesophageal varices in accordance with the Sarin classification.
Endoscopic ultrasonography (EUS) with color Doppler evaluation of blood flow in gastric varices and EUS-guided injection of cyanoacrylate.
Endoscopic ultrasound (EUS)-guided intervention for active bleeding following endoscopic treatment.Video 1
GV bleeding remains a critical challenge in cirrhotic patients. While endoscopic CYA injection is first-line therapy, failure rates necessitate alternative approaches. Nonendoscopic options include transjugular intrahepatic portosystemic shunt and balloon-occluded retrograde transvenous obliteration 4 . However, advancements in endoscopic techniques, such as EUS-guided glue embolization (EUS-GE), offer minimally invasive solutions with high efficacy.
In this case, EUS-GE succeeded where conventional endoscopy failed, likely due to enhanced visualization of the variceal architecture, including the feeding artery (left gastric vein branch) and drainage vein (gastrorenal shunt). A retrospective study by Bhat et al. 5 (n = 152) reported a 98% immediate hemostasis rate and 8% 1-year rebleeding rate with EUS-GE, outperforming traditional GVO (25–35% rebleeding). Coil-assisted embolization was not utilized here due to the varices’ moderate caliber.
This case underscores its safety and feasibility in acute settings, aligning with literature supporting its role in managing complex variceal anatomy.
Endoscopy_UCTN_Code_TTT_1AO_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Garcia-Tsao G Abraldes JG Berzigotti A Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liverdiseases Hepatology 20176531033527786365 10.1002/hep.28906 · doi ↗ · pubmed ↗
- 2Weilert F Shah JN Marson FPEUS-guided coil and glue for bleeding rectal varix Gastrointest Endosc 20127691591622172480 10.1016/j.gie.2011.09.027 · doi ↗ · pubmed ↗
- 3García-Pagán JC Caca K Bureau C Early TIPS (Transjugular Intrahepatic Portosystemic Shunt) Cooperative Study Group. Early use of TIPS in patients with cirrhosis and variceal bleeding N Engl J Med 20103622370237920573925 10.1056/NEJ Moa 0910102 · doi ↗ · pubmed ↗
- 4Goral VYılmaz N Current approaches to the treatment of gastric varices: glue, coil application, TIPS, and BRTO Medicina (Kaunas)20195533531277322 10.3390/medicina 55070335 PMC 6681371 · doi ↗ · pubmed ↗
- 5Bhat YM Weilert F Fredrick RTEUS-guided treatment of gastric fundal varices with combined injection of coils and cyanoacrylate glue: a large U.S. experience (with video)Gastrointest Endosc 2016831164117226452992 10.1016/j.gie.2015.09.040 · doi ↗ · pubmed ↗