Rarer than rare: managing an epiphrenic diverticulum in achalasia
Giovanni Aldinio, Caterina Pelligra, Laura Cini, Marina Coletta, Beatrice Marinoni, Matteo Porta, Gian Eugenio Tontini

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
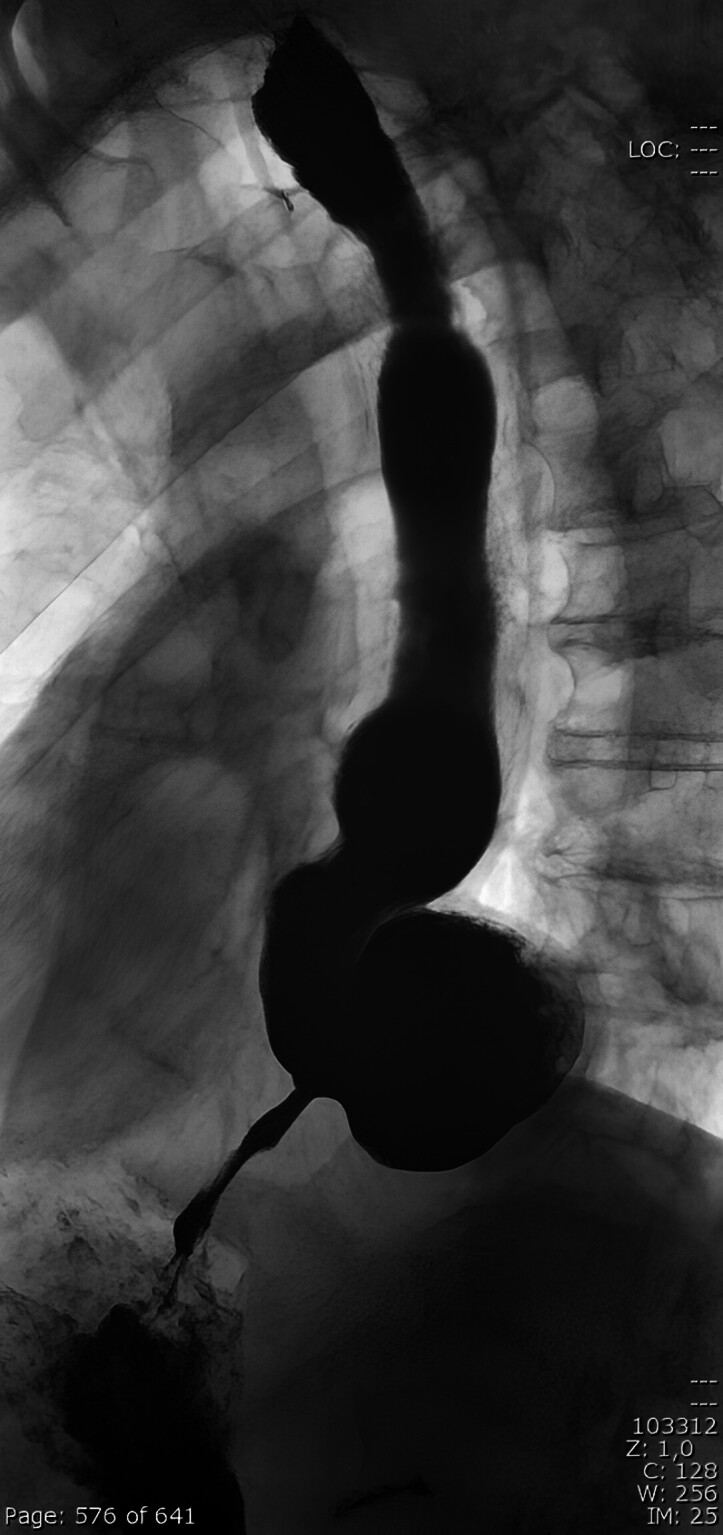 Fig. 1
Fig. 1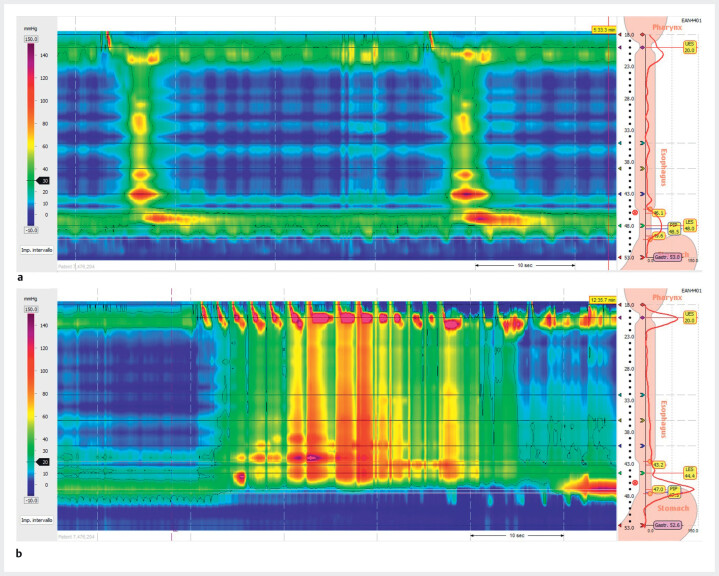 Fig. 2
Fig. 2 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Dysphagia Assessment and Management · Esophageal and GI Pathology
An epiphrenic diverticulum is an extraordinarily rare condition, occurring in approximately 1 per 500.000 people per year 1 . It is often associated with esophageal motility disorders (achalasia in 60% of cases) and, when large (i.e. >5 cm), undoubtedly causes symptoms such as dysphagia, regurgitation, weight loss, and aspiration pneumonia 1 2 . Malignant transformation, mostly into squamous cell carcinoma, occurs in about 0.6% of cases 3 . When a symptomatic diverticulum is associated with a motility disorder, subsequent management must address both conditions: minimally invasive surgery usually includes resection of the diverticulum, myotomy of the lower esophageal sphincter (LES), and an antireflux procedure 3 .
A 77-year-old man presented to the emergency room with progressive dysphagia and food regurgitation. Following two unsuccessful esophagogastroduodenoscopy (EGD) attempts at another hospital, a barium esophagogram showed a dilated esophagus with a prominent diverticulum above the LES ( Fig. 1 ). An EGD was eventually completed, revealing a markedly dilated, atonic esophagus filled with partially digested food, and a large epiphrenic diverticulum ( Video 1 ). The esophagogastric junction was passed with slight resistance using a 11.6-mm wide, high definition gastroscope (Pentax EG34-i10). A “Contents, Anatomy, Resistance, and Stasis” (CARS) score of 7 was highly suggestive of achalasia 4 . Type II achalasia was diagnosed via high resolution manometry (HRM), according to Chicago classification 4.0 ( Fig. 2 ).
Initial barium esophagogram showing a dilated esophagus with a prominent diverticulum above the lower esophageal sphincter.
High resolution manometry showing the absence of lower esophageal sphincter (LES) relaxation ( a : single swallow, integrated relaxation pressure [IRP] = 32.5 mmHg; b : rapid drink challenge, IRP = 36.5 mmHg), with concomitant esophageal panpressurizations , which is compatible with type II achalasia.
Type II achalasia and a large epiphrenic diverticulum were diagnosed on barium esophagogram, esophagogastroduodenoscopy, high resolution manometry, and computed tomography before the patient underwent laparoscopic diverticulectomy, Heller myotomy, and Dor fundoplication.Video 1
A preoperative abdominal computed tomography scan confirmed dilatation of the proximal and mid esophagus and a 6 × 5-cm diverticulum ( Video 1 ). The patient underwent laparoscopic transhiatal diverticulectomy, Heller myotomy, and Dor fundoplication under intraoperative endoscopic guidance. No perioperative complications occurred. Histology was subsequently negative for malignancy. A postoperative contrast esophagogram showed no leaks and good transit, allowing oral feeding and discharge within a week. At 3-month follow-up, a barium esophagogram confirmed normal passage of barium and resolution of the diverticulum ( Fig. 3 ).
Repeat barium esophagogram at 3-month follow-up showing normal passage of barium and resolution of the diverticulum.
This case adds to the limited literature documenting epiphrenic diverticula in patients with achalasia, and their management 5 . A comprehensive diagnostic workup and a tailored surgical approach addressing both the diverticulum and the underlying motility disorder are essential to achieve optimal outcomes.
Endoscopy_UCTN_Code_CCL_1AB_2AC_3AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Constantin A Constantinoiu S Achim F Esophageal diverticula: from diagnosis to therapeutic management-narrative review J Thorac Dis 20231575977936910058 10.21037/jtd-22-861PMC 9992562 · doi ↗ · pubmed ↗
- 2Fisichella PM Jalilvand A Dobrowolsky A Achalasia and epiphrenic diverticulum World J Surg 2015391614161910.1007/s 00268-015-2950-725609118 · doi ↗ · pubmed ↗
- 3Zaninotto G Portale G Costantini M Therapeutic strategies for epiphrenic diverticula: systematic review World J Surg 2011351447145310.1007/s 00268-011-1065-z 21541802 · doi ↗ · pubmed ↗
- 4Ellison A Peller M Nguyen AD An endoscopic scoring system for achalasia: the CARS score Gastrointest Endosc 2024100417428038431105 10.1016/j.gie.2024.02.020 · doi ↗ · pubmed ↗
- 5Okamoto K Kinoshita J Saito H Simultaneous laparoscopic surgery for esophageal achalasia combined with epiphrenic diverticulum: a case report Surg Tech Dev 202413245250