Secondary Versus Recurrent Central Nervous System Lymphoma: Evaluating the Similarities and Differences in a Single-Institution Cohort
Danielle A Bazer, Melanie Schweitzer, Ewa Zabrocka, Agnieszka Kowalska

TL;DR
This study compares two types of brain lymphoma to identify differences in symptoms, treatment, and outcomes, aiming to improve diagnosis and care.
Contribution
The paper provides a detailed comparison of clinical features and outcomes between RPCNSL and SCNSL in a small patient cohort.
Findings
RPCNSL lesions were solitary in frontal or temporal lobes, while SCNSL lesions were multifocal in two of three patients.
Altered mental status was a common symptom in both RPCNSL and SCNSL patients.
All RPCNSL patients eventually transitioned to hospice care, highlighting poor outcomes in this group.
Abstract
Background: Primary central nervous system lymphoma (PCNSL) is a rare malignancy that affects only a small number of individuals. A subset of these cases may later relapse as recurrent central nervous system lymphoma (RPCNSL), while systemic lymphomas may progress to secondary central nervous system lymphoma (SCNSL). Although these entities differ in origin, they often present with overlapping clinical and radiologic features, complicating diagnosis and management. Objective: This study aims to compare the clinical presentations, treatment histories, lesion characteristics, and outcomes of patients with RPCNSL and SCNSL in a single-institution cohort in an attempt to identify key distinguishing features and shared patterns. Improved understanding of these similarities and differences may enhance diagnostic accuracy, guide treatment strategies, and inform surveillance approaches.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
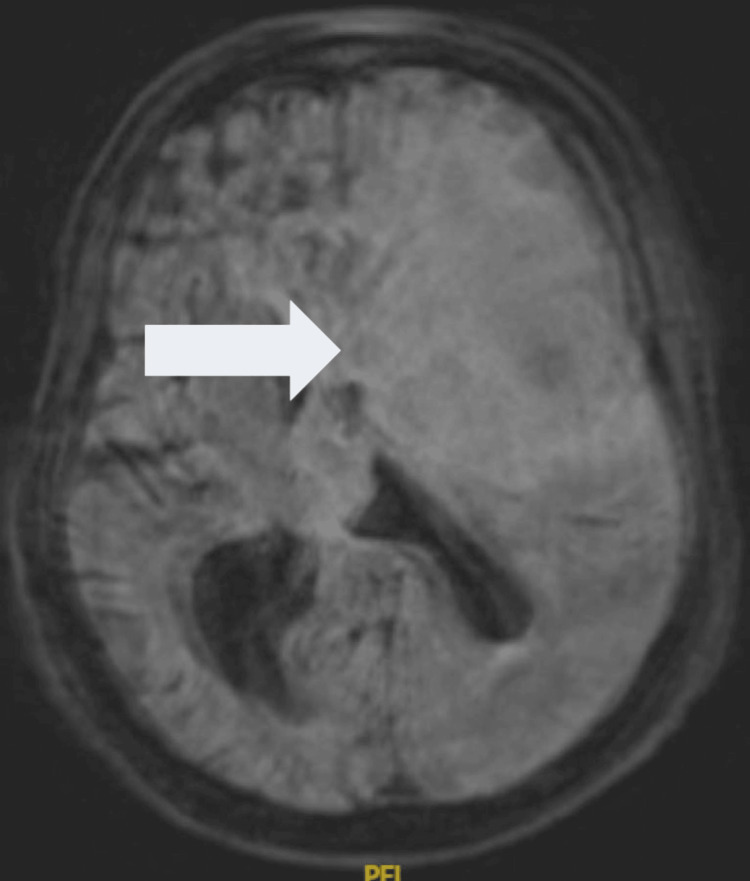 Figure 1
Figure 1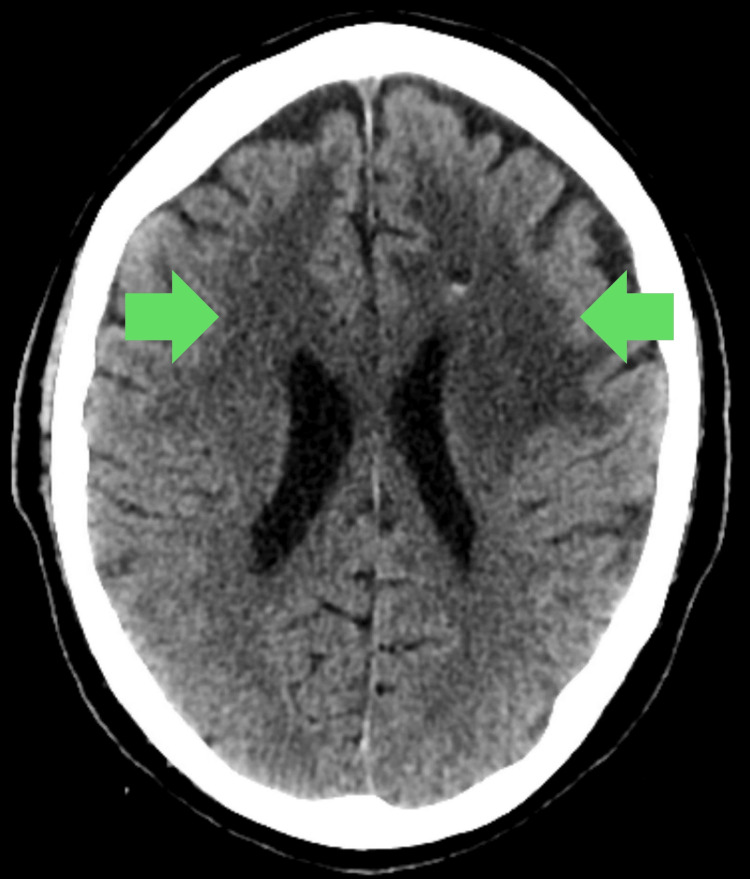 Figure 2
Figure 2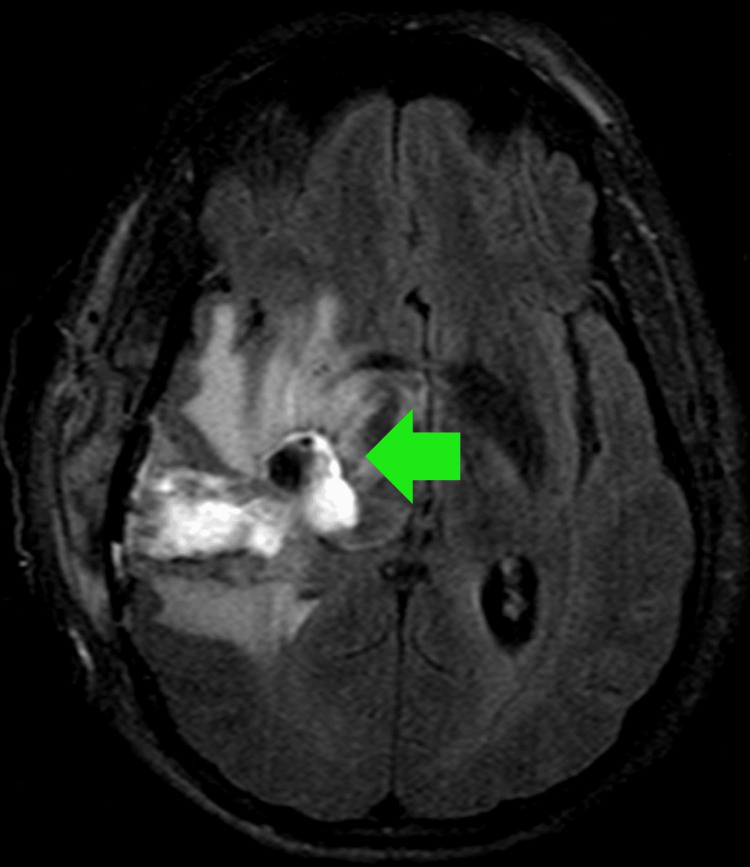 Figure 3
Figure 3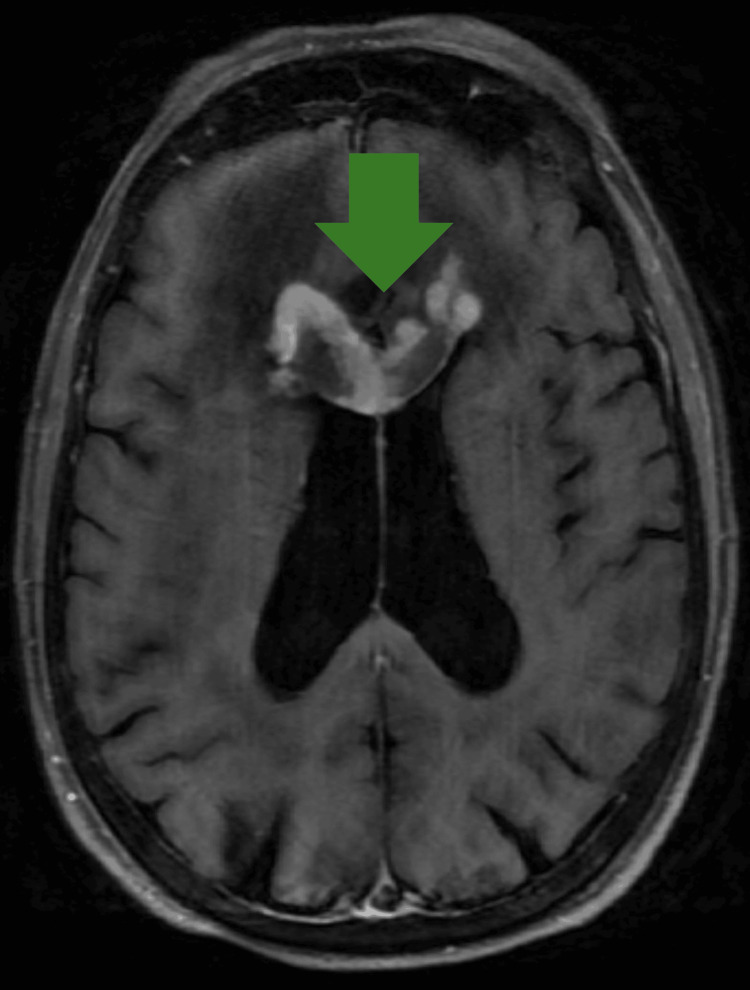 Figure 4
Figure 4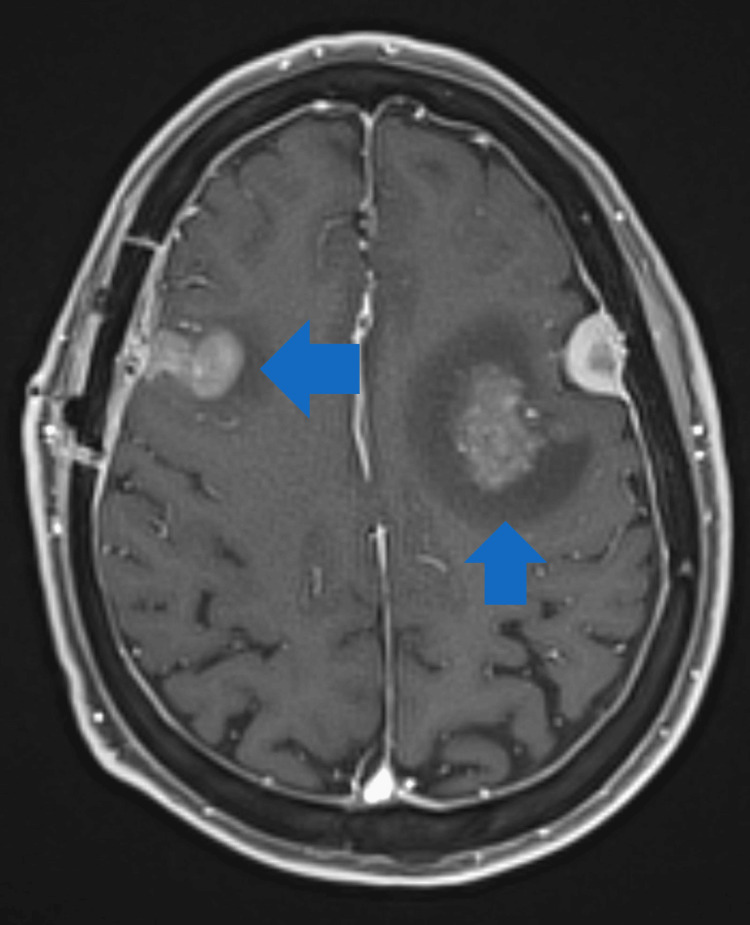 Figure 5
Figure 5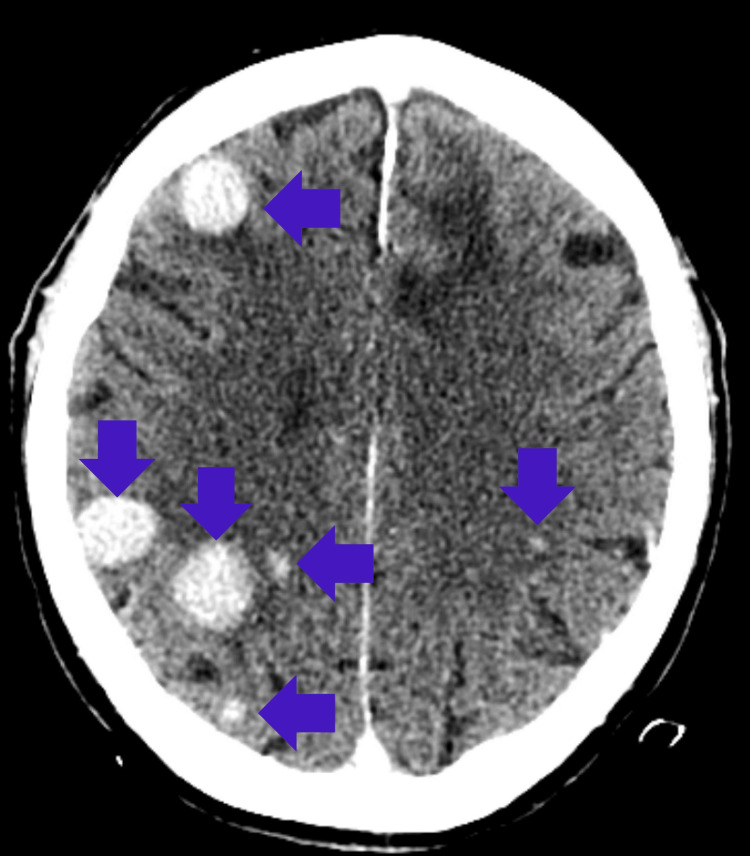 Figure 6
Figure 6| Patient # | Sex | SCNSL or RPCNSL? | Age at Initial Presentation | Age at Recurrence/ Secondary Presentation | Presenting Symptom for RCNSL/SCNSL | Imaging at Presentation of SCNSL/RCNSL | Prior Cancer History | Treatment Received at Initial Presentation | Treatment Received at Recurrence/ Secondary Presentation | Outcome (Months) |
| 1 | M | RPCNSL | 71 | 71 | AMS, gait ataxia | MRI without contrast: Large heterogeneous, centrally necrotic mass with restricted diffusion, centered in the left frontal lobe and basal ganglia. Extensive surrounding vasogenic edema and mass effect with sulcal effacement. Extension into the lateral ventricles, involving the body and genu of the corpus callosum. Rightward midline shift (15 mm) with subfalcine herniation. | PCNSL | Steroids | R-MVP | PFS=14; OS=15 |
| 2 | M | RPCNSL | 56 | 66 | AMS, frequent falls, left arm weakness, urinary incontinence | CT without contrast: Infiltrative low-attenuation foci in the bilateral frontal lobes and centrum semiovale, extending across the corpus callosum. | PCNSL | R-CHOP and radiation | Rituximab, HD-MTX, cytarabine | PFS=129; OS=137 |
| 3 | M | RPCNSL | 61 | 63 | AMS, personality changes, right-sided weakness | CT with contrast: Marked solid enhancement in the right medial temporal region with surrounding vasogenic edema. Two small, ill-defined central and left hypodense foci. Compression of the right lateral ventricle and brainstem with leftward midline shift. | PCNSL | DeAngelis Protocol | Rituximab, TMZ, cytarabine | PFS=23; OS=28 |
| 4 | F | SCNSL | 77 | 81 | AMS, starring spells | MRI with and without contrast: Extensive FLAIR hyperintensity in bilateral frontal lobes with heterogeneous enhancement and expansion of the genu and proximal body of the corpus callosum. Mass effect on the lateral ventricle. Ring-enhancing lesion in the right frontal lobe abutting the right lateral ventricle. Multiple homogeneously enhancing lesions in the left frontal lobe (largest 1.1 cm), also involving the corpus callosum. | DLBCL | Stereotactic radiation | Steroids, rituximab | PFS=unknown; outcome: lost to follow-up |
| 5 | M | SCNSL | 65 | 67 | Asymptomatic | MRI with and without contrast: Left frontal lobe mass with surrounding edema. Similar mass in the right frontal lobe with surrounding hemosiderin ring, edema, and overlying burr hole (biopsy site). Additional mass in the right occipital lobe and a smaller lesion in the left frontal lobe. Left frontal extra-axial, dural-based lesion. Associated local mass effect. | DLBCL | DA-EPOCH-R, R-CVP | DeAngelis Protocol | PFS=12; outcome= lost to follow-up |
| 6 | M | SCNSL | 76 | 80 | AMS, gait ataxia | CT with and without contrast: Numerous hyperdense mass lesions in bilateral cerebral hemispheres with homogeneous enhancement, consistent with lymphoma metastases. Partial effacement of the left frontal horn. | Atypical CLL variant with 17p deletion | Ibrutinib, bendamustine, rituximab, idelalisib. R-CVP | HD-MTX | PFS=12; outcome= lost to follow-up |
| Variable | RCNSL | SCNSL |
| Number of Patients | 3 | 3 |
| Gender | 2/3 male, 1/3 female | 3/3 male |
| Race | 3/3 Caucasian | 3/3 Caucasian |
| Median Age of Initial Presentation | 63 years | 67 years |
| Median Age of Secondary Presentation | 73 years | 76 years |
| Primary Cancer | PCNSL | 2/3 DLBCL with renal involvement; 1/3 atypical CLL variant with 17 q deletion |
| Primary Cancer Treatment at Recurrence | R-MVP; rituximab-methotrexate-cytarabine; rituximab-temozolomide-cyclophosphamide | Rituximab; DeAngelis Protocol, high-dose methotrexate |
| MRI Findings at Recurrence | 3/3 with single lesions localized to the frontal and temporal lobes | 2/3 had multiple lesions in the frontal, parietal, temporal, and occipital lobes. 1 patient had a single lesion in the genu of the corpus callosum |
| Presentation at Recurrence | 3/3 AMS | 2/3 AMS, 1/3 asymptomatic |
| Outcome | 3/3 deceased | 3/3 lost to follow-up |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCNS Lymphoma Diagnosis and Treatment · Glioma Diagnosis and Treatment · Lymphoma Diagnosis and Treatment
Introduction
Although rare, primary central nervous system lymphoma (PCNSL) affects 0.5 per 100,000 individuals [1,2]. It is estimated that 5% cases will develop into secondary central nervous system lymphoma (SCNSL) and 2-5% will evolve into recurrent central nervous system lymphoma (RPCNSL) with the diffuse large B-cell lymphoma (DLBCL) variant of RPCNSL [3,4]. With the adrenal involvement, relapse rates as high as 40% have been reported [3,4]. The incidence of both SCNSL and RPCNSL is increasing, and the prognosis of these patients remains poor despite advances in systemic therapy; it is anticipated that patients with SCNSL will die within a few months of the diagnosis [5,6].
The use of rituximab-based therapy has decreased the risk of central nervous system (CNS) recurrence, and common modalities for CNS prophylaxis include intrathecal methotrexate (with or without cytarabine and/or hydrocortisone) or intravenous high-dose methotrexate [4]. However, once a patient has developed SCNSL, there is a paucity of consensus guidelines due to a lack of randomized clinical trial data, prompting clinicians to rely on retrospective data and phase II studies [7].
The goal of this study was to compare clinical presentation, imaging characteristics, treatment regimens, and outcomes to identify distinguishing patterns between RPCNSL and SCNSL. We attempted to characterize early differentiators that may guide diagnosis, risk stratification, and treatment selection.
This abstract was presented at the Society for Neuro-Oncology Annual Meeting in November 2022.
Materials and methods
Study design
This is a retrospective case series that relied on chart review to identify appropriate participants; the chart review commenced after institutional review board approval. All study participants were treated at our University Hospital between 2010 and 2020. The participant cases were divided based on RPCNSL, SCNSL, and PCNSL. We narrowed our inclusion criteria to include patients living with RPCNSL and SCNSL.
Inclusion and exclusion criteria
This study included patients with SCNSL and RPCNSL, DLBCL subtype. Our study required patients to be greater than 18 years of age. Patients were evaluated at our hospital from the years 2010-2020. It was mandatory that the patients have their initial MRI, work-up, and treatment plan established at our institution.
This study excluded patients with primary CNS lymphoma. Patients who developed CNS lymphoma as a complication of human immunodeficiency virus (HIV) were excluded from this study. Patients who were also Epstein-Barr virus (EBV) positive were excluded from this study as well. We excluded individuals who had their initial treatment and/or work-up at an outside institution.
Data collection
Patients were identified using the key terms “CNS lymphoma,” “secondary CNS lymphoma,” and “recurrent primary CNS lymphoma” as well as the ICD-10 codes associated with such diagnoses. The electronic medical record was also queried to include patients greater than 18 years of age from the years 2010-2020. Investigators then reviewed the generated list of patients and went through the individual patient charts to determine if the patients were appropriate for study inclusion.
Statistical analysis
Descriptive statistics were used to interpret the data. Variables included age of primary malignancy diagnosis, age of secondary malignancy diagnosis, initial treatment for PCNSL, presenting symptoms, location of the tumor, and outcomes. The investigators performed the descriptive statistical analyses.
Ethics statement
This study was approved by the university’s institutional review board in 2021 and received the following IRB number: IRB2021-00200. Written consent was waived by the institutional review board. The study complies with the Declaration of Helsinki.
Results
Our series contained six patients, 3/6 with SCNSL and 3/6 with RPCNSL. All RPCNSL patients were male. In the SCNSL cohort, 2/3 were male. All patients in the study were Caucasian, HIV negative, and EBV negative. The average age at diagnosis of the first malignancy in patients with RPCNSL was 63 years (range, 56-71; median, 61 years), and the age at recurrence was 67 years (range, 63-71; median, 66 years). In SCNSL, the average age at initial diagnosis was 73 years (range, 65-77; median, 76 years), and the average age at secondary presentation was 76 years (range, 67-81; median, 80 years).
Initial PCNSL treatments for RPCSNL were steroids, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) with radiation, and DeAngelis Protocol (methotrexate, leucovorin, vincristine, procarbazine, whole brain radiation, dexamethasone, and cytarabine).
Initial malignancies for patients with SCNSL were DLBCL with renal involvement in two patients and atypical chronic lymphocytic leukemia (CLL) variant with 17p deletion in the remaining patient. The initial treatments for the patients who had DLBCL with renal involvement were stereotactic radiation as well as DA-EPOCH-R (dose-reduced etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) and R-CVP (rituximab, cyclophosphamide, vincristine, and prednisone). The patient with atypical CLL variant with 17p deletion was initially treated with ibrutinib, bendamustine, rituximab, and idelalisib, followed by R-CVP.
All patients with RPCNSL presented with altered mental status and 2/3 SCNSL patients were altered upon presentation; one SCNSL patient was asymptomatic. The lesions within the RPCNSL cohort were all singular lesions, localized to the frontal and temporal lobes (Figures 1-3). Within the SCNSL cohort, 2/3 patients had multiple lesions in the frontal, parietal, temporal, and occipital lobes, whereas 1 patient had a single lesion in the genu of the corpus callosum (Figure 4-6).
MRI of the brain of patient 1 with RPCNSLThere is a large, heterogeneous, centrally necrotic mass in the left frontal lobe and basal ganglia region, with extensive surrounding vasogenic edema and mass effect causing effacement of the sulci. The mass extends into the lateral ventricles and involves the body and genu of the corpus callosum.RPCNSL = recurrent central nervous system lymphoma
Head CT of patient 2 with RPCNSLLow-attenuation foci are present in the bilateral frontal lobes and centrum semiovale, crossing the midline.RPCNSL = recurrent central nervous system lymphoma
T2/FLAIR MRI of the brain in patient 3 with RPCNSLA heterogeneous mass is present in the medial temporal lobe, with surrounding vasogenic edema.RPCNSL = recurrent central nervous system lymphoma
T1-weighted post-contrast MRI of the brain in patient 1 with SCNSLThere is an enhancing lesion of the right genu of the corpus callosum.SCNSL = secondary central nervous system lymphoma
T1-weighted post-contrast MRI of the brain in patient 2 with SCNSLIt shows a left posterior frontal lobe lesion involving the precentral gyrus, as well as a right frontal lobe lesion with a surrounding hemosiderin ring and associated vasogenic edema.SCNSL = secondary central nervous system lymphoma
Contrast-enhanced head CT of patient 3 with SCNSLThere are numerous hyperdense mass lesions in the bilateral cerebral hemispheres with contrast enhancement. SCNSL = secondary central nervous system lymphoma
At recurrence, patients with PCNSL were treated with R-MVP (rituximab, methotrexate, procarbazine, vincristine); rituximab, methotrexate, and cytarabine; and rituximab, temozolomide, and cytarabine. The patients with SCNSL were treated with steroids and rituximab, DeAngelis Protocol, and high-dose methotrexate. The history and treatment course of all six patients are summarized in Table 1.
All of the RPCNSL patients were ultimately transitioned to palliative care and all of the SCNSL patients were lost to follow-up (Table 2).
Discussion
Despite limited case numbers, comparative data on SCNSL and RPCNSL are sparse. This case series is an attempt at a side-by-side comparison of these two rare CNS lymphoma presentations from a single institution, highlighting potential distinguishing features in clinical course, imaging, and outcomes that may aid in diagnostic and therapeutic decision-making.
Although differing in etiology, there are shared features among SCNSL and RPCNSL. In our cohort, five out of six patients presented with altered mental status. The majority (~75%) of RPCNSL patients are symptomatic at the time of relapse, with the most common symptoms including gait disorder, cognitive impairment, sensorimotor disorder, and balance issues [8]. The presentation is similar in the case of SCNSL [9]. Most relapses are confined to the central nervous system; however, a small number of relapses are isolated systemic relapses, and clinical symptoms occur early and vary. Although treatment is similar for both RPCNSL and SCNSL, the prognosis for RPCNSL is very poor [10,11].
The RPCNSL lesions were all singular and localized to the frontal and temporal lobes for our cohort. The lesions in the SCNSL cohort were more variable with 2/3 patients having multiple lesions and 1/3 patients having a single lesion in the corpus callosum. This is consistent with the work of Malikova et al., showing the presence of multiple lesions at the SCNSL diagnosis in over half of the patients [12]. Although SCNSL has been shown to present with leptomeningeal disease in 2/3 of patients, we have not observed it in our series [13,14]. This points to the heterogeneity of presentations, which illuminates a potential diagnostic challenge.
Although the literature delineates that rituximab-based therapy can decrease the risk of CNS recurrence in PCNSL patients [4], only two out of three patients with RPCNSL received a rituximab-based therapy as part of their initial regimen. Of the patients that received rituximab-based therapy for PCNSL, only one patient received CNS prophylaxis with methotrexate, which may contribute, in part, to why there was recurrent disease in the CNS. Yet, at recurrence, all patients received rituximab-based therapy for RPCNSL. Two out of three of the patients also received methotrexate, yet only one patient received both methotrexate and cytarabine in combination.
Similar to the diverse presentation of SCNSL, there was greater variety in the treatments delivered at initial presentation as well as at the time of secondary presentation. Our cohort is consistent with the current literature identifying that there is a predilection for genitourinary involvement [3,4]. In our cohort, among the patients with DLBCL and renal involvement, one was treated with systemic therapies (DA-EPOCH-R and R-CVP), while the other received stereotactic radiotherapy. The patient living with atypical CLL variant with 17p deletion also received R-CVP after pretreatment with ibrutinib, bendamustine, rituximab, and idelalisib. Similar to the RPCNSL cohort, two patients received a rituximab-based therapy for their initial cancer diagnosis. None of the patients with SCNSL received methotrexate as part of their initial cancer regimen. At the time of secondary presentation, only 1 patient was treated with a rituximab-based therapy, whereas the remaining 2 patients were treated with the DeAngelis Protocol and high-dose methotrexate.
In our cohort for both RPCNSL and SCNSL, the median progression-free survival (PFS) was 14 months. The median PFS for the RPCNSL cohort was 23 months and 12 months for the SCNSL. The median overall survival was challenging to calculate, as all patients with SCNSL were lost to follow-up. Of the patients with RPCNSL, the mean overall survival was 28 months. Unfortunately, our cohort is consistent with the current literature describing the high rate of mortality at recurrence/secondary progression [5,6]. These data highlight the immense need to develop better evidence-based treatments to improve the survival of patients living with both SCNSL and RPCNSL.
Although our case series is small, it contributes to our greater understanding of both RPCNSL and SCNSL. It offers a direct clinical comparison between RPCNSL and SCNSL, identifying trends such as lesion multiplicity, symptom presentation, and treatment heterogeneity. Notably, all patients with RPCNSL had solitary lesions and uniformly poor outcomes, while SCNSL cases were more variable in both lesion distribution and response to treatment. These observations may support earlier recognition and tailored management strategies in future clinical practice or research.
There are some limitations to our study. The small sample size and limited follow-up data, due to the retrospective nature of this study, limit our ability to confidently generalize the results. Nevertheless, considering the rarity of RPCNSL and SCNSL diagnoses, and taking into account the paucity of large, prospective clinical studies investigating the nature of these diseases [11,15], we believe that our study is a valuable addition to the fund of knowledge on these entities.
Conclusions
Despite the small sample size, our study highlights several key distinctions between RPCNSL and SCNSL. First, our study reveals a male and geriatric predominance for both RPCNSL as well as SCNSL. For the RPCNSL cohort, lesions were singular in all cases, whereas for SCNSL, the tumors had a predilection to be multifocal. All of the patients with RCNSL were transitioned to hospice. Thus, a high level of suspicion for a diagnosis of RPCNSL should be raised if there is a geriatric male patient with a history of primary CNS lymphoma with subsequent brain imaging suggesting a solitary lesion.
Unfortunately, our sample size is quite small; however, the trends we have identified can be hypothesis-generating and can guide further prospective, multi-institutional research that is much needed to better characterize prognostic factors, guide treatment decisions, and ultimately improve survival for patients with SCNSL and RPCNSL.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary CNS lymphoma J Clin Oncol Batchelor T Loeffler JS 128112882420061652518310.1200/JCO.2005.04.8819 · doi ↗ · pubmed ↗
- 2The changing incidence of primary central nervous system lymphoma is driven primarily by the changing incidence in young and middle-aged men and differs from time trends in systemic diffuse large B-cell non-Hodgkin's lymphoma Am J Hematol O'Neill BP Decker PA Tieu C Cerhan JR 99710008820132387380410.1002/ajh.23551 PMC 4020348 · doi ↗ · pubmed ↗
- 3Secondary CNS relapse in diffuse large B-cell lymphoma: defining high-risk patients and optimization of prophylaxis strategies Hematology Am Soc Hematol Educ Program Savage KJ 578586201720172922230710.1182/asheducation-2017.1.578PMC 6142549 · doi ↗ · pubmed ↗
- 4Extranodal diffuse large B cell lymphoma: molecular features, prognosis, and risk of central nervous system recurrence Curr Treat Options Oncol Ollila TA Olszewski AJ 381920182993160510.1007/s 11864-018-0555-8PMC 6294323 · doi ↗ · pubmed ↗
- 5Natural history of CNS relapse in patients with aggressive non-Hodgkin's lymphoma: a 20-year follow-up analysis of SWOG 8516—the Southwest Oncology Group J Clin Oncol Bernstein SH Unger JM Leblanc M Friedberg J Miller TP Fisher RI 1141192720091904728910.1200/JCO.2008.16.8021 PMC 4879698 · doi ↗ · pubmed ↗
- 6Treatment strategies, outcomes and prognostic factors in 291 patients with secondary CNS involvement by diffuse large B-cell lymphoma Eur J Cancer El-Galaly TC Cheah CY Bendtsen MD 57689320182947710210.1016/j.ejca.2018.01.073PMC 5869165 · doi ↗ · pubmed ↗
- 7Prevention and management of secondary central nervous system lymphoma Haematologica Bobillo S Khwaja J Ferreri AJ Cwynarski K 67368910820233638424610.3324/haematol.2022.281457 PMC 9973486 · doi ↗ · pubmed ↗
- 8Primary CNS lymphoma at first relapse/progression: characteristics, management, and outcome of 256 patients from the French LOC network Neuro Oncol Langner-Lemercier S Houillier C Soussain C 129713031820162695138210.1093/neuonc/now 033PMC 4998995 · doi ↗ · pubmed ↗