Angiosarcoma of the Liver: A Radiological Alarm for Radiologists and Hepato-Pancreato-Biliary (HPB) Surgeons
Evangelia Florou, Archana Abarnadevikarthikeyan, Stephen M Gregory, Parthi Srinivasan, Andreas Prachalias

TL;DR
Hepatic angiosarcoma is a rare, aggressive liver cancer that often mimics benign conditions on imaging, leading to late diagnosis and poor outcomes.
Contribution
The paper highlights the diagnostic challenges of hepatic angiosarcoma through two case studies emphasizing the importance of early detection and clinician awareness.
Findings
Radiological features of hepatic angiosarcoma can mimic benign liver cysts and cavernous haemangiomas.
Late diagnosis is common due to rapid clinical deterioration and misleading imaging findings.
Complete surgical resection offers better outcomes, but treatment options are limited in most cases.
Abstract
Hepatic angiosarcoma (HA) is a rare and aggressive malignancy. Radiological findings are non-specific and often mimic benign liver pathologies. Patients’ rapid clinical deterioration is often alarming, leading clinicians to a late, futile diagnosis. We present two cases of HA in which presenting symptoms, but more importantly, radiological appearances, were misleading, mimicking liver cysts and cavernous haemangiomas, respectively. Rapid clinical deterioration and speedy radiological evolution of disease spread led to a diagnosis of HA with a dismal prognosis. A 77-year-old male was diagnosed with an incidental finding of a cystic lesion in the upper abdomen. On contrast-enhanced computed tomography (CECT), the lesion mimicked a complex liver cyst with atypical radiological features, prompting clinicians to treat it with surgical resection for an otherwise unclear malignant pathology.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
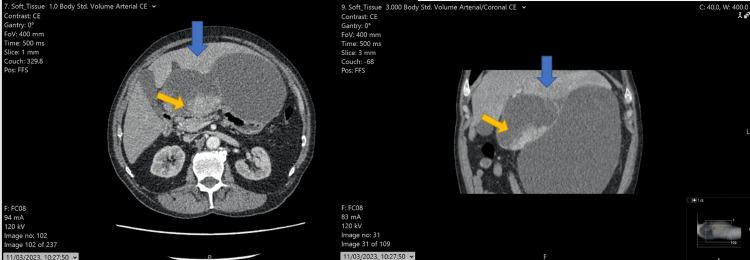 Figure 1
Figure 1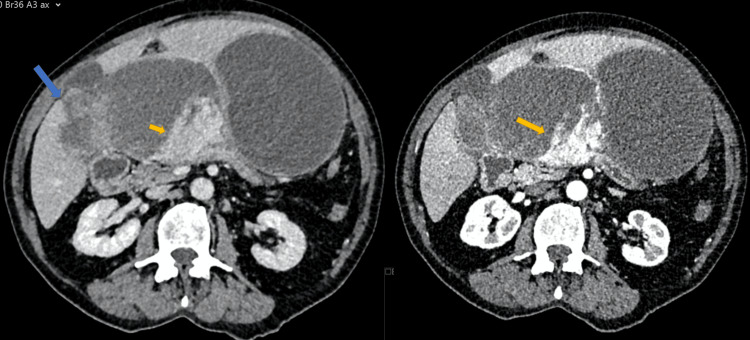 Figure 2
Figure 2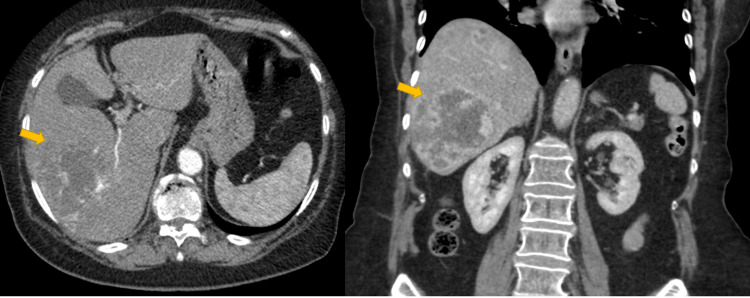 Figure 3
Figure 3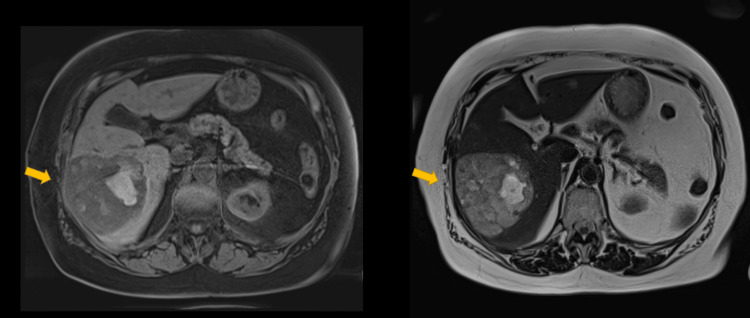 Figure 4
Figure 4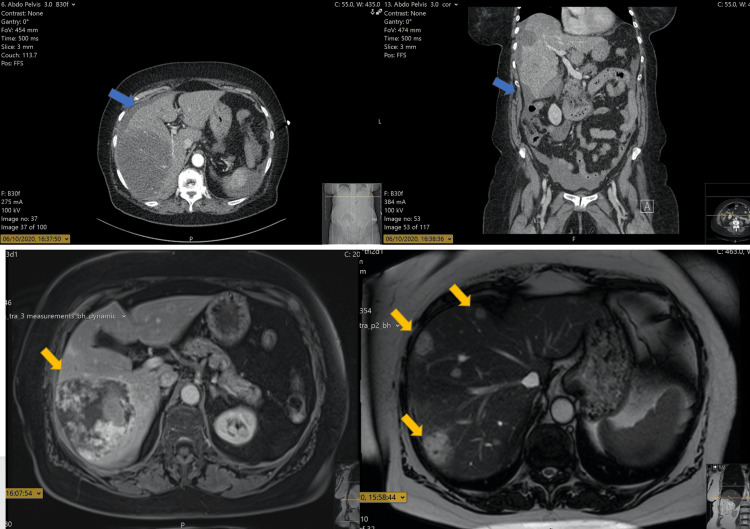 Figure 5
Figure 5| Feature | Hepatic Angiosarcoma (HA) | Cavernous Hemangioma | Simple Liver Cyst | Biliary Cystadenoma |
| Echogenicity (US) | Heterogeneous / mixed echogenicity | Homogeneously hyperechoic | Anechoic with posterior enhancement | Anechoic or septated, may have mural nodules |
| CT (Non-contrast) | Hypodense or mixed attenuation; may contain hemorrhage | Hypodense | Water attenuation (<20 HU) | Cystic lesion, often septated, ± calcifications |
| CT (Arterial phase) | Irregular peripheral or nodular enhancement, rapid washout | Peripheral nodular enhancement (classic) | No enhancement | Septal or mural enhancement |
| CT (Portal/venous phase) | Washout of enhancement, progression of necrosis | Progressive centripetal fill-in | No enhancement | Persistent enhancement in septa/nodules |
| MRI T1-weighted | Heterogeneous, possibly hyperintense (hemorrhage) | Hypointense | Hypointense | Variable: low-to-intermediate signal |
| MRI T2-weighted | Heterogeneous, high signal with areas of necrosis | Markedly hyperintense | Brightly hyperintense | Hyperintense with septations |
| Contrast-enhanced MRI | Early irregular enhancement with washout | Peripheral nodular enhancement with fill-in | No enhancement | Septal/mural nodular enhancement |
| Growth | Rapid progression between studies | Stable over time | Stable | Slow-growing, can increase gradually |
| Associated findings | Hemorrhage, necrosis, invasion, multifocality | None | None | May have biliary ductal dilation or compression |
| Clinical correlation | Often symptomatic, rapid deterioration | Incidental, asymptomatic | Incidental | May present with mass effect or vague symptoms |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Cardiac tumors and thrombi · Vascular Malformations and Hemangiomas
Introduction
Hepatic angiosarcoma (HA) is a rare primary liver malignancy, which accounts for only 1-2% of all primary liver malignancies [1-3] and 2% of all sarcomas [1,3]. It affects patients in the sixth decade of life [3,4], and some risk factors, such as former exposure to Thorotrast [5,6], vinyl chloride [7,8], and arsenic compounds [9], have been identified in 25-40%, but in the majority of the cases, no risk factor is identified [3].
HA is not easy to diagnose, as patients are often asymptomatic [1,3]. Symptomatic presentation occurs in 9% of the cases, with non-specific symptoms such as abdominal pain and discomfort, which may be late signs of metastatic disease [3]. Presentations with fulminant acute liver failure or intra-abdominal bleeding due to spontaneous tumour rupture have also been described, with the former being scantly documented in case reports [4,10] and the latter reported in 17-27% of the cases [3,11].
Histological confirmation may be challenging [1], as the tumour may be mimicking poorly differentiated carcinoma or undifferentiated sarcoma [1].
Surgical resection with negative margins is the only treatment with curative potential [3]. However, early diagnosis is quite rare, and the majority of the cases present with metastatic disease [3]. Systemic treatments do not offer improved prognosis, which remains dismal with a median overall survival of six months [3].
Radiologically, HA presents a diagnostic dilemma. Imaging features are often non-specific and may mimic benign hepatic lesions such as liver cysts or cavernous haemangiomas, leading to misinterpretation and delayed diagnosis. Furthermore, the rapid progression between imaging studies may be easily underestimated, masking the underlying malignant nature of the disease [2].
This article examines two cases of HA, underscoring the radiological diagnostic challenges that can arise in the absence of symptoms. In such cases, imaging techniques, typically considered as invaluable tools for early cancer detection, prove ineffective in diagnosing this aggressive and rare form of cancer.
Case presentation
Case 1
A 77-year-old male with a history of hypertension, bronchiectasis, and mild asthma was investigated for suspected lung cancer due to a persistent cough. During the diagnostic workup, which included contrast-enhanced computed tomography (CECT) of the chest, an incidental cystic lesion in the upper abdomen was revealed, a finding that prompted further imaging studies and referral to our tertiary centre. An abdominal CECT revealed a cystic lesion measuring 22 mm in maximum diameter located between the liver and the lesser curvature of the stomach (Figure 1).
Hepatic angiosarcoma (HA) mimicking a complex liver cystAxial and coronal imaging of CECT showing a large cystic lesion arising from the left lateral segment of the liver expanding between the liver, pancreas, and stomach (blue arrow). Some soft tissue components are evident (yellow arrow); however, in the context of the bi-lobar cystic lesion, this was interpreted initially as cyst wall complexity. HA: Hepatic angiosarcoma: CECT: Contrast-enhanced computed tomography
The case was brought for discussion in the multidisciplinary meeting, as radiological appearances were atypical; thus, diagnosis and management required discussion amongst specialists and consensus. Radiologically, the cyst appeared multilocular with a few internal septations. The differential diagnosis included complicated liver cyst, cystic differentiation of haemangioma, and biliary cystadenoma. Given the atypical features, a consensus was made to proceed to surgical resection in the form of peri-cystectomy for full histopathological evaluation and establishment of a definitive diagnosis. The patient was scheduled for surgery four weeks later. On the preoperative repeat CECT scan, findings were surprising. The cystic lesion appeared doubled in size and had clear features of malignant pathology (Figure 2).
HA mimicking complex liver cystAxial and coronal imaging of CECT showing the cystic lesion increased in size. On the right, a new solid tissue component infiltrating the liver (blue arrow) is evident along with a further increase in the inter-cystic soft tissue part of the lesion (yellow arrow). On the left, the inter-cystic soft tissue component is enhanced on arterial phase imaging (yellow arrow).HA: hepatic angiosarcoma; CECT: contrast enhanced computed tomography
On laparotomy, the CECT findings were confirmed, and multiple sites of peritoneal disease were identified. Core biopsies from the partly solid part of the lesion infiltrating the liver were taken for diagnosis confirmation. The histopathological examination revealed a pleomorphic malignant neoplasm consistent with HA. The patient was referred to the special Sarcoma Oncology centre for further treatment, but succumbed to the disease within four months.
Case 2
A 79-year-old female with a history of right-sided breast cancer treated with surgical excision presented with right-sided flank pain. A CECT scan of the thorax, abdomen, and pelvis was performed, which revealed a large lesion in segments V/VI of the liver (Figure 3). The lesion measured 8 cm in maximum diameter and appeared to have internal as well as peripheral nodular discontinuous enhancement with progressive centripetal fill-in. The overall radiological impression was that the lesion represents a somewhat atypical cavernous haemangioma.
HA mimicking cavernous haemangiomaAxial and coronal imaging of CECT showing the lesion with appearances in keeping with cavernous haemangioma (yellow arrow). Interpretation of the lesion as being a cavernous haemangioma was misleading, as the lesion was representing an HA.HA: hepatic angiosarcoma; CECT: contrast-enhanced computed tomography
Given the atypical radiological findings, a magnetic resonance imaging (MRI) of the liver was deemed necessary to further characterise the lesion. On MRI, the lesion appears hyperintense on delayed images. T2-weighted MRI shows marked hyperintensity, features in keeping with cavernous haemangioma (Figure 4). Despite the patient having had surgery for breast cancer in the past, previous imaging studies were not available to review and confirm the presence of this benign entity within the liver, and the final conclusion was that no further workup or follow-up was required.
HA mimicking cavernous haemangiomaMRI on T1 (left) and T2 (right) sequences. The lesion (yellow arrow) appears hypointense in T1 and hyperintense in T2, interpreted as cavernous haemangioma. MRI: magnetic resonance imaging; HA: hepatic angiosarcoma
One month later, the patient re-presented with intra-abdominal bleeding. CECT revealed rupture of the previously labelled cavernous haemangioma, and treatment involved right hepatic artery embolisation (Figure 5). Furthermore, multiple new liver lesions were identified with guided biopsy, confirming HA. The patient was referred to Sarcoma Oncology services; however, the aggressiveness of the disease did not allow for any additional treatment, and the patient died one month later.
HA mimicking cavernous haemangiomaOn top, CECT demonstrates spontaneous HA bleeding with perihepatic free fluid evident (blue arrows). On the bottom, MRI imaging shows HA progression in size but also new lesions demonstrating disease spread. MRI: magnetic resonance imaging; HA: hepatic angiosarcoma; CECT: contrast-enhanced computed tomography
Discussion
HA is an aggressive malignancy. Most cases present with advanced disease involving both liver lobes, and distant metastases in lungs and bones may be present [2,12]. Prognosis is poor, with most patients dying within six months of diagnosis [2,12]. Surgical resection and adjuvant systemic treatment have better survival, reaching a five-year survival of 79% in some series [3,12].
Early diagnosis on imaging studies plays a pivotal role, as it provides potential for treatment. In contrast-enhanced CECT, HA typically presents with peripheral enhancement in the late arterial phase and may exhibit a reversed enhancement pattern compared to that of benign cavernous haemangioma [13,14]. While haemangiomas often show early central enhancement followed by delayed peripheral fill-in, the absence of washout usually argues against malignancy. However, imaging features of HA are often inconsistent and may be misinterpreted [13,14].
In the first case described here, retrospective imaging review identified heterogeneous arterial enhancement at the periphery of the cystic lesion, an alarming radiological feature suggestive of aggressive malignant pathology. Nonetheless, these findings were initially overlooked, as the lesion was discovered incidentally during a work-up for persistent cough, and the patient lacked specific hepatic symptoms.
On non-contrast MRI, HA appears hypointense on T1-weighted images and characteristically shows heterogeneous hyperintensity on T2-weighted images [13,15]. This feature can help distinguish HA from benign haemangiomas; hence, careful evaluation and heightened radiological awareness during interpretation are essential [13,15]. In the second case described here, this specific feature was retrospectively identified as the key radiological sign raising suspicion for malignancy. On contrast-enhanced MRI, HA demonstrates imaging characteristics similar to those seen on CECT, including a heterogeneous enhancement pattern in both the arterial and venous phases [12,14,15]. These appearances can resemble those of other vascular liver tumours, and HA may easily mimic a benign haemangioma [15].
As radiological studies fail to contribute to early diagnosis, the rapid progression of disease on repeat imaging studies led to late diagnosis in both cases [12,14]. Similar cases have been reported in the literature, where hepatic angiosarcoma initially mimicked benign lesions such as haemangiomas, cystadenomas, or simple cysts, resulting in diagnostic delay [16,17]. The radiologic overlap between HA and cavernous haemangiomas has also been well reported [15,18]. Bartolotta et al. emphasized the diagnostic pitfalls in distinguishing vascular liver tumours with atypical enhancement patterns, further supporting the need for close imaging follow-up in ambiguous cases [18].
Radiological differentiation between HA and benign hepatic lesions is summarised in Table 1.
Histological studies may prove useful in the future in identifying HA subtypes potentially curable with liver transplantation, a treatment that is currently not indicated for this aggressive primary liver malignancy [3,9,12].
These cases highlight the importance of maintaining a high index of suspicion when encountering hepatic lesions with atypical or ambiguous imaging features. In clinical practice, reliance on a single imaging modality or a one-time scan can delay diagnosis, particularly when initial appearances suggest a benign lesion and it is encountered in patients in their sixth decade of life. Prompt follow-up imaging, especially in the presence of radiological red flags such as heterogeneous enhancement, atypical growth patterns, or interval changes, should be considered even in asymptomatic patients [15,19]. Furthermore, early percutaneous biopsy, although sometimes challenging in vascular tumours, may provide critical diagnostic clarity and should not be deferred in cases with progressive or unexplained imaging findings [20,21]. Adoption of this approach could potentially expedite diagnosis, avoid misclassification, and open a therapeutic window in a malignancy otherwise associated with dismal outcomes [2,22].
Conclusions
HA is a rare but very aggressive primary liver malignancy. Absence of symptoms shifts the diagnostic burden to imaging studies, with the latter failing to alarm clinicians as the tumour can mimic benign liver pathologies. Clinicians and radiologists should be alert to this pathology in patients in the sixth decade of life when interpreting vague symptoms, if any, and imaging studies with somewhat atypical features. Early diagnosis and surgical resection provide the only chance for prolonged survival.
These cases underscore the importance of prompt follow-up imaging and consideration of early biopsy when radiological features are equivocal or deviate from typical benign patterns. Incorporating such strategies into clinical practice may aid in earlier recognition of this aggressive malignancy, potentially improving outcomes in an otherwise dismal disease. Further histological and molecular analysis of HA subtypes may, in the future, define new therapeutic approaches and identify a subset of patients who may benefit from liver transplantation, a modality currently not recommended in this setting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Angiosarcoma of the liver: clinicopathologic features and morphologic patterns Am J Surg Pathol Yasir S Torbenson MS 5815904320193098679910.1097/PAS.0000000000001228 · doi ↗ · pubmed ↗
- 2Vascular tumors of the liver: a brief review Ann Hepatobiliary Pancreat Surg Sarangi S Thirunavukkarasu B Khera S 3293412720233795370910.14701/ahbps.23-046PMC 10700950 · doi ↗ · pubmed ↗
- 3Management strategies and outcomes in primary liver angiosarcoma Am J Clin Oncol Ramakrishnan N Mokhtari R Charville GW 4394444620233758087110.1097/COC.0000000000001032 PMC 10510833 · doi ↗ · pubmed ↗
- 4Angiosarcoma of the liver as a cause of fulminant liver failure BMJ Case Rep Montell García M Romero Cabello R Romero Feregrino R 2012201210.1136/bcr-2012-006417 PMC 454370322865805 · doi ↗ · pubmed ↗
- 5Thorotrast-induced ruptured hepatic angiosarcoma Abdom Imaging Azodo MV Gutierrez OH Greer T 7881181993843169810.1007/BF 00201708 · doi ↗ · pubmed ↗
- 6Pathomorphologic characteristics of 102 cases of thorotrast-related hepatocellular carcinoma, cholangiocarcinoma, and hepatic angiosarcoma Cancer Ito Y Kojiro M Nakashima T 61153621988 https://pubmed.ncbi.nlm.nih.gov/2457426/245742610.1002/1097-0142(19880915)62:6<1153::aid-cncr 2820620619>3.0.co;2-i · doi ↗ · pubmed ↗
- 7Angiosarcoma of the liver following vinyl chloride exposure JAMA Block JB 53542291974 https://pubmed.ncbi.nlm.nih.gov/4406736/4406736 · pubmed ↗
- 8Mutation analysis of K-ras-2 in liver angiosarcoma and adjacent nonneoplastic liver tissue from patients occupationally exposed to vinyl chloride Environ Mol Mutagen Weihrauch M Bader M Lehnert G 3640402002 https://onlinelibrary.wiley.com/doi/abs/10.1002/em.100841221107410.1002/em.10084 · doi ↗ · pubmed ↗