Staphylococcal Toxic Shock Syndrome Associated With a Cosmetic Rhinoplasty Procedure
Nanako Kitagawa, Daichi Umemoto, Hiroaki Nishioka

TL;DR
A 25-year-old woman developed life-threatening staphylococcal toxic shock syndrome after a cosmetic rhinoplasty and recovered with prompt treatment.
Contribution
Highlights staphylococcal TSS as a rare but serious complication of cosmetic rhinoplasty.
Findings
The patient developed TSS symptoms two days after rhinoplasty, including fever, vomiting, and rash.
Methicillin-susceptible Staphylococcus aureus was identified from nasal swabs.
Prompt treatment with fluids, vasopressors, and antibiotics led to recovery.
Abstract
Staphylococcal toxic shock syndrome (TSS) is a rare but life-threatening condition. Here, we present a case of a 25-year-old woman who developed staphylococcal TSS following cosmetic rhinoplasty. Two days before her hospital admission, she had undergone cosmetic rhinoplasty and experienced fever, vomiting, and skin rash following the procedure. On admission, she presented with hypotension. TSS was suspected, and treatment comprising fluid resuscitation, vasopressors, and antibiotics was promptly initiated. On examination, methicillin-susceptible Staphylococcus aureus was identified in nasal swab specimens. She recovered within a few days, and desquamation was observed later. Although rare, TSS should be recognized as a serious complication of cosmetic surgeries, particularly given the significant increase in the number of such procedures worldwide.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
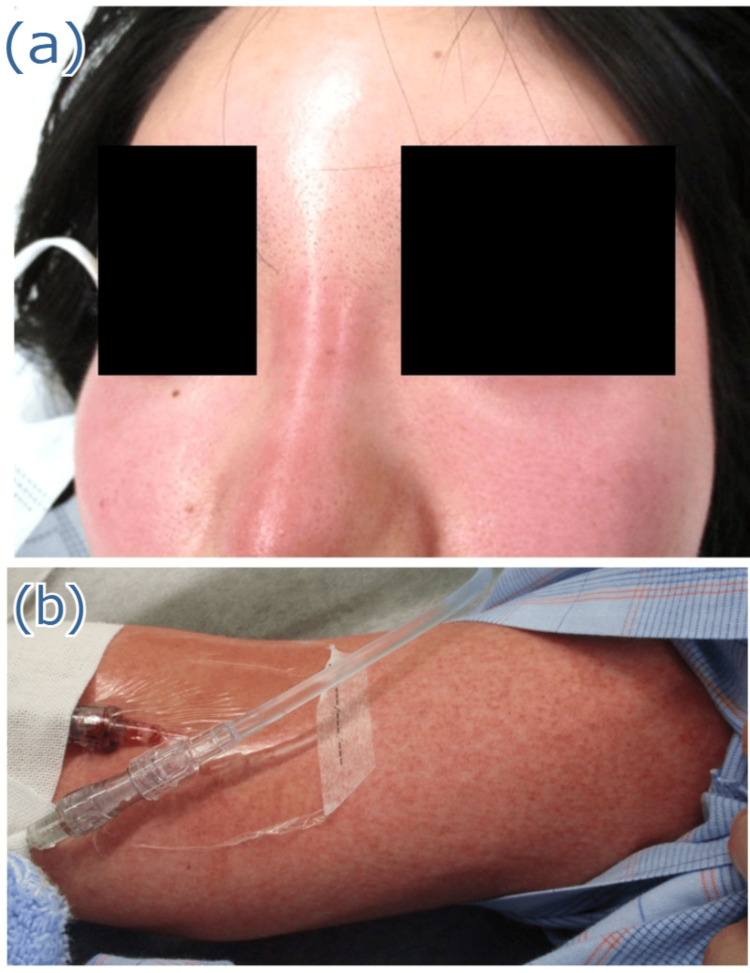 Figure 1
Figure 1 Figure 2
Figure 2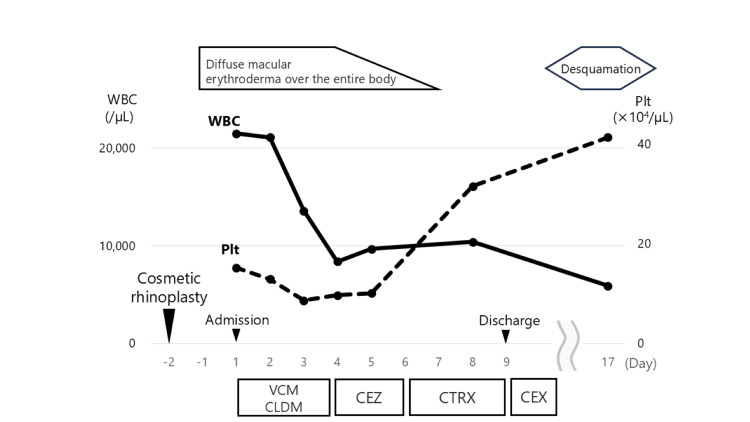 Figure 3
Figure 3| Blood work | Result | Reference range |
| White blood cell (/μL) | 13,600 | 3,900-9,800 |
| Neutrophils (%) | 92 | 26-71 |
| Lymphocyte (%) | 3.5 | 19-61 |
| Hemoglobin (g/dL) | 9.8 | 11.1-15.1 |
| Platelet (×104/μL) | 8.6 | 13.0-37.0 |
| Albumin (g/dL) | 3.2 | 3.9-4.9 |
| AST (U/L) | 38 | 8-40 |
| ALT (U/L) | 28 | 8-40 |
| BUN (mg/dL) | 36.8 | 8.0-20.0 |
| Cre (mg/dL) | 1.48 | 0.40-1.80 |
| CRP (mg/dL) | 28.59 | 0.00-0.50 |
| PCG | ABPC | CEZ | CFX | CTRX | GM | CLDM | LVFX | VCM | ST | LZD | DPC | |
| MSSA | 9 | 9 | 100 | 100 | 100 | 80 | 79 | 83 | 100 | 100 | 100 | 100 |
| Author, year | Age | Sex | Surgical procedure | Detection sites of | Outcome |
| Jacobson & Kasworm, 1986 [ | 27 | F | Septoplasty | Maxillary sinus | Recovered |
| 34 | M | Septoplasty | (-) | Recovered | |
| 29 | F | Septoplasty | Right and left nostril | Recovered | |
| Tobin et al., 1987 [ | 29 | F | Herniorrhaphy and septorhinoplasty | Nasal cultures | Recovered |
| Wilson et al., 1987 [ | 39 | F | Antroscopy and turbinectomy | Nasal swab | Recovered |
| Nahass & Gocke, 1988 [ | 32 | M | Nasal polypectomy, septoplasty | Nares and sinus drainage | Recovered |
| Jones & MacRae, 1990 [ | 50 | M | Septoplasty | Nasal cavities | Recovered |
| Liu et al., 1990 [ | 32 | M | Submucous resection of the nasal septum and polypectomy | Throat swab | Recovered |
| Abifadel et al., 1990 [ | 24 | M | Cosmetic rhinoplasty | (+) | Recovered |
| Schweitzer et al., 1990 [ | 30 | M | Septorhinoplasty | Blood culture | Recovered |
| Abram et al., 1994 [ | 30 | M | Functional endonasal sinus surgery, septoplasty | Nasal culture | Recovered |
| 32 | F | Functional endonasal sinus surgery | Nasal culture | Recovered | |
| 14 | F | Second-stage endonasal clean-out procedure after functional endonasal sinus surgery | Nasal and throat cultures | Recovered | |
| 25 | F | Functional endonasal sinus surgery | Throat cultures | Recovered | |
| 8 | M | Second-stage endonasal clean-out procedure after functional endonasal sinus surgery | Nasal cultures | Recovered | |
| Miller & Stankiewicz, 1994 [ | 61 | F | Endoscopic bilateral total ethmoidectomy, sphenoidotomy, maxillary antrostomy, and septoplasty | Sinus cultures | Recovered |
| Graham et al., 1995 [ | 29 | M | Nasal septoplasty | Wound cultures | Recovered |
| Younis & Lazar, 1996 [ | 5 | M | Functional endonasal sinus surgery | Direct sinus cultures | Recovered |
| 7 | F | Functional endonasal sinus surgery | Sinus cultures | Recovered | |
| 32 | M | Functional endonasal sinus surgery | Blood and sinus cultures | Recovered | |
| Our case | 25 | F | Cosmetic rhinoplasty | Nasal swab | Recovered |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNasal Surgery and Airway Studies · Historical Medical Research and Treatments · Mycobacterium research and diagnosis
Introduction
Toxic shock syndrome (TSS) is a rare but life-threatening complication that can arise from certain bacterial infections. It is primarily caused by toxins produced by Staphylococcus aureus, particularly toxic shock syndrome toxin-1 (TSST-1); however, the condition may also be provoked by toxins produced by group A streptococci [1]. TSS typically presents with a sudden onset of fever, rash, hypotension, and involvement of multiple organs. Dermatological symptoms include diffuse macular erythroderma, followed by skin peeling (desquamation) one to two weeks later. Importantly, TSS can affect anyone, even individuals who are otherwise healthy.
Staphylococcal TSS is generally categorized into two types: menstrual and non-menstrual. Menstrual TSS is often linked to tampon use, although there have been reports of its association with menstrual cups and intrauterine devices [1,2]. Non-menstrual TSS may occur in various clinical situations, including surgical and postpartum wound infections, septorhinoplasty, osteomyelitis, purpura fulminans, and post-influenza complications [2,3]. However, reports on staphylococcal TSS after cosmetic rhinoplasty are rare.
In this report, we present the case of a young woman who developed staphylococcal TSS, which was associated with cosmetic rhinoplasty.
Case presentation
A previously healthy 25-year-old woman was admitted to our hospital with a one-day history of fever, vomiting, and generalized skin rash. Two days before admission, she had undergone cosmetic rhinoplasty at another cosmetic surgery clinic. The patient did not take any medication and reported no history of smoking, alcohol consumption, or food or drug allergies. Also, she did not report using menstrual tampons. Physical examination revealed a blood pressure of 69/44 mmHg, pulse rate of 158/min, respiratory rate of 25 breaths/min, and body temperature of 39.3 ℃. The patient was alert and conscious. Notable findings included redness of the nasal root, bilateral conjunctival hyperemia, and diffuse macular erythroderma over the entire body (Figure 1). The heart and breathing sounds were clear, and there were no insect bites. Laboratory findings showed the following results: white blood cell (WBC) count, 13,600/μL (with neutrophils: 92.0%); hemoglobin, 9.8 g/dL; platelet count, 8.6×10^4^/μL; albumin, 3.2 g/dL; aspartate aminotransferase, 38 U/L; alanine aminotransferase, 28 U/L; blood urea nitrogen, 36.8 mg/dL; creatinine, 1.48 mg/dL; C-reactive protein, 28.59 mg/dL (Table 1). Anti-measles IgM antibody test results were negative, and blood and urine cultures did not show bacterial growth. Computed tomography of the face revealed a rhinoplasty artifact on the nasal dorsum, without surrounding fluid accumulation (Figure 2).
Physical examination findingsRedness of the nasal root (a) and diffuse macular erythroderma over the arm (b) are observed.
A computed tomography scan of the faceA rhinoplasty artifact on the nasal dorsum (white arrows), without surrounding fluid accumulation, is revealed.
TSS was suspected based on clinical findings, including high fever, diffuse rash, hypotension, thrombocytopenia, and vomiting. The patient underwent immediate fluid resuscitation using norepinephrine and vasopressin. Treatment with vancomycin (targeting trough levels of 15-20 µg/mL) and clindamycin (600 mg every 8 h) was initiated. Polymerase chain reaction analysis (FilmArray®; bioMérieux, Tokyo) of nasal swab specimens obtained from the rhinoplasty surgical site tested positive for S. aureus, which was identified as methicillin-susceptible S. aureus. By day 3, the patient recovered from shock, and the antibiotic regimen was changed to cefazolin (2 g every 8 h) (Table 2). On day 4, the fever resolved, and by day 6, the rash gradually improved. Owing to the increase in eosinophils (WBC count of 9,700/μL with 16.5% eosinophils), likely caused by an allergy to cefazolin, the antibiotic was switched to ceftriaxone (2 g every 24 h). The patient was discharged on day 9. She started taking cefalexin (2 g/day) but discontinued it at her own discretion owing to the appearance of a skin rash. After discontinuation of the medication, the skin rash quickly disappeared, and the patient remained symptom-free and healthy. On day 17, the patient returned to our outpatient department for a follow-up visit, where desquamation of her upper arms was observed; however, there was no redness at the nasal root (Figure 3). Ultimately, the patient was diagnosed with staphylococcal TSS, which is likely related to cosmetic rhinoplasty.
Patient’s clinical courseCEX: cefalexin, CLDM: clindamycin, CTRX: ceftriaxone, Plt: platelet, VCM: vancomycin, WBC: white blood cell
Discussion
The clinical course of our patient highlighted two important observations: first, TSS may develop after rhinoplasty for cosmetic reasons, and second, TSS can be treated effectively without the need to remove foreign bodies.
TSS is a life-threatening condition that can develop rapidly; therefore, prompt identification of its cause is essential. While tampon use during menstruation is a well-known trigger for TSS, research shows that at least half of the reported cases of staphylococcal TSS are unrelated to menstruation [4], and the mortality rate of non-menstrual TSS can be as high as 4%-22%, which is greater than that of menstrual TSS [1]. Surgery on the nasal area can lead to staphylococcal TSS, and some cases of staphylococcal TSS related to nasal surgery have been reported in the literature (Table 3) [5-16]. However, only one case, documented in French, was associated with cosmetic purposes [11], as seen in our case. Although cosmetic surgery may be less likely to result in staphylococcal TSS, TSS should be recognized as a serious complication of cosmetic rhinoplasty, especially considering the significant increase in cosmetic plastic surgeries globally in recent years, with rhinoplasty procedures alone increasing by 21.6% annually [17].
The exotoxin TSST-1, produced by* S. aureus*, is believed to play a significant role in the pathogenesis of staphylococcal TSS. However, the mechanisms underlying postoperative staphylococcal TSS are poorly understood. In this case, the patient had a silicone implant inserted for prosthetic rhinoplasty in the nasal dorsum, where *S. aureus *colonization was likely to occur. Surgical procedures create an oxygen-rich environment in the nasal dorsum that promotes *S. aureus *growth and TSST-1 production. This toxin disrupts the mucosal barrier and stimulates cytokine production, leading to the development of TSS [2]. TSST-1 may also promote S. aureus colonization within the nasal dorsum by activating CD8+ T cells [18]. Additionally, surgical procedures compromise the immunological barrier, thereby possibly allowing foreign materials to become substrates for bacterial growth.
The management of TSS includes supportive care, surgical debridement (if warranted), removal of infected foreign bodies, and antibiotic administration. Fluid resuscitation and vasopressor administration should begin immediately, along with intubation, ventilation, and renal replacement therapy, as required [1]. For source control, removal of abscesses, packing, or foreign bodies is recommended. However, a few cases of TSS have been successfully treated without the need to remove foreign bodies [19,20], indicating that TSS can sometimes be managed effectively without surgical intervention. In this case, because the patient did not want to undergo surgery, and her nasal inflammation seemed mild, we attempted to treat her without removing the implant. However, we were uncertain whether the implant was genuinely infected in our case. In terms of antibiotic therapy, a combination of vancomycin and clindamycin may be considered as an initial treatment option, targeting Gram-positive cocci, including *S. aureus *or streptococcal species, which are common causative organisms of TSS. Although no studies have provided guidelines on the duration of antibiotic therapy for TSS [1], antibiotics are typically administered for 14 days.
Conclusions
This case demonstrates that staphylococcal TSS can occur following rhinoplasty performed for cosmetic purposes. Although TSS is a rare complication of cosmetic rhinoplasty, it is important to recognize the increasing prevalence of plastic surgery worldwide. Early diagnosis and prompt treatment are crucial because TSS is a life-threatening condition. When patients present with a sudden onset of fever, rash, and hypotension, clinicians should consider TSS as a possible diagnosis and inquire about any recent history of cosmetic surgery, despite its rarity as a complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Toxic shock syndrome: a literature review Antibiotics (Basel) Atchade E De Tymowski C Grall N Tanaka S Montravers P 961320243824765510.3390/antibiotics 13010096 PMC 10812596 · doi ↗ · pubmed ↗
- 2Device-associated menstrual toxic shock syndrome Clin Microbiol Rev Schlievert PM Davis CC 33202010.1128/CMR.00032-19PMC 725486032461307 · doi ↗ · pubmed ↗
- 3Toxic shock syndrome after surgery: case presentation and systematic review of the literature Plast Reconstr Surg Glob Open Celie KB Colen DL Kovach SJIII 08202010.1097/GOX.0000000000002499 PMC 757207533133879 · doi ↗ · pubmed ↗
- 4Clinical and molecular epidemiology of staphylococcal toxic shock syndrome in the United Kingdom Emerg Infect Dis Sharma H Smith D Turner CE 2582662420182935015910.3201/eid 2402.170606 PMC 5782905 · doi ↗ · pubmed ↗
- 5Toxic shock syndrome after nasal surgery. Case reports and analysis of risk factors Arch Otolaryngol Head Neck Surg Jacobson JA Kasworm EM 3293321121986394264110.1001/archotol.1986.03780030093019 · doi ↗ · pubmed ↗
- 6Toxic shock syndrome following breast and nasal surgery Plast Reconstr Surg Tobin G Shaw RC Goodpasture HC 111114801987360214910.1097/00006534-198707000-00019 · doi ↗ · pubmed ↗
- 7Toxic shock syndrome after nasal surgery Rhinology Wilson JA von Haacke NP Mc Andrew PT Murray JA 139140251987 https://pubmed.ncbi.nlm.nih.gov/3616393/3616393 · pubmed ↗
- 8Toxic shock syndrome associated with use of a nasal tampon Am J Med Nahass RG Gocke DJ 629631841988334827210.1016/0002-9343(88)90147-7 · doi ↗ · pubmed ↗