Optimizing Laparoscopic Adrenal Surgery: A Retrospective Study of 83 Patients at a Tertiary Cancer Center
Mohamed I Fahim, Fady Shafeik, El Sayed Ashraf Khalil, Abdelmaksoud M Ali, Rasha M Allam, Marina Asaad

TL;DR
This study compares laparoscopic and open adrenal surgery outcomes, finding laparoscopic surgery feasible for small benign adrenal tumors with some technical adjustments.
Contribution
The study introduces technical modifications like modified port positioning and gauze retractors to improve laparoscopic adrenal surgery.
Findings
Laparoscopic adrenalectomy was feasible for lesions up to 6 cm with technical modifications.
There was a significant difference in lesion size between open and laparoscopic approaches.
One postoperative death occurred in the laparoscopic group, while no mortality was recorded in the open group.
Abstract
Aim of the study This study aims to report our institutional outcomes of laparoscopic adrenalectomy, to compare these with a cohort of patients undergoing open adrenalectomy, and to describe the feasibility and utility of technical modifications, including modified port positioning and the use of intra-abdominal gauze retractors. Patients and methods This retrospective cohort study included 83 patients with radiologically benign-appearing adrenal tumors who underwent adrenalectomy at the National Cancer Institute (NCI), Cairo University, Cairo, Egypt, between January 2014 and January 2020. Patient data were extracted from medical records and included demographics (age and gender), lesion characteristics (size, laterality, and functional status), surgical approach (laparoscopic or open), and results of endocrine investigations (serum metanephrines, urinary vanillylmandelic acid (VMA),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
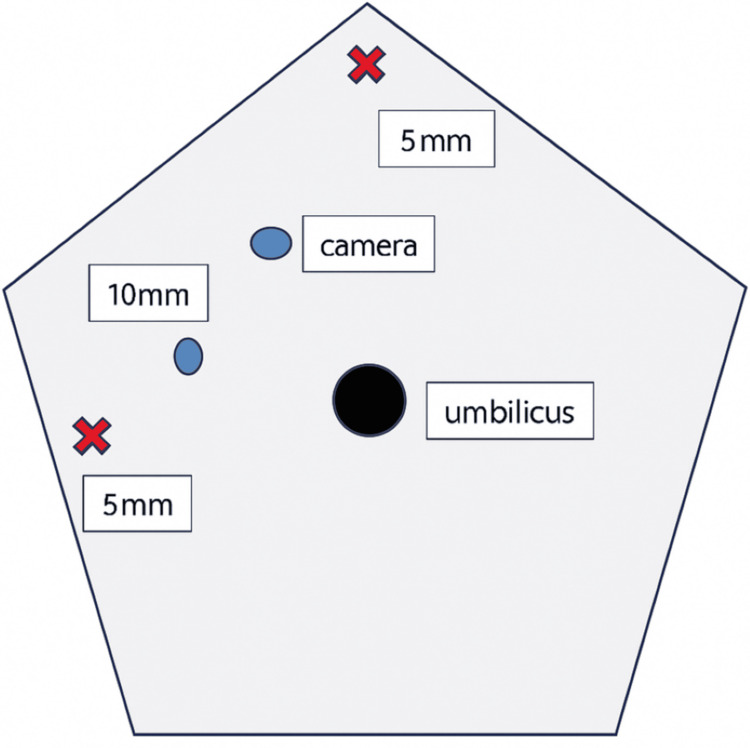 Figure 1
Figure 1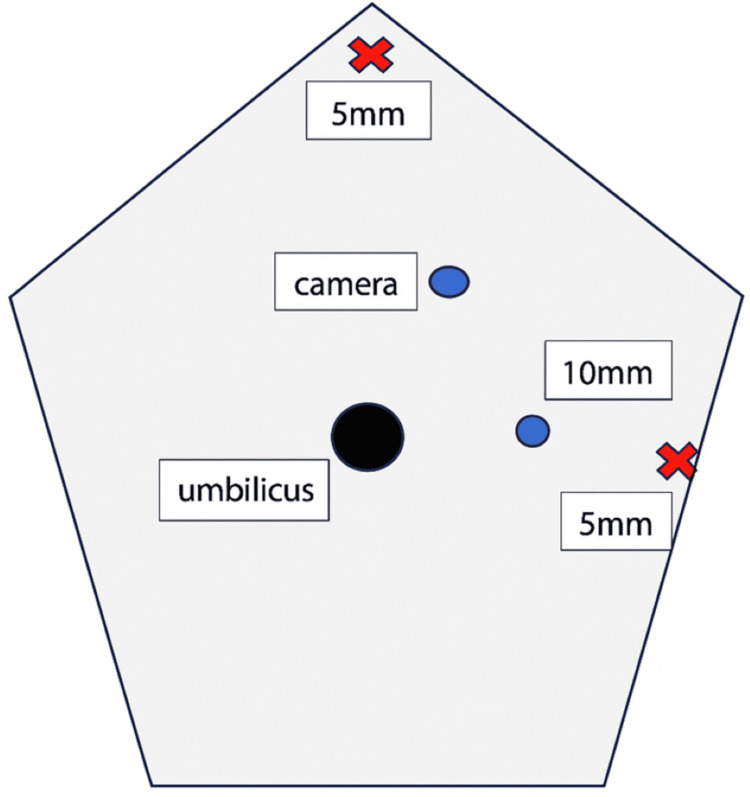 Figure 2
Figure 2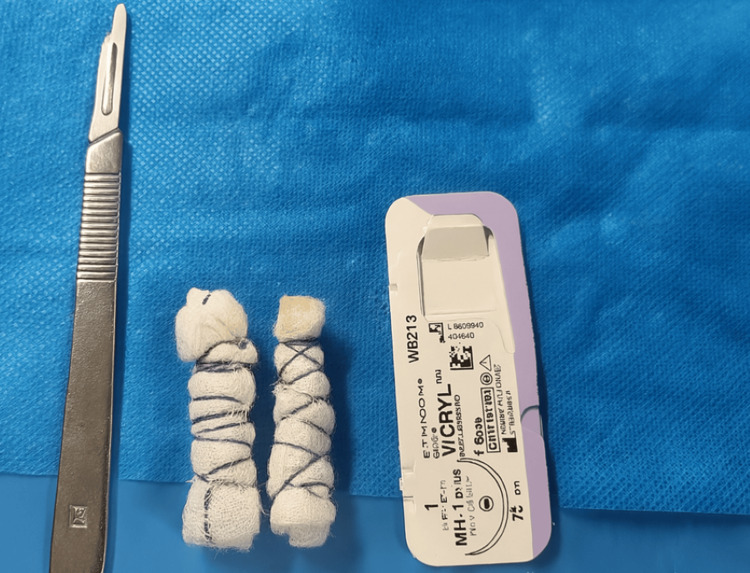 Figure 3
Figure 3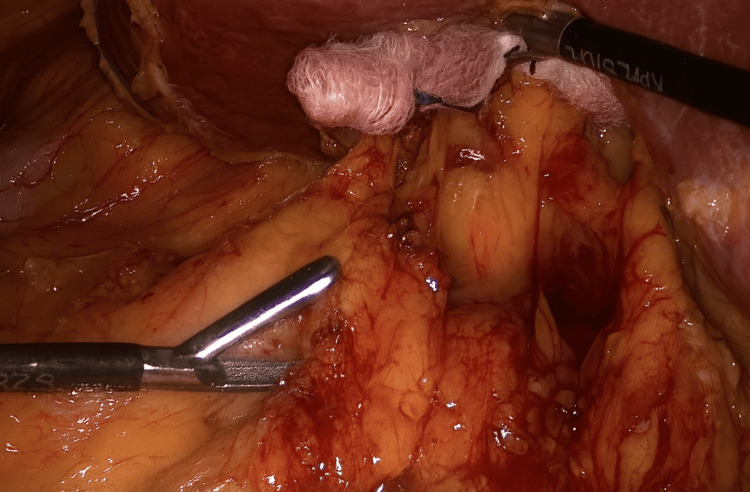 Figure 4
Figure 4 Figure 5
Figure 5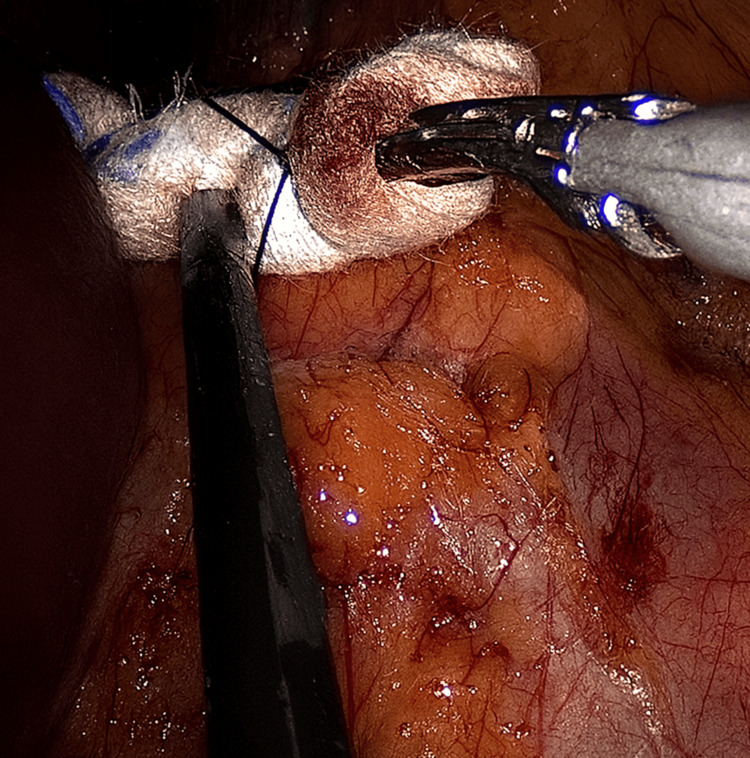 Figure 6
Figure 6 Figure 7
Figure 7| Variables | Open (n=51) | Laparoscopic (n=32) | Test used and value | P value | |
| Age (years) | <47 | 22 (43.1%) | 18 (56.3%) | Chi-square = 1.354 | 0.245 |
| >=47 | 29 (56.9%) | 14 (43.8%) | |||
| Gender | Male | 21 (41.2%) | 8 (25.0%) | Chi-square = 2.263 | 0.132 |
| Female | 30 (58.8%) | 24 (75.0%) | |||
| Laterality | Right | 32 (62.7%) | 25 (78.1%) | Chi-square = 2.162 | 0.141 |
| Left | 19 (37.3%) | 7 (21.9%) | |||
| Size of lesion by radiology (cm) | <=6.5 | 22 (43.1%) | 20 (62.5%) | Chi-square = 2.949 | 0.086 |
| >6.5 | 29 (56.9%) | 12 (37.5%) | |||
| Size of lesion by pathology (cm) | <=6 | 21 (41.2%) | 22 (68.8%) | Chi-square = 5.988 | 0.014* |
| >6 | 30 (58.8%) | 10 (31.3%) | |||
| Size of gland by pathology (cm) | <=5.5 | 23 (45.1%) | 19 (59.4%) | Chi-square = 1.603 | 0.205 |
| >5.5 | 28 (54.9%) | 13 (40.6%) | |||
| Function | Functioning | 19 (37.3%) | 13 (40.6%) | Chi-square = 0.094 | 0.759 |
| Non-functioning | 32 (62.7%) | 19 (59.4%) | |||
| Pathological diagnosis | Benign | 29 (56.9%) | 17 (53.1%) | Fischer’s exact = 0.335 | 0.919 |
| Malignant | 2 (3.9%) | 1 (3.1%) | |||
| Unpredictable behavior | 20 (39.2%) | 14 (43.8%) | |||
| Pathological diagnosis | Benign | 29 (56.9%) | 17 (53.1%) | Chi-square = 0.111 | 0.739 |
| Malignant & unpredictable behavior | 22 (43.1%) | 15 (46.9%) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Hormonal Regulation and Hypertension · Pituitary Gland Disorders and Treatments
Introduction
Laparoscopic adrenalectomy has become the standard surgical approach for managing benign adrenal tumors, following its first description by Gagner et al. in 1992 [1]. Compared to traditional open adrenalectomy, the laparoscopic technique offers several notable advantages, including reduced postoperative pain, quicker recovery, shorter hospital stay, and improved cosmetic outcomes [1,2].
The anatomical location of the adrenal glands - deep within the retroperitoneal space - makes surgical access inherently challenging. Achieving sufficient exposure via open surgery often necessitates a large incision disproportionate to the gland's size. In contrast, a laparoscopic approach enables precise access with minimal disruption, making it a favorable option when oncological safety can be maintained [2,3].
This study presents our institutional experience with laparoscopic adrenalectomy, reporting institutional outcomes of laparoscopic adrenalectomy, comparing them with a cohort of open adrenalectomy cases, and describing the feasibility and utility of technical modifications, including modified port positioning and the use of intra-abdominal gauze retractors.
It also explores how tumor size influenced the choice of surgical approach and outcomes. Both elements are examined in the context of a real-world, evolving laparoscopic practice at a tertiary oncology center.
Materials and methods
We conducted a retrospective observational cohort study at the National Cancer Institute (NCI), Cairo University, Cairo, Egypt. A total of 83 patients underwent adrenalectomy for radiologically benign‑appearing adrenal lesions between January 2014 and January 2020. Patient data were retrieved from hospital records and entered into a standardized database for subsequent analysis.
Patients were considered eligible if imaging demonstrated a benign‑appearing adrenal lesion, if they had a good performance status, and if baseline liver and kidney functions were preserved. Patients were excluded when pre‑operative imaging suggested malignant features such as irregular borders, infiltration of adjacent structures, or suspicious lymphadenopathy. Patients who were deemed unfit for surgery were also excluded.
Among the 83 patients, 51 (61.4%) underwent open adrenalectomy, and 32 (38.6%) underwent laparoscopic adrenalectomy. All laparoscopic procedures were performed with the patient in a semi‑lateral position. Four ports were used: one 10‑mm camera port, one additional 10‑mm port, and two 5‑mm ports. For optimal retraction, a small piece of gauze was rolled and tied with 1‑0 Vicryl and introduced through the 10‑mm port to serve as an intra‑abdominal retractor. This method was adopted as a simple, flexible, and atraumatic alternative to rigid instruments, particularly useful in cases where deeper retroperitoneal access was required and advanced laparoscopic tools were not routinely available. It reflects the early phase of laparoscopic practice development within our unit. The port placements and retraction technique are illustrated in Figures 1-7.
Port placement for right-sided laparoscopic adrenalectomy
Port placement for left-sided laparoscopic adrenalectomy
Intra-abdominal gauze retractors prepared for use
Application of the gauze retractor during right-sided adrenalectomy
Alternative view showing the gauze retractor on the right side
Use of the gauze retractor during left-sided adrenalectomy
Additional view of the gauze retractor in the left-sided procedure
The decision regarding surgical approach was individualized and made by the operating surgeon based on multiple factors, including tumor size and characteristics, patient comorbidities, prior abdominal surgery, and the surgeon’s laparoscopic expertise. As this study took place during the early phase of laparoscopic adoption in our unit, surgeon preference and case complexity played key roles in determining the approach.
The procedures were performed by senior consultant surgeons, including professors and lecturers in surgical oncology, with more than 10-20 years of operative experience at our institution.
Data collected for each patient included demographic details (age and sex), lesion characteristics (side and size), endocrine profile (serum metanephrines, urinary vanillyl mandelic acid (VMA), aldosterone, cortisol, sodium, and potassium), the chosen surgical approach (laparoscopic or open), and histopathological results.
Tumor size was assessed preoperatively using cross-sectional imaging and confirmed by pathological examination. Although it was considered during surgical planning, there was no fixed size cutoff; decisions were influenced by surgeon experience and unit expertise.
Postoperative follow‑up began one month after discharge and was continued at six‑month intervals. Follow‑up included imaging-computed tomography (CT) of the abdomen and pelvis and hormonal evaluations when indicated, particularly in patients with functioning adrenal lesions. The median follow‑up duration for the cohort was 30 months.
All patients provided written informed consent prior to inclusion in the study. The study protocol was reviewed and approved by the local institutional ethics committee.
Data were analyzed using Statistical Product and Service Solutions (SPSS, version 22; IBM SPSS Statistics for Windows, Armonk, NY). Quantitative variables were summarized as mean and range, and categorical variables were expressed as frequencies and percentages. Comparisons between open and laparoscopic groups for categorical variables were performed using the chi‑square test or Fisher’s exact test where appropriate. Continuous variables were compared using Student’s t‑test. A p‑value of less than 0.05 was considered statistically significant.
Results
A total of 83 patients with adrenal tumors were included in this study and were followed throughout the designated period. The median age of the cohort was 47 years. Of these, 51 patients underwent open adrenalectomy, while 32 were managed laparoscopically. Detailed demographic and pathological characteristics are presented in Table 1. A statistically significant difference was observed in the pathological size of adrenal lesions between the open and laparoscopic groups (p = 0.014).
Histopathological analysis revealed that 47 patients had benign adrenal lesions, including adenomas, ganglioneuromas, myelolipomas, cysts, and hematomas. A further 34 patients were diagnosed with borderline tumors, primarily pheochromocytomas, and three patients were found to have adrenocortical carcinoma based on postoperative pathology.
With respect to lesion function, 51 patients (61.4%) presented with non-functioning adrenal tumors, while the remaining 32 patients (38.6%) had functioning lesions. Among these, 31 were confirmed to have hormonally active pheochromocytomas, and one patient had a cortisol-secreting tumor.
In the laparoscopic group, two cases - both involving right-sided adrenalectomy - were converted to open procedures due to intraoperative bleeding. One of these patients experienced a fatal postoperative complication, resulting in mortality on the first day after surgery. In contrast, no postoperative deaths occurred among patients who underwent open adrenalectomy. All patients in both groups remained disease-free during follow-up, with no clinical or radiological evidence of recurrence or metastasis.
Discussion
In this study, the majority of adrenal tumors were non-functioning, comprising 61.4% (51 of 83 cases), while the remaining 38.6% (32 patients) had functioning lesions. These findings are consistent with previously reported literature, which has shown that non-functioning adrenal tumors represent the most common clinical presentation [4,5].
Tumor size plays a critical role in determining the surgical approach. Several authors have advocated for a maximum lesion size of 6 cm for laparoscopic adrenalectomy, citing increased technical challenges and a higher probability of malignancy with larger tumors [6,7]. However, other studies have reported successful laparoscopic resection in select cases with lesions up to 8 cm in diameter, particularly when preoperative imaging and hormonal evaluation do not suggest malignancy [8,9].
The choice of surgical approach in this study was not based on a strict size threshold. Although a 6 cm cutoff is often used in the literature to guide laparoscopic feasibility, decisions were influenced by surgeon experience, tumor characteristics, and intraoperative conditions. During the study period, laparoscopic adrenalectomy was still being adopted in our unit, and as a tertiary oncology center, open surgery remained the default in many cases - including some with lesions under 6 cm.
In our cohort, one-third of patients with lesions larger than 6 cm (10 out of 30) were managed laparoscopically, while the rest underwent open surgery. The pathological lesion size was significantly different between groups (p = 0.014), supporting the cautious selection of laparoscopic cases based on tumor characteristics, size, and surgical expertise.
According to the European Society of Endocrinology Clinical Practice Guidelines, features such as tumor size exceeding 4 cm, irregular margins, heterogeneous appearance, and multiple hormone secretion raise suspicion for adrenocortical carcinoma and warrant consideration for open resection [10]. Similarly, the 2022 NCCN Guidelines for Neuroendocrine and Adrenal Tumors recommend open adrenalectomy in cases where imaging or biochemical profiles suggest malignancy.
Recent advancements in minimally invasive adrenal surgery are rapidly evolving. Robotic adrenalectomy has emerged as a promising alternative to conventional laparoscopy, offering enhanced dexterity, three-dimensional visualization, and improved ergonomics. Comparative studies and meta-analyses have demonstrated that robotic adrenalectomy may lead to shorter operative times, reduced blood loss, and similar oncological outcomes in appropriately selected cases [11]. In addition, technologies such as 3D laparoscopy, high-energy sealing devices, and intraoperative fluorescence imaging have been introduced to improve dissection accuracy and reduce complication rates [12]. The integration of Enhanced Recovery After Surgery (ERAS) protocols has further contributed to shorter hospital stays and optimized perioperative outcomes in adrenal surgery [13].
In addition, multi-institutional series have confirmed the safety and reproducibility of laparoscopic adrenalectomy across large patient cohorts, further validating its role as a standard approach for benign adrenal disease [14]. Moreover, recent prospective data highlight that optimized perioperative pathways, including individualized anesthesia protocols and minimally invasive techniques, continue to reduce morbidity and improve long-term functional outcomes after adrenal surgery [15].
In our experience, the use of gauze retractors appeared to improve operative exposure during laparoscopic dissection, particularly in cases requiring deep retroperitoneal access. Similarly, the modified port configuration was subjectively found to provide comfortable ergonomics for the surgical team. However, as no objective measures (e.g., operative time, blood loss, or standardized surgeon feedback) were used to quantify these aspects, these observations should be interpreted as subjective impressions rather than validated findings.
This study has several limitations. Its retrospective design introduces potential for selection bias and unmeasured confounding. The relatively small sample size, particularly when divided between laparoscopic and open groups, limits the statistical power of between-group comparisons. As a single-institution experience, the results may not be fully generalizable to other surgical teams or populations. Furthermore, the significant difference in pathological tumor size between the groups suggests that selection bias may have favored laparoscopic resection for smaller lesions. These factors should be considered when interpreting our findings, and further prospective multicenter studies are recommended.
While this study describes the feasibility of gauze retraction in laparoscopic adrenalectomy, it was not designed to compare outcomes between cases with and without this technique. Future prospective studies could further assess its relative benefits and clinical impact.
Conclusions
Laparoscopic adrenalectomy appears to be a feasible technique in selected patients with benign-appearing adrenal lesions, particularly for lesions up to 6 cm. Technical modifications, such as modified port positioning and the use of gauze retractors, were subjectively found to enhance operative exposure and facilitate dissection. However, due to the study's retrospective design, selection bias, and small sample size, no definitive conclusions regarding comparative safety or superiority over open surgery can be drawn. Further prospective studies are warranted to validate these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma N Engl J Med Gagner M Lacroix A BoltéE 10333271992138770010.1056/NEJM 199210013271417 · doi ↗ · pubmed ↗
- 2Laparoscopic adrenalectomy for large adrenocortical carcinoma JSLS Machado NO Al Qadhi H Al Wahaibi K Rizvi SG 019201510.4293/JSLS.2015.00036 PMC 448795726175553 · doi ↗ · pubmed ↗
- 3Laparoscopic adrenalectomy versus open adrenalectomy: results from a retrospective comparative study Ulster Med J Ramachandran MS Reid JA Dolan SJ Farling PA Russell CF 126128752006 https://pmc.ncbi.nlm.nih.gov/articles/PMC 1891736/16755942 PMC 1891736 · pubmed ↗
- 4Laparoscopic treatment of adrenal tumors: a single-center experience with 58 patients Surg Res Pract Ari A Buyukasik K Tatar C 9574391201620162797508110.1155/2016/9574391 PMC 5128712 · doi ↗ · pubmed ↗
- 5Laparoscopic versus open adrenalectomy: a retrospective comparative study Med Arch Al-Jalabneh T Al-Shawabkeh O Al-Gwairy I Abu-Zeitoun O Al-Njadat I Al-Soudi M Zarour A 41447520213401219810.5455/medarh.2021.75.41-44PMC 8116067 · doi ↗ · pubmed ↗
- 6Laparoscopic adrenalectomy compared to open adrenalectomy for benign adrenal neoplasms J Am Coll Surg Brunt LM Doherty GM Norton JA Soper NJ Quasebarth MA Moley JF 1101831996 https://pubmed.ncbi.nlm.nih.gov/8673301/8673301 · pubmed ↗
- 7Laparoscopic adrenalectomy: lessons learned from 100 consecutive procedures Ann Surg Gagner M Pomp A Heniford BT Pharand D Lacroix A 2382472261997933993010.1097/00000658-199709000-00003 PMC 1191015 · doi ↗ · pubmed ↗
- 8Adrenalectomy in the era of laparoscopy Surgery Staren ED Prinz RA 7067111201996886238110.1016/s 0039-6060(96)80020-1 · doi ↗ · pubmed ↗