Exploring the Zika virus epidemic’s association with fertility in a cohort of women of Northeastern Brazil: socioeconomic and educational gradients
Carlos Sanhueza-Sanzana, Carl Kendall, Kasim Allel, Moisés Humberto Sandoval González, Rosa Livia Freitas de Almeida, Italo Wesley Oliveira Aguiar, Lívia Karla Sales Dias, Roberto Justa da Pires, Cristiane Cunha Frota, Francisco Gustavo Silveira Correia

TL;DR
This study examines how the Zika virus outbreak in Brazil affected fertility rates, finding that socioeconomic factors like education and overcrowding influenced birth trends.
Contribution
The study reveals how the Zika epidemic impacted fertility rates and highlights sociodemographic disparities in reproductive behavior.
Findings
Fertility rates dropped during the Zika epidemic and increased afterward.
Low education and overcrowding were linked to higher fertility rates.
Unwanted pregnancies were associated with reduced fertility.
Abstract
To explore the association between the Zika virus epidemic, fertility rates, and sociodemographic and behavioral factors influencing birth trends. A prospective cohort of 1,497 women aged between 15 and 39 years living in arbovirus-endemic areas in Fortaleza, Brazil, was analyzed. Women were enrolled in February 2018 and followed up two times every six months. The total fertility rate (TFR), age-specific fertility rate (ASFR), and mean age at first birth (MAB) were estimated and a multivariate Poisson regression model was used to explore the main factors associated with fertility. The TFR was lowest during the epidemic period (2.64, 95%CI 2.06-3.06), increasing in the post-epidemic phase (TFR=3.52, 95%CI 3.18-3.86). Low educational attainment (RR=1.32, TFR=3.69, 95%CI 3.26-4.13), overcrowding (RR=1.27, TFR=3.26, 95%CI 2.98-3.54), and having undergone an abortion (RR=1.85, TFR=4.88,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
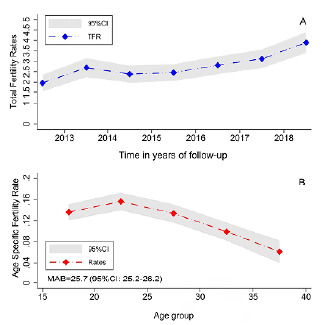 Figure 1
Figure 1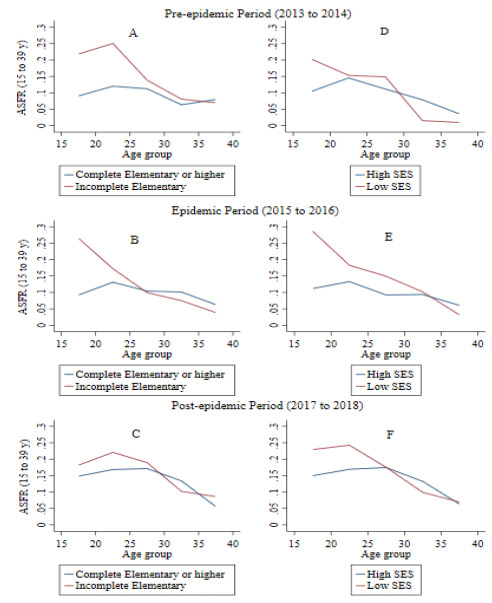 Figure 2
Figure 2- —National Council for Scientific and Technological Development
- —Coordination for the Improvement of Higher Education Personnel
- —Ceará Support Foundation for Scientific and Technological Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Demographic Trends and Gender Preferences · Adolescent Sexual and Reproductive Health
INTRODUCTION
In 2015, the Zika virus (ZIKV) outbreak in Brazil, initially detected in the state of Pernambuco, triggered a Public Health Emergency of National Importance (Emergência em Saúde Pública de Importância Nacional - ESPIN) declaration due to a surge in neonatal microcephaly cases1 ^,^ 2. The outbreak spread to 14 Brazilian states and 33 countries in the Americas3, resulting in 3,742 confirmed cases of congenital infections with abnormal child growth by March 5, 2024, with 1,828 (48.9%) attributed to Congenital Zika Syndrome (CZS), of which 1,380 (75.5%) occurred in the Northeast region4. ZIKV, alongside Dengue (DENV) and Chikungunya (CHIKV) viruses, circulated in urban areas, causing significant human morbidity and mortality5 ^,^ 6 ^,^ 7 ^,^ 8 ^,^ 9 ^,^ 10, with 11.6 million reported cases and 7,043 deaths between 2008 and 201911.
While biological and epidemiological aspects of ZIKV and CZS are well-documented5 ^,^ 6 ^,^ 7 ^,^ 8 ^,^ 9 ^,^ 10, their demographic impacts remain less explored. Some studies suggest that fears of CZS and increased abortions led to delayed pregnancies, potentially contributing to declining birth rates12 ^,^ 13 ^,^ 14 ^,^ 15. For example, Brazil’s total fertility rate (TFR) dropped from 6.7 in 1960 to 1.7 in 201716 ^,^ 17, though this decline varied regionally. The Southeast region reached replacement-level fertility between 1995 and 2000, while other regions maintained higher rates16. Sociodemographic factors, such as education, urbanization, healthcare access, and sterilization procedures were identified as drivers of this fertility transition18. In the state of Ceará, in northeastern Brazil, TFR decreased over time, reaching 1.70 per 100 thousand women of childbearing age in 2018, compared to the national average of 1.7719 ^,^ 20. In the present study, we investigate the association between the ZIKV epidemic, fertility rates, and sociodemographic and behavioral factors influencing birth trends in Ceará to elicit regional policymaking for future outbreaks.
METHODS
Study setting, design and population
A cohort of women of reproductive age, who lived in areas of high vulnerability for arboviruses infection in Fortaleza, state of Ceará, Brazil, were enrolled. The study sample was recruited from a prospective cohort study, “ZIKA in Fortaleza (ZIF).” Briefly, four primary health care units (PHCUs) within Fortaleza, most affected by arbovirus infections caused by CHIKV, were chosen to participate in ZIF. Two of these PHCUs are in the Barra do Ceará, an urban neighborhood located in the second-most densely populated area of Fortaleza21. This neighborhood has a very low Human Development Index (HDI=0.22), with poor infrastructure, lack of sanitation, difficulty accessing water and need for water storage, unpaved and poorly maintained streets and failure to collect household waste, all of which are favorable conditions for the proliferation of Aedes aegypti 22 ^,^ 23. The third PHCU is in the Esperança complex, in Fortaleza’s southwest area, with a population of 16,405 inhabitants (HDI=0.29). The fourth PHCU is in Rodolfo Teófilo, a more economically-advantaged town with 19,114 inhabitants (HDI=0.48)23 ^,^ 24. Women who attended any of the four PHCUs were enrolled in February 2018 and two follow-up waves were conducted, with an average follow-up time of six months ending in August 2019.
The study sampling criteria included women:
- Living in the chosen PHCU area;
- Aged between 15 and 39 years, due to a greater chance of becoming pregnant;
- Being sexually active, defined as having at least one sexual relationship in the past 12 months;
- Having no tubal ligation or health problem that might prevent pregnancy; and
- Agreeing to participate in the study.
A probabilistic sample size of 1,497 women was estimated. More detailed information about sample calculation and design of the study is provided in a previous publication10.
Main outcomes
To analyze fertility rates among the sampled women over time, the time variable was subdivided into three periods following the epidemiology of Zika in Brazil24 ^,^ 25:
- Pre-epidemic period: from 2013 to 2014;
- Epidemic period: from 2015 to 2016; and
- Post-epidemic period: from 2017 to 2018.
“Fertility” for each woman was reconstructed using the birth history of each woman from 2013 on. In addition to the mother’s age and age at each birth, the authors thoroughly investigated up to five children reported born during the study recall period (2013-2018). Furthermore, we collected information about women’s pregnancies prior to 2013, the number of pregnancies that did not end in live births, and their pregnancy status at the time of interview. For all children, we collected information about sex, survival status, age (if alive), and age at death if deceased. Age at first birth was calculated as the difference between the birth date of the first-born child and the birth date of the women. Mean age at first birth (MAB) was defined as the average age at which the woman had her first pregnancy. To measure abortion, the questions “Have you had an abortion?” and “Have any of these abortions been induced?” were asked, using the WHO criteria26. By “spontaneous abortion,” the authors mean the involuntary termination of pregnancy, and “induced abortion” means the outcome of a deliberate interruption of pregnancy.
Independent variables
Women responded to a closed-ended questionnaire with the following four major components. First, socioeconomic and demographic variables were the age of the participant, educational attainment, race/ethnicity, socioeconomic status according to Brazilian criteria (Associação Brasileira de Estudos Populacionais [Brazilian Association of Population Studies] - ABEP)27 ^,^ 28, employment status, whether women were receiving cash transfers from the Bolsa Família program (a cash transfer program of the Brazilian government) or any other state program, marital status, household food insecurity based on the instrument of the United States Department of Agriculture (USDA)29, the number of residents and children in the household, and poverty. Poverty was classified as income BRL≤179 per capita per month, or approximately USD54/month (using Mid-year 2017 BRL/USD exchange rate), USD1.80 per day. Second,household sanitation variables included sewage disposal, water source, and water storage. Third, sexual and reproductive health variables were use of condom in the last sexual intercourse, frequency of condom use, use of repellent to prevent ZIKV, knowledge of contraceptive methods, type of contraceptive method, age at first live birth, pregnancy history, desire for pregnancy, pregnancy postponement, abortion (spontaneous and/or induced), and the reason (if any) to postpone her pregnancy. Fourth, medical history variables were family history of arbovirus infections, self-reported comorbidities, diagnosed chronic conditions (e.g., hypertension, asthma, cardiovascular disease, and diabetes), and use of illicit drugs and tobacco.
Statistical analysis
The authors reconstructed fertility trends of the sampled women, estimated differentials in fertility levels, and finally calculated the age-specific fertility rate (ASFR), TFR, and MAB for each age group, socioeconomic status (Brazilian ABEP criterion), self-reported race or skin color (white and non-white: Black, Indigenous, Asian, or mixed-race), and educational attainment (incomplete elementary school, complete elementary school, or higher education). Births in 2019 were censored due to the small number of births at the end of the study, which affected estimates, and because of the small proportion of women in the ZIF cohort who were waiting to give birth during the second wave of the study. For the study’s purposes, TFR, ASFR, and MAB rates were calculated for women between 15 and 39 years of age due to samples constrains. The equation and estimation approaches are described next.
First, the ASFR was calculated for five groups of five-year ranges: 15-19, 20-24, 25-29, 30-34, and 35-39 years of age (see Equation 1). ASFR represents the number of births occurring during a given year or a reference period per one thousand women-years of exposure for a specific age group. For each age group, where β_a_ denotes the number of births of women in age group a during the reference period30 ^,^ 31 ^,^ 32, and E_a_ denotes the number of women in age group a during the same reference period.
Second, the TFR was calculated, which is the number of children who would have been born per woman between 15 and 49 years of age if women were to pass through the childbearing years not subject to mortality (see Equation 2).
Third, MAB rates were computed, which consists in the average age at first birth at time (t), where b (a, t) denotes the age-specific birth rate for birth order one at (single) age a and time t, and a max denotes the highest age at which first births are observed (see Equation 3).
For the present study, TFR, ASFR, and MAB rates were calculated for women between 15 and 39 years of age due to the small number of women ≥40 years in the sample.
Finally, univariable (crude) and multivariate (adjusted) analyses were employed using Poisson regressions. The outcome variable was the number of children born by women of reproductive age. Risk ratios (RR) and their respective 95% confidence intervals (95%CI) were reported. The variables that were significant at p-value<0.05 univariately were adjusted in a final multivariate regression model (Table 1). All models were tested for multicollinearity using the variance inflation factor (VIF) and variables were kept if VIF<5.
Table 1.Age Specific Fertility Rate of women between 15 and 39 years of age from the “Zika in Fortaleza” cohort and between 2013 and 2018.Variable (n=1,497)2013-2014 2015-2016 2017-2018 p-value ASFR95%CIASFR95%CIASFR95%CIEducational attainmentIncomplete elementary school by age group15-190.210.15-0.280.260.19-0.330.180.12-0.23<0.00120-240.250.16-0.330.170.10-0.240.220.15-0.2925-290.130.07-0.200.090.04-0.150.180.11-0.2630-340.080.02-0.130.070.02-0.120.100.04-0.1635-390.150.01-0.360.030.01-0.090.080.03-0.14TFR4.212.93-5.483.242.57-3.923.893.17-4.61Complete elementary school or higher education by age group15-190.090.06-0.110.090.07-0.110.140.11-0.18<0.00120-240.120.09-0.150.130.10-0.160.160.13-0.2025-290.110.08-0.140.100.07-0.130.170.13-0.2130-340.060.03-0.090.100.06-0.130.130.09-0.1735-390.080.00-0.130.060.02-0.100.050.02-0.08TFR1.931.64-2.222.452.08-2.833.383.00-3.77Socioeconomic Status (SES)Low SES (D, E) by age group15-190.200.12-0.280.280.18-0.380.220.12-0.33<0.00120-240.150.07-0.220.180.09-0.260.240.15-0.3325-290.140.07-0.220.140.08-0.210.170.10-0.2530-340.010.01-0.040.100.02-0.170.090.03-0.1635-390.180.01-0.54 0.030.01-0.090.060.01-0.13TFR3.521.58-5.453.752.86-4.644.073.15-5.00High SES (A, B1, B2, C) by age group15-190.100.08-0.120.110.08-0.130.140.11-0.18<0.00120-240.140.11-0.170.130.10-0.160.160.13-0.1925-290.110.08-0.140.090.06-0.110.170.13-0.2130-340.070.04-0.100.090.06-0.120.130.09-0.1635-390.030.00-0.100.060.01-0.100.060.03-0.09TFR2.381.92-2.842.452.10-2.803.443.07-3.81ASFR: Age Specific Fertility Rate; TFR: Total Fertility Rates; p-value significance statistics=<5%, Poisson Regression Model; 95%CI: 95% confidence interval.
All data analyses were processed using the statistical package Stata v.17 (Stata Corporation, College Station, Texas, USA). Specifically, the fertility estimation method proposed by Schoumaker (2013) and the “tfr2” module for fertility rates were used.
Data Availability Statement
The data and codes used for the analysis of this study are available for public access with prior authorization from the principal investigator, Dr. Ligia Kerr, at the following link: https://github.com/kasimallel/Zikavirus_Fertility_Brazil/blob/main/README.md
RESULTS
Characterization of women’s sociodemographic profile
Of the 1,497 eligible women from the ZIF study, 1,175 women (78.4% of the first wave) completed the second wave of the study. In Table 2, we show the descriptive statistics of our final sample (1,497 women). Most women were under 29 years of age and had complete elementary education or higher (74.4%). Most women were non-white (88.6%), belonged to the middle or higher socioeconomic class (84.6%, A/B/C), 77.3% reported not working or being unemployed, 19.2% were extremely poor, and 29.1% lived on less than one minimum wage per month (equivalent to USD 170, or USD 5.70/day). Most participants received federal cash transfers, did not store water, and had one or two children (58%) by the age of 18 (35.2%) or 19-24 years (30.8%). One-third (31.8%) reported using condoms at the last sexual intercourse.
Table 2.Descriptive characteristics of women between 15 and 39 years of age from the “Zika in Fortaleza” cohort, Fortaleza (CE), Brazil, 2018.Variable n=1,497n%Age group, years (n=1,497)15-1931020.720-2441827.925-2932521.730-3425617.135-3918812.5Educational attainment (n=1,496)Incomplete elementary school 38325.6Complete elementary school or higher education1,11374.4Race or color of skin (n=1,487)White 17011.4Non-white 1,31788.6Socioeconomic status, ABEP criterion (n=1,497)Higher (A, B and C)1,26784.6Lower (D and E)23015.4Employment situation (n=1,497)Formal job1338.9Informal job 20613.8Does not work or is unemployed1,15877.3Beneficiary of the Bolsa Família program (n=1,497)Not a beneficiary67445.0Beneficiary82355.0Number of children (n=1,497)No children 42828.6One to two86958.0Three or more20013.4Used a condom in the last sexual intercourse (n=1,489)Yes47431.8No1,01568.2Use of condom frequency (n=1,488)Always31821.4Sometimes61841.5Never55237.1Wanted to get pregnant (n=1,475)Yes56238.1No 91361.9Had abortion (n=1,493)No90060.3Yes25417.0No history of pregnancy33922.7
At the time of the second interview, 77.3% of the participants reported they were pregnant, and 17% had a history of induced or spontaneous abortion. Only 2.1% reported postponing pregnancy for fear of ZIKV infection, while 14.1% reported postponing pregnancy due to an unfavorable economic situation. More than half (59.6%) had family histories of DENV, CHIKV, or ZIKV infections. Finally, a minority of women had comorbidities (20.6%) and had not used drugs (13.9%) or smoked tobacco (32.7%).
Fertility rates and mean age of first birth
We estimated a TFR of 2.9 births per 100 thousand women-years (95%CI 2.7-3.1) for the six years preceding the initiation of the cohort study. We observed a sustained increase between 2016 and 2018; from 2.8 (95%CI 2.4-3.2) to 3.8 (95%CI 3.4-4.4) (p<.001). The TFR during the epidemic ZIKV period experienced a slowdown relative to the pre-epidemic period and subsequently increased during the post-epidemic period (Table 3; Figure 1A). The TFR for 2013 was already 2.7; in 2014, we estimated a TFR of 2.4, and 2.5 in 2015; however, the TFR increased again in the post-epidemic period. In this sense, there was a slowdown in fertility rates compared to the pre-epidemic period, but there was stabilization during the epidemic years, followed by a subsequent increase in the TFR in the period following the peak of the ZIKV epidemic.
Table 3.Total Fertility Rates from the “Zika in Fortaleza” cohort according to their socioeconomic status and educational attainment.Variable (n=1,497)2013-2014 2015-2016 2017-2018 p-valueTFR95%CITFR95%CITFR95%CIEducational attainmentComplete elementary school or higher1.91.6-2.22.52.1-2.83.43.0-3.8<0.001Incomplete elementary school 4.22.9-5.53.22.6-43.93.2-4.6Socioeconomic statusHigh (A-B and C)2.41.9-2.82.42.1-2.83.43.1-3.8<0.001Low (D and E)3.51.6-5.53.82.9-4.64.13.2-5Race or skin colorWhite 1.50.8-2.12.41.5-3.33.92.9-50.310Non-white 2.82.1-3.42.72.3-33.53.1-3.8 Bolsa Família programNot a beneficiary1.41.1-1.71.91.4-2.33.52.9-4<0.001Beneficiary3.52.6-4.33.32.8-3.83.63.1-4Household food insecurityNo1.91.5-2.22.31.8-2.83.63.0-4.1<0.001Yes 3.22.3-4.03.22.6-3.74.23.6-4.8Loss to follow-up2.21.6-2.82.21.6-2.72.31.7-2.9Household residentsThree or less1.61.3-22.41.9-2.83.32.8-3.8<0.001Four or more3.42.5-4.22.92.4-3.33.73.2-4.1Poverty situationYes 3.42.3-4.54.23.2-5.24.93.9-5.8<0.001No2.31.7-2.92.21.9-2.63.63.1-3.9Water StorageYes2.72.1-3.33.12.5-3.83.53.1-3.9<0.001No2.51.8-3.22.52.1-2.83.602.9-4.3Used a condom in the last sexual intercourseYes3.51.8-5.32.61.9-3.33.102.5-3.7<0.001No2.21.9-2.52.72.3-3.03.663.2-4.1Wanted to get pregnantNo3.32.3-4.32.21.8-2.52.792.4-3.2<0.001Yes1.71.3-2.03.32.7-3.94.804.2-5.5TFR2.62.1-3.12.62.3-33.523.2-3.9<0.001TFR: Total Fertility Rates; 95%CI: 95% confidence intervals.
Figure 1.Total fertility rates* and age specific fertility rates^†^ of women aged 15 to 39 years from the “Zika in Fortaleza (CE)” cohort, reported between 2013 and 2018^‡^.*Rates computed per each year. Constant age fertility schedule was assumed. ^†^Age Specific Fertility Rates computed by 5-year periods; ^‡^MAB: Mean age at first birth. TFR: Total Fertility Rates; 95%CI: 95% confidence interval.
The ASFR was higher in the groups between 20 and 24 years of age (0.15 births per 100 thousand women-years), followed by the group of 15-19 years (ASFR=0.13). The ASFR declined in older women, particularly in the 30-34 (ASFR=0.09, 95%CI 0.08-0.11) and 35-39 age group (ASFR=0.06, 95%CI 0.03-0.08) (Figure 1B).
Differences in fertility rates were observed by women’s socioeconomic status in all periods studied, but particularly during the epidemic period. Women in socioeconomic classes D and E had higher fertility (TFR=3.8, 95%CI 2.9-4.6) compared to women of higher socioeconomic status (TFR=2.5 births per one thousand women, 95%CI 2.1-2.8) (Table 3; Figure 2). A similar situation occurred when comparing the MAB, suggesting that women from high socioeconomic status became pregnant at a later age (26 years, 95%CI 25.4-26.6), compared to women from lower socioeconomic status (MAB=24.2, 95%CI 23.1-25.4) (Figure 2).
Figure 2.Age Specific Fertility Rates* by socioeconomic status and educational attainment for women aged 15 to 39 years from the “Zika in Fortaleza (CE)” cohort between 2013 and 2018.*Rates computed per each year. ASFR: Age Specific Fertility Rate, computed by each year. Constant age fertility schedule was assumed; SES: Socioeconomic status.
There was a significant difference in fertility between women who were beneficiaries of the Bolsa Família program and women who experienced household food insecurity. We observed that female beneficiaries of the Bolsa Família program during the epidemic period had a TFR of 3.3 (95%CI 2.8-3.8) compared to non-beneficiaries (TFR=1.9, 95%CI 1.4-2.3; p<0.001). In turn, women who experienced food insecurity had a TFR of 3.2 (95%CI 2.6-3.7) compared to women who did not (p<0.001, Table 3). Overall, according to our findings, poor women had a TFR of 4.2 (95%CI 3.2-5.2) compared to less poor women (TFR=2.2, 95%CI 1.9-2.6). Women who had their first child before the age of 18 had higher fertility rates in the epidemic period (TFR=3.5, 95%CI 2.9-4.2) compared to women who had their first child after (2.83, 95%CI 2.3-3.3, Table 3).
Women having higher educational attainment had a lower fertility rate during the epidemic period (TFR=2.5, 95%CI 2.1-2.8) per one thousand women, compared to women with less educational attainment (TFR=3.2, 95%CI 2.6-3.9) (Table 3). Women with less educational attainment have had their children earlier, but also stopped having children earlier.
Social gradients and factors associated with fertility
According to our Poisson univariate regression analyses, fertility rates increased with lower educational attainment or socioeconomic status, unemployment, receiving cash transfers, higher number of people living in the household, and women’s age at the first live birth or whether they experienced abortion.
In our adjusted results we found that age and educational attainment are strong predictors of fertility (Table 4). Younger women between 15 and 19 years of age had 3.78 times higher adjusted odds of fertility, and women between 20 and 24 years had 3.23 times higher adjusted odds of fertility compared to older women (35-39 years, p<0.01) (Table 4). Those women from lower educational attainment status had 1.32 times higher adjusted odds of fertility compared to women with higher educational attainment (p<0.01). Women who lived with four or more people at the household had 1.22 times higher adjusted odds of fertility than those who lived with less than four people (p<0.01). The desire for pregnancy was associated with 19% lower adjusted odds of fertility (p<0.01).
Table 4.Poisson regression multivariate analysis of Total Fertility Rates in women from the “Zika in Fortaleza” cohort between 2013 and 2018.Variable (n=1,497)Model 1 Model 2* RR (crude)95%CIp-valueRR (adjusted)95%CIp-valueAge group35-391 <0.0011 <0.00130-341.71.2-2.51.91.3-2.725-292.61.7-42.61.7-4.020-243.21.9-5.23.21.9-5.515-193.72.2-6.43.72.2-6.3Educational attainmentComplete elementary school or higher education11<0.0511<0.001Incomplete elementary school 1.21.2-2.5 1.321.1-1.5Socioeconomic status, ABEP criterionHigher (A, B and C)11<0.05
Lower (D and E)1.21-1.4
Household residentsThree or less11<0.00111<0.001Four or more1.31.1-1.4 1.231.1-1.4Contraceptive methodsCondom or birth control pills11<0.001
Long-term1.41.2-1.6
Do not use1.21.0-1.4
Wanted to get pregnantYes 11<0.00111<0.001No0.80.74-0.9 0.80.7-0.9Had an abortionNo1 <0.00111<0.001Yes1.81.6-2.1 1.91.6-2.1*Model adjusted for the reproductive and sexual health variable and socioeconomic and demographic variables; 95%CI: 95% confidence interval; RR: risk ratios.
DISCUSSION
According to our results, the decline in fertility rates during the Zika epidemic in Brazil is evident. We demonstrated a strong association between the epidemic ZIKV period and fertility, in line with previous literature12 ^,^ 13 ^,^ 14 ^,^ 15. We observed a slowdown in fertility rates among women in the ZIF-cohort between 2015 and 2016, followed by an increase post-epidemic. Higher fertility rates in the last period may be due to age censoring. These findings support our hypotheses: women postponed pregnancy due to ZIKV risks, and fertility differs by socioeconomic status and level of education.
The observed slowdown of the fertility rate is consistent with recent studies carried out in the Northeast region, according to which there were 36,546 fewer births than expected12 ^,^ 13 ^,^ 15. This deficit in births showed important differences between highly and less affected regions by ZIKV, which demonstrates a potential association between the deficit of births and ZIKV and CZS cases. This decline in the TFR is also consistent with the official data on the number of live births in Fortaleza, where 39,548 live births occurred in 2015, dropping to 37,463 in 201633. The estimated TFR for Fortaleza was 44.5 in 2015, decreasing to 41.2 in 2016, indicating a decline in fertility during the epidemic period, as we show in the present study34.
TFRs were higher among poorer and less educated women; they were also higher at younger ages and declined as women approached 30 years of age. For poorer and less educated women in our cohort, pregnancy occurs earlier and more often than for richer and more educated women. Conversely, richer and more educated women postponed their pregnancy until the age of 30 years.
The poorest and less educated women and their infants were the groups most affected by the ZIKV epidemic and CZS. This phenomenon was produced by a range of factors including geography, class, and race, as demonstrated by the larger number of cases of microcephaly and infant deaths reported in the Northeastern states of Brazil. This is a product of inequity in the life conditions of these women, mainly Black and mixed-race women from low-income families10 ^,^ 35 ^,^ 36 ^,^ 37.
Researchers have reported the effects of the ZIKV epidemic on shaping the reproductive intentions of women in Brazil13 ^,^ 14 ^,^ 38. In addition, they also show an increasing racial vulnerability: Black and mixed-race women were more likely to postpone pregnancy than white women. We found very different results: 61.9% did not want to get pregnant, regardless of the ZIKV epidemic, and only 2.1% reported avoiding pregnancy due to the fear of ZIKV infection and CZS. Moreover, 17.1% of the women reported abortion, and 14% of these were reported as induced abortions.
We identified significant fertility disparities between women with low levels of education and socioeconomic status versus those with high levels of education and wealth. These disparities, influenced by race, gender, and class, highlight the need for sexual and reproductive health policies focused on human rights for women39 ^,^ 40 ^,^ 41. These findings are consistent with studies showing higher ASFR in younger women with lower levels of wage income14 ^,^ 15.
Many “emerging” countries in a post-transitional fertility regime experienced a decline in TFR below 1.72 children per woman42 ^,^ 43. This group includes all countries and regions of the world, except for Sub-Saharan Africa. Almost all countries in Latin America, with few exceptions (Bolivia, Guatemala, and Haiti), demonstrate decline along with improvements in women’s education and participation in the labor market42. However, according to the literature, fertility changes occur in response to shocks and as a consequence of economic crisis12 ^,^ 42 and public health emergencies44.
We highlight issues regarding contraceptive access, reflecting women’s autonomy and rights. Women using long-term methods, such as IUDs or diaphragms, had higher fertility than those using pills or condoms. Often older, they likely sought for more reliable birth control after completing their reproductive careers14 ^,^ 15.
While contraceptive methods are associated with fertility, we know that the economy plays a large role in the intendedness of pregnancy. We found that almost one third of the women in the ZIF-cohort were formally unemployed and more than two fifth of the sample did not work. This shows the diminished financial autonomy of these women as they were out of the labor market, degrading their ability to generate income associated with fertility and poverty’s intergenerational transmission14 ^,^ 15 ^,^ 45 ^,^ 46.
Brazilian women face vulnerabilities due to high maternal mortality, adolescent pregnancies, and limited access to legal abortion. These outcomes highlight inequality, poverty, and discrimination against Indigenous, Black, and adolescent women17 ^,^ 47. The intersection of gender, race, and education increases pregnancy risks. In many Latin American countries, including Brazil, El Salvador, and Honduras, abortion remains illegal, forcing secrecy and causing severe consequences, including death44 ^,^ 48 ^-^ 52.
Another expression of unequal power relationships is that adolescent pregnancy is high in vulnerable groups. Lower wealth quintiles, with less education, have more desired children and fewer unwanted pregnancies, while higher quintiles experience the opposite, leading to more unwanted pregnancies39 ^,^ 40 ^,^ 41. In contrast, authors of other studies have explained that poor pregnant adolescents in Latin America report higher levels of unintended pregnancy17 ^,^ 47. As expected, the answer to our research questions forces a discussion of a wide range of individual, collective, cultural, and structural factors that influence fertility, beyond contraception.
In this study, we showed that the ZIKV epidemic impacts fertility, with trends varying according to education and socioeconomic class. These factors highlight social inequalities in women’s sexual and reproductive health in arbovirus-endemic areas of northeastern Brazil.
Limitations
The present study has some limitations. While most studies on fertility use the age range of 15 to 49, our cohort included women 15-39, affecting absolute fertility values. We focused on childbearing-age women, especially those at higher risk of congenital Zika syndrome. Given the fertility decline after the age of 39, we prioritized higher fertility rates and excluded women aged 40 years or older.
Additionally, over 40% of the participating women had ZIKV infection, which further increased the risk of suffering the consequences of this infection for both women and their children. Still, the trend data are strongly indicative of the effect of ZIKV on fertility. Finally, a number of important variables concerning food insecurity that might affect fertility were only collected in the second wave, and retrospectively with regard to the time of the first wave, which could introduce misclassification bias.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica Nota informativa no 01/2015 - COES Microcefalias. Procedimentos preliminaries a serem adotados para a vigilência dos casos de microcefalia no Brasil[Internet]July 4, 2024 Available at: https://www.cosemspa.com.br/wordpress/wp-content/uploads/2015/11/microcefalia-nota-informativa-17nov 2015-c-1.pdf
- 2World Health Organization WHO statement on the first meeting of the International Health Regulations (2005) (IHR 2005) Emergency Committee on Zika virus and observed increase in neurological disorders and neonatal malformations[Internet]2016 July 4, 2024 Available at: http://www.who.int/mediacentre/news/statements/2016/1st-emergency-committee-zika/en/
- 3Garcia LP Instituto de Pesquisa Ecoômica Aplicada Ministério do Planejamento, Desenvolvimento e Gestão Epidemia do vírus zika e microcefalia no Brasil: emergência, evolução e enfrentamento[Internet]Brasilia Ipea 2018 July 4, 2024 Available at: http://repositorio.ipea.gov.br/bitstream/11058/8282/1/td_2368.pdf
- 4Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde Situação epidemiológica da síndrome congênita associada à infecção pelo vírus zika: Brasil, 2015 a 2023[Internet]Boletim Epidemiologico 2024555 July 04, 2024 Available at: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2024/boletim-epidemiologico-volume-55-no-05/view
- 5Araújo TVB Rodrigues LC Ximenes RAA Miranda-Filho DB Montarroyos UR Melo APL Association between Zika virus infection and microcephaly in Brazil, January to May, 2016: preliminary report of a case-control study Lancet Infect Dis 201616121356136310.1016/S 1473-3099(16)30318-827641777 PMC 7617035 · doi ↗ · pubmed ↗
- 6Musso D Ko AI Baud D Zika virus infection - after the pandemic N Engl J Med 2019381151444145710.1056/NEJ Mra 180824631597021 · doi ↗ · pubmed ↗
- 7Petersen LR Jamieson DJ Powers AM Honein MA Zika virus N Engl J Med 2016374161552156310.1056/NEJ Mra 160211327028561 · doi ↗ · pubmed ↗
- 8Oliveira WK França GVA Carmo EH Duncan BB Kuchenbecker RS Schmidt MI Infection-related microcephaly after the 2015 and 2016 Zika virus outbreaks in Brazil: a surveillance-based analysis Lancet 20173901009786187010.1016/S 0140-6736(17)31368-528647172 · doi ↗ · pubmed ↗