Association Between Stone Composition and Recurrence Rates Following Ureteroscopy: A Scoping Review
Althea O George, Mayowa Adefehinti, Minwook Lee, Ajibola A Adebisi, Ayodele Odedara, Raymond Omiko, Mobolaji Akinwale, Steven Ndonga, Adeyeye Olalekan, Abdulhameed Yusuf, Sahar Ali, Reginald Ononye, Daniel E Onobun

TL;DR
This review examines how different types of kidney stones affect recurrence rates after ureteroscopy, finding that calcium-based stones are linked to higher recurrence.
Contribution
The study identifies gaps in evidence regarding stone composition and recurrence, emphasizing the need for standardized research methods.
Findings
Calcium oxalate stones are associated with higher recurrence rates after ureteroscopy.
Recurrence rates varied widely, from 25.8% at 32 months to nearly 60% at 36 months.
Inconsistent reporting of uric acid, struvite, and cystine stones limits definitive conclusions.
Abstract
Urolithiasis remains a significant global health burden, with high recurrence rates following intervention. Ureteroscopy is increasingly preferred due to its safety and efficacy; however, recurrence after ureteroscopy is common and may be influenced by stone composition. This scoping review aims to explore the relationship between stone composition and recurrence rates post-ureteroscopy and to identify gaps in current evidence that could inform clinical practice and research. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews guidelines, we conducted a structured literature search (2014-2024) across PubMed, Scopus, MEDLINE, and Google Scholar. Studies were eligible if they reported on adult patients (≥18 years) undergoing ureteroscopy for renal or ureteric stones, provided stone composition data, and reported recurrence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
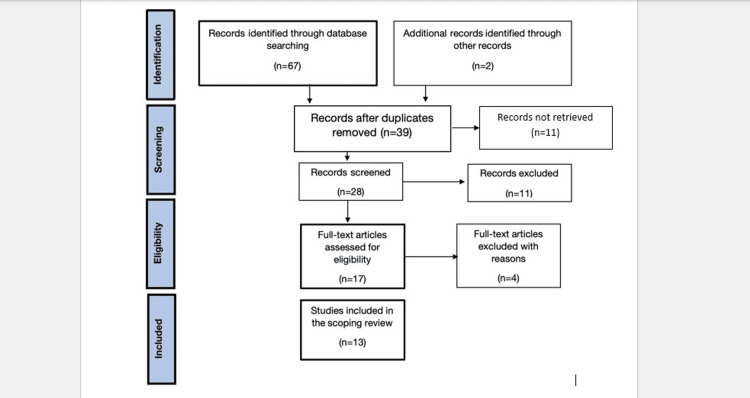 Figure 1
Figure 1| Search component | Keywords/Search terms | Boolean operators |
| Concept 1: Procedure | “ureteroscopy” OR “endoscopic stone removal” | OR |
| Concept 2: Stones | “urolithiasis” OR “renal calculi” OR “stone composition” | OR |
| Concept 3: Outcome | “recurrence” OR “recurrent stones” OR “stone recurrence” | OR |
| Combined search | (“ureteroscopy” AND “stone composition” AND “recurrence”) | AND |
| Reason for exclusion | Number of articles | Further explanation |
| Irrelevant to ureteroscopy or urolithiasis | 5 | These articles did not focus on ureteroscopy as a treatment modality for stone disease |
| No data on stone composition | 3 | Studies lacked detailed information about the chemical or mineral composition of stones |
| No outcome data on recurrence | 2 | Articles failed to report recurrence rates or follow-up outcomes after ureteroscopy |
| Small case series (n ≤ 10) | 1 | The study did not meet the sample size threshold defined for inclusion |
| Review articles, commentaries, or editorials | 2 | Non-empirical literature that did not present original data was excluded |
| Total | 13 | |
| Year | Authors | Title | Location | Methodology | Objectives |
| 2024 |
Skolarikosa et al. [ | Metabolic evaluation and recurrence prevention for urinary stone patients: An EAU guidelines update | Ireland (UK) | Qualitative | To define patients who are at a high risk of recurrence of urolithiasis by conducting a literature review that proposes to delineate diagnostic and therapeutic algorithms for each type of stone, with the aim of and to clarify general guidelines and recommendations for the prevention of recurrence |
| 2022 |
Baowaidan et al. [ | Incidence and risk factors for urolithiasis recurrence after endourological management of kidney stones: a retrospective single-centre study | France | Qualitative | To determine the recurrence rate of lithiasis after endourological management of nephrolithiasis and identify the risk factors for these recurrences |
| 2014 |
Vernez et al. [ | Nephrolithometric scoring systems to predict outcomes of percutaneous nephrolithotomy | USA | Qualitative | To develop a user-friendly system (S.T.O.N.E. Score) to quantify and describe stone characteristics provided by axial CT scan to predict ureteroscopy outcomes and to evaluate the characteristics that are thought to affect stone-free rates |
| 2017 |
Oliver et al. [ | Successful ureteroscopy for kidney stone disease leads to resolution of urinary tract infections: prospective outcomes with a 12-month follow-up | Southampton (UK) | Qualitative | To investigate the resolution of urinary tract infection with the successful treatment of kidney stone disease |
| 2017 |
Aggarwal et al. [ | Renal stones: a clinical review | India | Qualitative | To conduct a clinical review of the prevalence of urinary tract stones in India and provide more information on the illness |
| 2018 |
Alelign et al. [ | Kidney stone disease: an update on current concepts | Ethiopia | Qualitative | To evaluate the increasing rate of urological disorders of human health, affecting about 12% of the world population. Also, to explore the relationship between stone recurrence and an increased risk of end-stage renal failure |
| 2019 |
D’Costa et al. [ | Leave no stone unturned: defining recurrence in kidney stone formers | USA | Qualitative | To explore and investigate the various manifestations of kidney stone recurrence and the reported rates of kidney stone recurrence in various clinical settings |
| 2019 |
Fontenelle et al. [ | Kidney stones: treatment and prevention | Brazil | Quantitative | To investigate and assess the treatment and prevention of kidney stones, as they are becoming a prevalent disorder, with an annual incidence of eight cases per 1,000 adults |
| 2020 |
Nevo et al. [ | Patients treated for uric acid stones reoccur more often and within a shorter interval in comparison to patients treated for calcium stones | Canada | Quantitative | To investigate the association between stone composition and recurrence rate in a well-characterized group of patients |
| 2020 |
Lane et al. [ | Correlation of operative time with outcomes of ureteroscopy and stone treatment: a systematic review of literature | Southampton (UK) | Qualitative | To present the latest evidence related to the impact of increased operative times in retrograde intrarenal surgery and identify possible important factors that can facilitate ureteroscopy procedures |
| 2023 |
Kim et al. [ | Real-world practice stone-free rates after ureteroscopy: variation and outcomes in a surgical collaborative | Michigan (USA) | Mixed-method | To evaluate the stone-free rate for ureteroscopy and its predictors across diverse surgeons in Michigan |
| 2023 |
Ripa et al. [ | Role of ureteroscopy (URS) and stone treatment in patients with recurrent UTIs: outcomes over a 10-year period | Southampton (UK) | Quantitative | To assess whether the eradication of kidney stones might result in a substantial reduction in the onset of recurrent urinary tract infections |
| 2024 |
Achar et al. [ | Indications for intervention in patients undergoing ureteroscopic therapy for ureteric calculus: a cross-sectional study | India | Quantitative | To analyse the various indications for surgery, whether MET was used or not, if used-its details, operative findings at ureteroscopy, including the reason for the failure of MET |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Ureteral procedures and complications · Pediatric Urology and Nephrology Studies
Introduction and background
Kidney stone disease continues to place a considerable strain on urological services worldwide, not only due to its high prevalence but also because of its recurrent nature [1]. Despite advances in surgical management, long-term outcomes remain suboptimal in many patients, particularly those predisposed to recurrence. There is evidence that stone composition and metabolic profiles are determinants of recurrence risk [2]. As such, understanding its role in predicting recurrence is critical to informing postoperative follow-up and developing targeted strategies to reduce long-term stone burden [3].
The pathophysiology of stone disease is multifactorial, involving both intrinsic factors, such as genetic predisposition and metabolic derangements, and extrinsic contributors, including fluid intake, dietary habits, and environmental conditions [4]. Stone formation typically begins with urinary supersaturation of lithogenic solutes such as calcium, oxalate, and uric acid, leading to crystal nucleation, aggregation, and retention within the renal collecting system [5,6]. Clinically, patients may present with acute loin to groin colicky pain, haematuria, or chronic complications, such as recurrent urinary tract infections, hydronephrosis, or progressive renal impairment [7,8].
While multiple treatment modalities exist, including extracorporeal shockwave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), and ureteroscopy, the latter has become a cornerstone of modern endourology due to its minimally invasive nature and high stone-free rates [9]. Advancements in ureteroscopic technologies, particularly the widespread adoption of flexible ureteroscopes and laser lithotripsy (e.g., Holmium:YAG and Thulium fibre lasers), have further enhanced procedural outcomes. Nevertheless, recurrence following ureteroscopy remains a persistent clinical challenge, often attributable to a combination of metabolic, anatomical, and behavioural factors [7,10].
Importantly, the aim of this review is not to evaluate ureteroscopy itself, but rather to use it as a clinical context in which stone composition may influence recurrence outcomes. Recurrence is affected by factors such as stone type, metabolic risk profiles, obesity, diabetes, young age, and personal or family history of nephrolithiasis [10]. Despite the established role of composition in guiding preventive strategies, post-ureteroscopy follow-up remains variable and often lacks metabolic assessment or structured patient counselling [11,12]. Hence, this review aims to: (i) synthesise recurrence patterns by stone composition following ureteroscopy; (ii) evaluate how recurrence risk varies across stone types; and (iii) identify gaps to inform future research and practice.
Review
Methodology
Overview of Methodology
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines developed by Tricco et al. and was guided by the methodological frameworks proposed by Arksey and O'Malley and further refined by the Joanna Briggs Institute (JBI) [13,14]. These frameworks were selected to ensure transparency, methodological rigour, and reproducibility in mapping existing literature on stone composition and recurrence after ureteroscopy.
Protocol and Registration
This scoping review followed the PRISMA-ScR guidelines developed by Tricco et al. [14], ensuring transparency and methodological rigour. The protocol was informed by a preliminary literature scan and refined with input from experts in urology and systematic reviews. Although the review protocol was not registered, this decision aligns with PRISMA-ScR flexibility for exploratory scoping designs. Ethical approval was not required, as only publicly available data were used. All steps, from search to synthesis, were aligned with PRISMA-ScR to ensure a transparent and reproducible process.
Eligibility Criteria
This review was structured using the Population, Concept, and Context (PCC) framework recommended by the JBI.
Population: Adult patients (aged ≥18 years) undergoing ureteroscopy for ureteric or renal stones.
Concept: Stone composition (fully or partially reported) and recurrence rates defined radiologically, symptomatically, or via reintervention.
Context: Studies published between January 2014 and April 2024 in English.
Eligible study designs included retrospective and prospective observational studies, clinical trials, and large case series (n > 10). Exclusion criteria comprised case reports, reviews, editorials, conference abstracts without full text, non-English publications, and studies not primarily focused on ureteroscopy or without data on stone composition and recurrence.
Search Strategy and Information Sources
A comprehensive literature search was conducted across the following four electronic databases: PubMed, Scopus, MEDLINE (via Ovid), and Google Scholar. The search spanned publications from January 2014 to April 2024 to reflect current endourological practices. Grey literature was identified through Google Scholar, institutional repositories, and clinical trial registries. Reference lists of included studies were also screened to enhance coverage.
The search strategy used Boolean operators and MeSH terms, combining keywords for ureteroscopy, stone composition, and recurrence. Filters were applied to limit results to human studies, English-language studies, and relevant publication types. The final search was conducted on 30 April 2024. Full search strings are detailed in Table 1 and Appendix A.
The third phase involved grey literature searches via Google Scholar, institutional repositories, urology conference abstracts, and clinical trial registries to identify unpublished or ongoing studies. Reference lists of included articles and reviews were also manually searched to minimise publication bias.
Selection of Sources of Evidence
Study selection followed a structured two-phase screening process, i.e., title/abstract review and full-text assessment, guided by established scoping review frameworks. Two independent reviewers applied predefined inclusion criteria, resolving discrepancies through discussion or third-party adjudication to ensure objectivity and reduce bias.
Data Charting Process
A total of 13 studies were included in this scoping review after screening 69 records from databases and additional sources, with duplicates removed and exclusions documented. Data were charted based on author, year, country, study design, sample size, stone type, recurrence definitions, follow-up duration, recurrence rates, and recurrence-free survival.
Data Synthesis Strategy
Given the heterogeneity in study designs, recurrence definitions, follow-up durations, and outcome reporting across the included studies, a formal meta-analysis was not feasible. Instead, a descriptive, narrative synthesis was employed to summarise patterns in stone composition and recurrence rates. This approach is consistent with the aims of scoping review methodology, which prioritises breadth of evidence mapping over statistical aggregation. While this limits the ability to draw definitive conclusions or pooled estimates, it allows for the identification of key trends, thematic patterns, and gaps in the literature. Future studies with standardised methodologies and consistent outcome measures would be required to support a meta-analytic approach and strengthen the evidence hierarchy.
In accordance with PRISMA-ScR and JBI guidelines, no formal risk of bias assessment was undertaken, as the objective of this scoping review was to characterise the breadth and nature of available evidence rather than evaluate study quality. Most included studies were retrospective, and findings should be interpreted within that context.
Synthesis of Results
A total of 69 records were identified through database searches and supplementary sources. After removing duplicates, 39 unique studies remained and were screened for eligibility. Title and abstract screening excluded 11 studies that did not meet the inclusion criteria, leaving 28 for full-text review. Following a detailed assessment, 13 studies met all inclusion criteria and were included in the final synthesis. Reasons for exclusion at the full-text stage included absence of recurrence data, lack of stone composition detail, or insufficient sample size.
Data were synthesised using a descriptive analytical approach. Studies were grouped by stone composition, recurrence definitions, and follow-up duration to identify thematic patterns and common findings across heterogeneous data sources. Evidence mapping is presented in Table 2.
Results
PRISMA-ScR Flow Diagram
The PRISMA-SCR flow diagram presented in Figure 1 illustrates the detailed explanation of the search decision and the record selection process.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) flow diagram.
Summary of Study Characteristics
The included studies varied in design and setting, with most being retrospective observational studies. Geographic representation spanned Europe, Asia, North America, and Africa. Sample sizes ranged from 45 to 300 patients. Table 3 summarises key characteristics, including study location, methodology, and objectives.
Frequency of Stone Composition
Calcium oxalate stones, particularly the monohydrate subtype, were the most frequently reported across studies. Baowaidan et al. identified calcium oxalate monohydrate in 23.2% of patients, followed by mixed stones (20.5%), calcium oxalate dihydrate stones (6.8%), and uric acid stones (5.8%) [10]. Other studies, including Kim et al. and Skolarikos et al., corroborated the predominance of calcium oxalate stones [2,23]. Uric acid, struvite, cystine, and brushite stones were underrepresented or not stratified in several studies, highlighting a limitation in composition-specific analysis [23,25].
Recurrence Stratified by Stone Type
Recurrence rates varied widely across the studies. For example, Baowaidan et al. reported a 25.8% recurrence rate over a median of 32 months, while Skolarikos et al. cited recurrence approaching 60% at 36 months in patients without metabolic follow-up [2,10,23]. Calcium oxalate stones were consistently associated with higher recurrence risk, though few studies stratified recurrence rates by specific subtypes [23].
Nevo et al. found that uric acid stone-formers experienced recurrence earlier and more frequently than those with calcium oxalate stones [21]. However, most studies lacked sufficient detail on recurrence rates for non-calcium stone types, limiting generalisability. This underreporting underscores the need for standardised compositional reporting.
Reporting and Follow-Up Gaps
A key limitation across included studies was heterogeneity in recurrence definitions and follow-up duration. Follow-up periods ranged from four weeks to over five years, and recurrence was variably defined as radiological detection, symptomatic presentation, or need for re-intervention. Early recurrences (<6 weeks) were often not differentiated from residual fragments, which may have inflated reported recurrence rates.
Furthermore, metabolic evaluation was inconsistently reported. Only a minority of studies incorporated metabolic profiling or preventive strategies. This gap highlights the limited integration of recurrence prevention protocols in routine follow-up after ureteroscopy.
Overall, the review identifies recurring methodological limitations: inconsistent recurrence definitions, underreporting of non-calcium stone types, and inadequate follow-up strategies. Addressing these issues is critical for improving recurrence risk stratification and personalising postoperative surveillance.
Discussion
Interpretation of Findings
This scoping review highlights the prevailing patterns of stone composition and their potential association with recurrence following ureteroscopy, while also revealing substantial gaps in consistency and methodology across studies. Notably, calcium-based stones, especially calcium oxalate, were consistently identified as the dominant stone type, aligning with global epidemiological data suggesting they account for over 70% of urolithiasis cases. Their high recurrence risk, as demonstrated by Skolarikos et al. and Baowaidan et al., reinforces the importance of long-term surveillance and metabolic evaluation, particularly in patients forming calcium oxalate monohydrate stones [2,10].
This association underscores a key theme: recurrence is not solely the result of surgical failure or residual fragments, but rather a reflection of ongoing metabolic imbalance [7,26]. Therefore, managing stone disease extends beyond the procedural endpoint; it necessitates a multidisciplinary approach involving urologists, nephrologists, dieticians, and primary care providers. Yet, despite the established link between stone composition and metabolic profile, only a minority of studies integrated metabolic workup or preventive strategies such as dietary counselling or pharmacotherapy into their analysis.
Beyond calcium oxalate, the representation of other stone types, such as uric acid, struvite, cystine, and mixed stones, was inconsistent and often inadequately reported. Uric acid stones, though potentially responsive to alkalinisation therapy, were rarely stratified in recurrence outcomes [21]. Similarly, infection-related struvite stones and hereditary cystine stones were too infrequent to draw meaningful conclusions.
Another major limitation across the reviewed literature was the lack of standardisation in defining and measuring recurrence. Follow-up durations varied from as short as four weeks to several years, and recurrence definitions ranged from imaging-confirmed new stones to symptomatic presentation or treatment failure. Notably, recurrence identified within very short intervals, such as four weeks postoperatively, likely represents residual fragments rather than true recurrence. For instance, Baowaidan et al. reported a 25.8% recurrence over a median of 32 months, while Skolarikos et al. cited rates nearing 60% over three years in patients without metabolic correction [2,10]. Without consistent assessment of stone-free status post-ureteroscopy, especially in the early postoperative period, these findings risk misclassification, which undermines comparability and weakens generalisability across populations.
Ultimately, while this review affirms that calcium oxalate stones are both the most prevalent and most prone to recurrence following ureteroscopy [3], the strength of this conclusion is limited by inconsistencies in study design, outcome reporting, and lack of integration between stone composition and broader metabolic context. Future research must aim to stratify recurrence risk by stone type using standardised definitions and incorporate comprehensive postoperative metabolic assessment. Doing so will allow for more precise follow-up strategies and better-informed recurrence prevention protocols in clinical urological practice.
Clinical Implications
The findings of this scoping review carry important implications for the clinical management of patients undergoing ureteroscopy. While ureteroscopy remains an effective intervention for stone clearance, the evidence highlights that recurrence risk, particularly in calcium oxalate stone-formers, must be anticipated and managed beyond the operative episode. Stone composition is not merely a descriptive pathology but a clinical marker that should guide long-term surveillance, preventive strategies, and patient education [27].
The consistently high recurrence observed in patients with calcium oxalate stones, as reported in some studies, suggests the need for structured, stone-type-specific follow-up. These patients often have underlying metabolic derangements, such as hyperoxaluria or hypocitraturia, which are modifiable but frequently unassessed. Therefore, integrating routine stone analysis, metabolic evaluation, dietary counselling, and pharmacological prophylaxis, such as thiazides or citrate therapy, into the postoperative care plan is essential to reduce recurrence risk [2,28].
However, the review also exposes a recurring clinical oversight: inconsistent or absent stone composition reporting. In many studies, stone fragments were either not retrieved or not analysed, representing a missed opportunity to personalise care. This gap is particularly concerning in high-risk populations, where early identification of stone type could directly inform preventive strategies [29].
Equally important is the role of patient education. Post-ureteroscopy counselling remains sporadic, yet structured education on fluid intake, dietary modification, and medication adherence is proven to reduce recurrence. Preventing future stone episodes requires more than surgical skill; it demands active, multidisciplinary collaboration involving urologists, nephrologists, dietitians, and primary care providers [30,31].
Finally, these clinical insights highlight a research gap [4,31]. There is a pressing need for prospective studies and randomised controlled trials evaluating the impact of stone composition-based surveillance on recurrence rates and long-term outcomes. Much of the current evidence is retrospective and lacks granularity on follow-up practices and intervention efficacy. Moving forward, routine integration of stone analysis and metabolic profiling should be standard care in endourology to shift the paradigm from stone removal to recurrence prevention [19,32].
Research Gaps and Future Directions
This review revealed key gaps limiting the strength of current evidence on stone composition and recurrence after ureteroscopy. Inconsistent or incomplete reporting of stone composition was common, hindering accurate risk stratification. Definitions of recurrence varied widely, radiological, symptomatic, or intervention-based, making cross-study comparisons difficult. Follow-up durations lacked standardisation and rarely addressed late or side-specific recurrence. Most studies were retrospective and lacked integration of patient-specific factors such as metabolic profiles and comorbidities, limiting insights into personalised recurrence risk and long-term outcomes. Prospective, standardised research is needed to address these limitations.
Strengths and limitations
This scoping review employed a comprehensive, multi-database search strategy and adhered to PRISMA-ScR guidelines, enhancing its methodological transparency and reproducibility. By focusing specifically on stone composition and recurrence after ureteroscopy, it addresses an important but underexplored clinical issue. The inclusion of studies across diverse populations adds to the generalisability of findings, and the synthesis of recurrence data by stone type offers practical insights.
However, several limitations must be acknowledged. First, the heterogeneity in study design, follow-up duration, recurrence definitions, and outcome reporting limits the comparability and strength of conclusions. Most included studies were retrospective and lacked uniform definitions of recurrence, making synthesis challenging. Second, the absence of consistent stone-free rate reporting is a significant limitation. Without clear documentation of post-procedural stone-free rate, particularly in studies with short follow-up durations, it is difficult to differentiate between true recurrence and residual fragments, potentially confounding recurrence estimates.
Additionally, patient-level factors such as metabolic evaluations, comorbidities, or adherence to preventive strategies were infrequently reported. Language bias is also present, as only English-language studies were included due to translation constraints. Despite these limitations, the review provides a valuable foundation for informing tailored follow-up protocols and future research design.
Conclusions
Calcium oxalate stones, particularly the monohydrate subtype, were the most frequently reported in the literature and appeared to be associated with higher recurrence following ureteroscopy. However, recurrence data were inconsistently stratified by stone composition, and most evidence was drawn from retrospective studies. Other stone types, such as uric acid, calcium phosphate, cystine, and struvite, were underreported or lacked sufficient recurrence data to allow definitive conclusions. These findings highlight the need for stone-type-informed follow-up strategies, with calcium oxalate stone-formers potentially benefiting from more structured metabolic evaluation, dietary counselling, and imaging surveillance. However, due to limited and heterogeneous data for non-calcium stones, recommendations for these subtypes remain tentative. This review underscores the importance of routine stone analysis and calls for more prospective research using standardised definitions of recurrence and consistent stone composition reporting. Such efforts are essential to advance personalised post-ureteroscopy care and improve long-term outcomes in patients with urolithiasis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Determining the true burden of kidney stone disease Nat Rev Nephrol Thongprayoon C Krambeck AE Rule AD 736746162020 https://www.nature.com/articles/s 41581-020-0320-73275374010.1038/s 41581-020-0320-7 · doi ↗ · pubmed ↗
- 2Metabolic evaluation and recurrence prevention for urinary stone patients: EAU guidelines Eur Urol Skolarikos A Straub M Knoll T Sarica K Seitz C Petřík A Türk C 750763672015 https://linkinghub.elsevier.com/retrieve/pii/S 03022838140110262545461310.1016/j.eururo.2014.10.029 · doi ↗ · pubmed ↗
- 3Recurrence rates of urinary calculi according to stone composition and morphology Urolithiasis Daudon M Jungers P Bazin D Williams JC Jr 459470462018 http://link.springer.com/10.1007/s 00240-018-1043-02939233810.1007/s 00240-018-1043-0PMC 6711148 · doi ↗ · pubmed ↗
- 4Renal stone disease Nephron Physiol Sayer JA 044118201110.1159/00032090221071986 · doi ↗ · pubmed ↗
- 5Kidney stone formation—thermodynamic, kinetic, and clinical aspects Water-Formed Deposits: Fundamentals and Mitigation Strategies Oner M Koutsoukos PG Robertson WG 511541 New York Elsevier 52022 https://linkinghub.elsevier.com/retrieve/pii/B 9780128228968000352
- 6A review of types, mechanisms, complications, and management of renal stone formation Egypt Acad J Biol Sci C Physiol Mol Biol Elgendy A Nabil Z Gad El-Hak H Nafie M El-Shenawy N 313321162024 https://eajbsc.journals.ekb.eg/article_350197.html
- 7Burden of urolithiasis: trends in prevalence, treatments, and costs Eur Urol Focus Raheem OA Khandwala YS Sur RL Ghani KR Denstedt JD 182632017 https://linkinghub.elsevier.com/retrieve/pii/S 240545691730086 X 2872036310.1016/j.euf.2017.04.001 · doi ↗ · pubmed ↗
- 8The stone hospital and stone treatment Urolithiasis Moran ME 145161 New York, NY Springer 2025