Lipomyelomeningocele in a Newborn: A Case Report
Karla V Soria, Ignacio J Contreras, Andrew Kobets, Lourdes Cohen

TL;DR
A newborn diagnosed with lipomyelomeningocele underwent successful surgery early, emphasizing the importance of timely treatment.
Contribution
This case report adds to the clinical understanding of LMMC through a successful neonatal surgical intervention.
Findings
Early surgical intervention in a neonate with LMMC resulted in a successful outcome.
The case underscores the importance of prompt diagnosis and treatment for LMMC.
No adverse outcomes were observed following the surgical repair.
Abstract
Lipomyelomeningocele (LMMC) is an uncommon type of closed spinal defect that falls under the broader category of spine bifida. This congenital condition may present at birth as a lumbosacral mass or manifest later in life with neurologic symptoms. In this report, we describe a neonate who was diagnosed with LMMC at birth and underwent timely surgical intervention during the neonatal period. The procedure was successful and the patient experienced no adverse outcome. This case highlights the importance of early diagnosis and prompt surgical repair.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
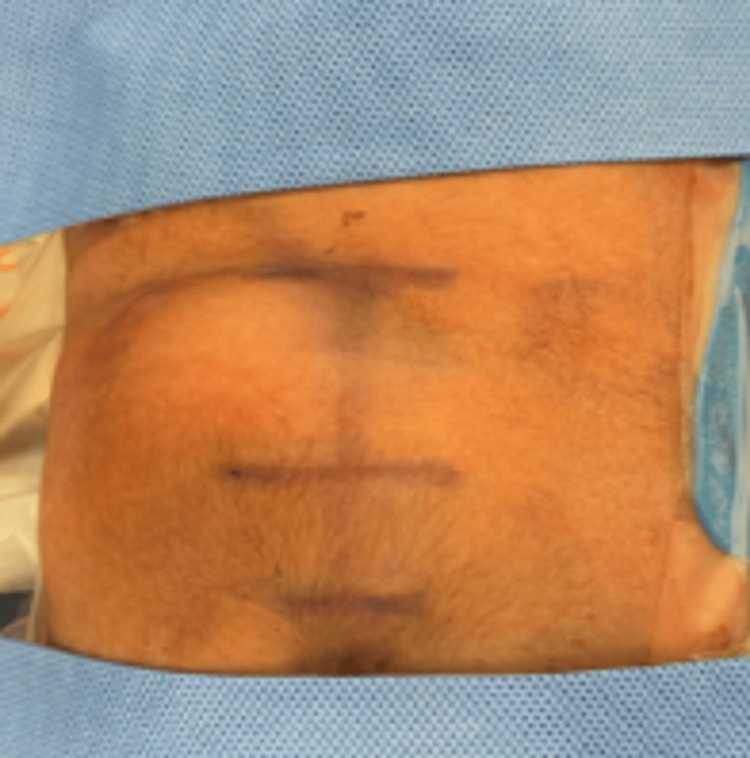 Figure 1
Figure 1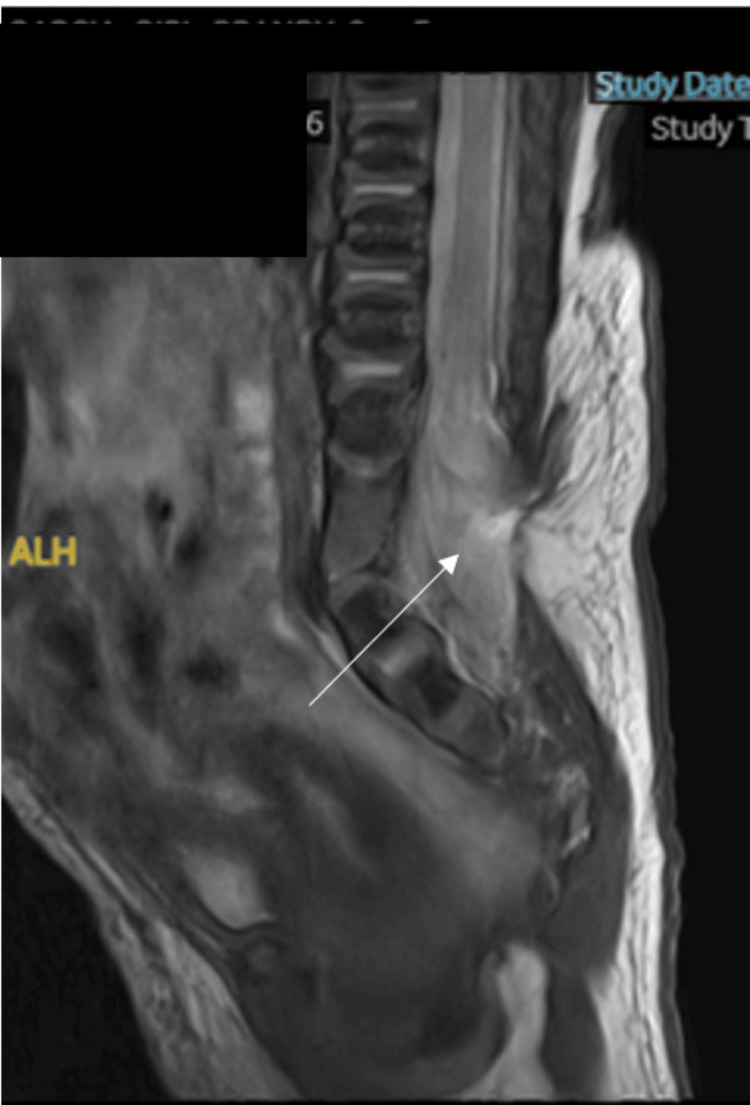 Figure 2
Figure 2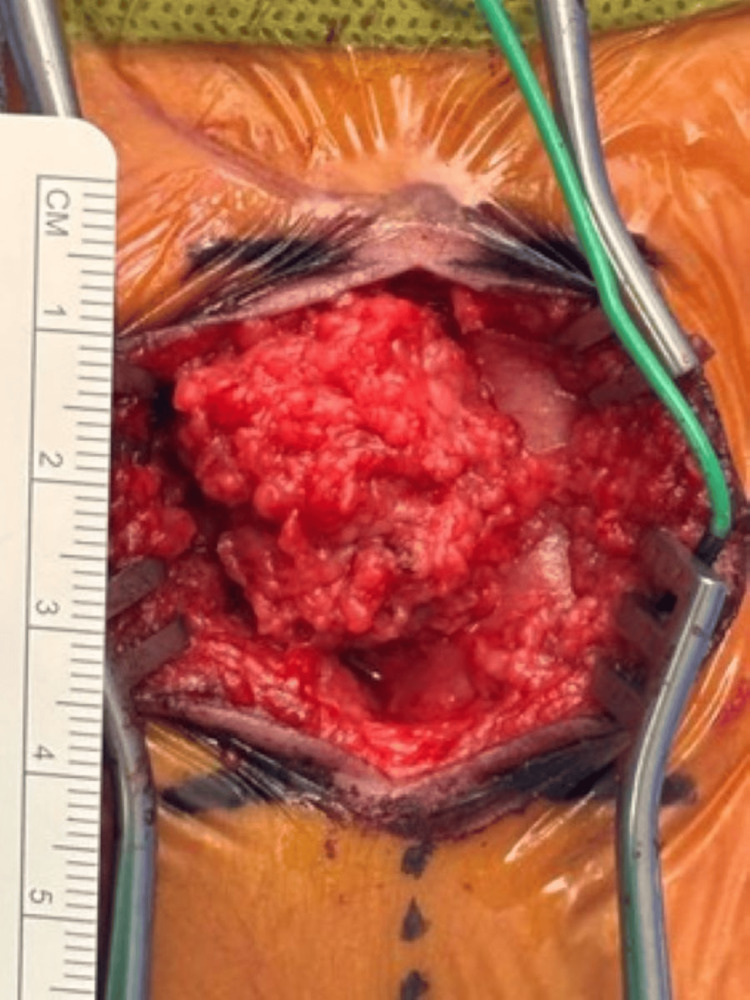 Figure 3
Figure 3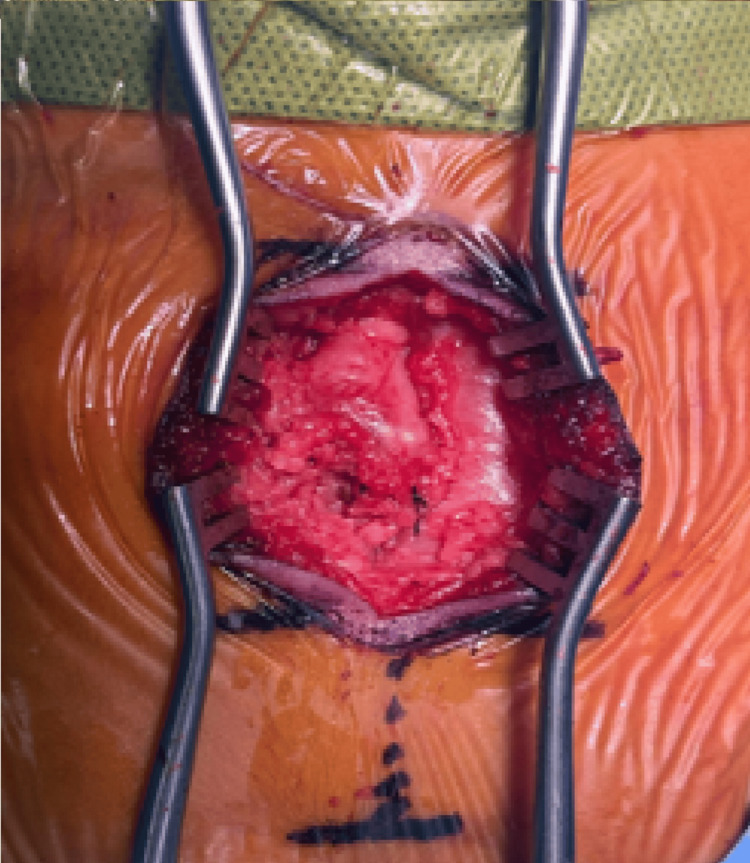 Figure 4
Figure 4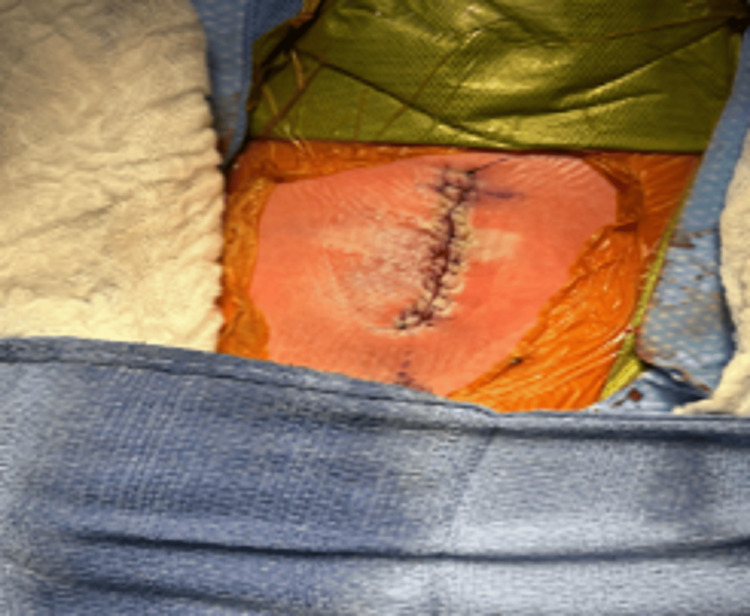 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Congenital Anomalies and Fetal Surgery · Teratomas and Epidermoid Cysts
Introduction
Lipomyelomeningocele (LMMC) is a type of closed neural tube defect, where neural elements are integrated into a spinal lipoma. This rare condition affects one to six individuals per 100,000 live births. It is a closed defect due to abnormal central nervous system development, involving primary or secondary neurulation. During primary neurulation, the neural tube forms and the ectoderm separates to create the skin of the spine. If disjunction occurs, mesoderm can enter the neural tube and create a lipoma that disrupts normal anatomy. Secondary neurulation is the formation of the spine below S2 through the cavitation and fusion of mesoderm with the primary neural tube. This process can be interrupted by mesoderm migration. Secondary neurulation is not completely understood, however, there are some theories suggesting the involvement of morphogenetic determinants, with potential key genes including Sonic Hedgehog and Pax family transcription factors [1]. In LMMC, the neural-lipoma junction is outside the spinal canal, extending dorsally through a bony defect. The lipoma exits the dura defect, passes through a fascial defect, and connects with subcutaneous tissue, tethering the spinal cord and making it vulnerable to stretch injuries during growth or repetitive movements [1].
LMMCs are classified into four types, as described by Chapman, depending on the location of the neural-lipoma interface: (1) dorsal, if the interface is at the dorsum of the spinal cord and the conus medullaris is spared; (2) caudal, if the filum terminal or the conus medullaris is involved; (3) transitional, when dorsal and caudal components are involved with nerve roots crossing the lipoma; and (4) where the spinal cord exits the spinal canal distally within the fatty mass [2].
Case presentation
A 26-year-old Hispanic woman, gravida 2, para 0, presented at 40 weeks gestation for an elective induction of labor. Due to prolonged labor course, a low transverse cesarean section was performed. The pregnancy was complicated by the presence of uterine fibroids. A first-trimester prenatal ultrasound was normal; however, during the second trimester, fetal sac views were suboptimal, raising concerns about a possible spinal abnormality.
A female infant weighing 3075 grams was delivered by cesarean section. Apgar scores were 9 at both 1 and 5 minutes. The placenta was intact.
On admission physical exam, a closed sacral dimple with a left palpable soft mass in the lumbosacral region was noted (Figure 1). Left hip examination was positive for a click. Complete neurological examination was within normal limits, including deep tendon reflexes and sensation.
A 4x3.5 cm circular, soft, nontender, nonpulsatile mass to right of lumbosacral region
Ultrasound confirmed left hip dysplasia and suspected spinal dysraphism. Brain MRI findings were within normal limits. MRI of the spine demonstrated a low-lying conus medullaris and a large posterior bony defect in the lower lumbar region, through which the spinal cord was herniated. The distal spinal cord was tethered to the posterior spinal elements. No evidence of syringomyelia or cerebellar tonsillar descent was observed, supporting the diagnosis of LMMC (Figure 2).
Spine MRI
She was transferred at six days of life (DOL) to a higher level of care hospital for surgical repair. The procedure was performed with no complications. A large lipomatous mass enveloped in the neural placode of the spinal cord was found intraoperative (Figure 3).
Lipomatous tissue encasing the neural placode
The cord was carefully dissected from the lipoma, allowing it to bring the dura and cord back into the spinal canal and to a normal anatomic position (Figure 4).
Spinal cord dissected from the lipoma
The closure of the fat layers and sealing of the dura was performed, followed by an additional resection of the remaining fat to achieve a cosmetically appealing closure (Figure 5).
LMMC repaired and closedLMMC: lipomyelomeningocele
She was discharged, and subsequent follow-up visits revealed normal neurologic examinations, with no evidence of motor or sensory compromise.
Discussion
Our case report identified a neonate who presented with a paraspinal mass at the time of birth associated with left hip dysplasia. MRI confirmed the diagnosis of LMMC.
This case is in accordance with the epidemiology of LMMC and other forms of closed spinal dysraphism which indicate higher frequency among individuals of Hispanic ethnicity compared to non-Hispanic White populations. This characteristic suggests a potential ethnic, genetic, environmental, or socioeconomic association that is not fully understood and warrants further research [3].
Our case was not associated with Chiari malformation which can occur in 13%, spinal dermal sinuses, anal stenosis (1%), or Down syndrome (1%). We did not find any visible capillary malformation, infantile hemangioma, or any other caudal malformations of organ systems like, cloacal exstrophy, VACTERL (vertebral defects, anal atresia, cardiac defects, trachea-esophageal fistula, renal anomalies, and limb abnormalities) [4,5].
The patient had a successful surgical repair on day 10 of life. The surgical management of LMMCs remains controversial, especially in patients with asymptomatic diseases. Various studies have suggested risks of progressive neurologic, urologic, and orthopedic deficits in patients with LMMCs if untreated. Other studies have shown progressive neurologic and urologic deficits in patients who were operated on prophylactically as well [6,7]. These variable outcomes may be due to the different symptoms that were assessed, the duration of follow-up, the type of malformation, and the timing of surgery [8].
Factors that may affect the treatment outcome of LMMCs include age, gender, morphology, the presence and severity of neurological symptoms, and the absence and presence of an associated spinal cord syrinx, of which the morphology is considered the most crucial factor affecting outcome [1]. One study suggests that those with symptomatic LMMCs had improvement or preservation of their pre-operative neurological function at follow-up visits, especially if corrected soon after the development of the deficit [9]. Some neurosurgeons suggest that early surgical intervention can be performed prophylactically to prevent neurological sequelae secondary to a tethered cord [10].
Conclusions
This case report describes the successful neonatal surgical management of an asymptomatic infant with LMMC, without evidence of spinal cord syrinx. The favorable outcome contributes to the growing body of literature on early intervention strategies for neonates with LMMC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Surgical management of lipomyelomeningocele in children: Challenges and considerations Surg Neurol Int Wagner KM Raskin JS Hansen D Reddy GD Jea A Lam S 6382017 https://doi.org/10.4103/2152-7806.2052682854012910.4103/2152-7806.205268 PMC 5421405 · doi ↗ · pubmed ↗
- 2Congenital intraspinal lipomas: anatomic considerations and surgical treatment Child's Brain Chapman PH 3747919827060411 · pubmed ↗
- 3Findings from the National Spina Bifida Patient Registry 6 2025 Centers for Disease Control and Prevention. Findings from the National Spina Bifida Patient Registry 2024 https://www.cdc.gov/spina-bifida/data/findings-from-the-nsbpr-registry.html
- 4Congenital brain and spinal cord malformations and their associated cutaneous markers Pediatrics Dias M Partington M 0191362015 https://doi.org/10.1542/peds.2015-191410.1542/peds.2015-285426416933 · doi ↗ · pubmed ↗
- 5Critical analysis of the Chiari malformation type I found in children with lipomyelomeningocele J Neurosurg Tubbs RS Bui CJ Rice WC Loukas M Naftel RP Holcombe MP Oakes WJ 196200106200710.3171/ped.2007.106.3.19617465384 · doi ↗ · pubmed ↗
- 6Lipomyelomeningocele—controversies in management Indian J Neurosurg Singh A Ghosh SN Chaudhuri AK Sadique SI Chaudhuri S 3542018
- 7Lipomyelomeningocele Neurosurg Clin N Am Sutton LN 32533861995 https://pubmed.ncbi.nlm.nih.gov/7620357/7620357 · pubmed ↗
- 8Cord untethering for lipomyelomeningocele: expectation after surgery Neurosurg Focus Cochrane DD 023200710.3171/FOC-07/08/E 917961013 · doi ↗ · pubmed ↗