Lung Function in a Multiethnic U.S. Cohort of Adolescents and Adults Born Preterm in the New BPD Era
Nataly J. Sanchez‐Solano, Tyler J. Wall, Gregory P. Barton, Dan M. Dane, Connie C. W. Hsia, Kara N. Goss

TL;DR
This study finds that adults born preterm, especially non-Hispanic Black individuals, are more likely to have lung function issues compared to those born at term.
Contribution
The study provides new insights into lung function in a multiethnic U.S. cohort of preterm-born individuals in the modern BPD era.
Findings
Preterm participants were more likely to have obstructive or restrictive ventilatory defects compared to term participants.
Non-Hispanic Black preterm participants had worse lung function than Hispanic White preterm participants.
Neonatal factors like bronchopulmonary dysplasia and low weight for gestational age were linked to reduced lung function.
Abstract
Extreme preterm birth is a recognized risk factor for reduced pulmonary function over the lifespan. However, data are lacking in U.S.‐born adults and in multiethnic populations. To comprehensively evaluate lung function in adolescents and young adults born premature, and to assess for potential impact of neonatal, racial/ethnic, and socioeconomic risk factors on long‐term lung function. Preterm participants aged 12–40 years of age were recruited from the Parkland Hospital Neonatal ICU Registry (Dallas County, Texas). Preterm and term‐born participants completed pulmonary function testing including spirometry, lung volumes, diffusion capacity, and respiratory muscle forces, using Global Lung Initiative race‐neutral reference equations. Influence of racial/ethnic background, neonatal factors, and socioeconomic ratings were assessed for preterm participants. Preterm participants (n =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
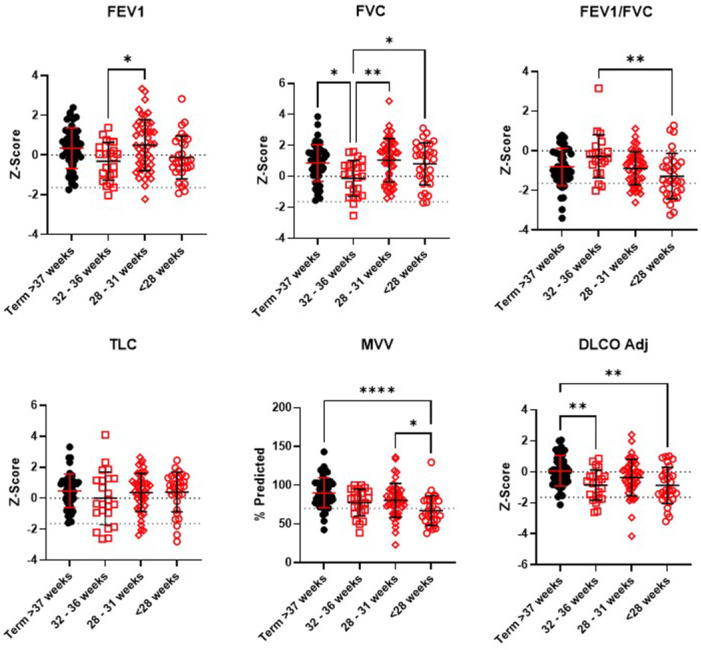 Figure 1
Figure 1| Enrollment characteristics | Term ( | Preterm ( |
| Preterm Non‐Hispanic Black ( | Preterm Hispanic ( |
|
|---|---|---|---|---|---|---|
| Age, mean (range) | 29 (13–40) | 26 (16‐36) |
| 30 (21–34) | 24 (16–35) |
|
| Birth year, mean (range) | 1994 (‘82‐’09) | 1996 (‘86‐‘06) |
| 1991 (‘87‐‘01) | 1998 (‘86‐‘06) |
|
| Female, | 29 (60.4) | 70 (66.7) | 0.47 | 22 (78.6) | 45 (64.3) | 0.23 |
| Hispanic/Latinx ethnicity, | 16 (33.3) | 70 (66.7) |
| 0 (0) | 69 (100) |
|
| Race, |
|
| ||||
| Black or African American | 5 (10.4) | 28 (26.7) | — | 27 (100) | 0 (0) | — |
| White | 30 (62.5) | 73 (69.5) | — | — | — | — |
| Asian | 9 (18.8) | 3 (2.9) | — | — | — | — |
| Other | 4 (8.3) | 1 (1.0) | — | — | — | — |
| Height, mean (SD), cm | 170 (10) | 162 (10) |
| 168 (11) | 160 (9) |
|
| Weight, mean (SD), kg | 74.3 (16.3) | 79.2 (23.4) | 0.14 | 92.4 (29.8) | 74.1 (19.2) |
|
| BMI, mean (SD), kg/m2 | 25.7 (4.5) | 29.9 (7.4) |
| 32.7 (9.4) | 28.9 (6.5) |
|
| Current or former smoker, | 10 (20.8) | 35 (33.3) | 0.13 | 13 (41.9) | 18 (25.7) | 0.05 |
| Self‐reported asthma diagnosis, | 4 (8.3) | 29 (27.6) |
| 9 (32.1) | 16 (22.9) | 0.44 |
| Handgrip strength, mean (SD), kg | 37.2 (12.9) | 32.9 (11.2) |
| 34.9 (12.3) | 30.8 (10.0) | 0.10 |
|
| ||||||
| Birth weight, mean (SD), g | 3332 (468) | 1311 (396) |
| 1351 (389.1) | 1277 (391.3) | 0.40 |
| Gestational age (GA), mean (SD), weeks | 39.2 (1.1) | 29.5 (2.5) |
| 30.4 (1.1) | 29.1 (2.5) |
|
| Small for gestational age, | 5 (11) | 33 (31) |
| 8 (29.6) | 24 (34.8) | 0.81 |
| Weight for GA Z‐score (SD) | −0.02 (1.14) | −0.85 (1.65) |
| −1.50 (1.7) | −0.66 (1.6) |
|
| Weight for GA %ile (SD) | 49.3 (30.0) | 34.6 (32.6) |
| 21.0 (22.6) | 38.3 (34.8) |
|
|
Characteristic | Total ( | Registry ( | Enrolled ( |
|
|---|---|---|---|---|
|
| ||||
| Birth weight, mean (SD), g | 1474 (448) | 1477 (448) | 1311 (396) |
|
| Birth weight classification, |
| |||
| ELBW (< 1000 g) | 922 (15) | 897 (15) | 25 (24) | |
| VLBW (1000–1499 g) | 2335 (39) | 2290 (39) | 45 (43) | |
| LBW (1500–2499 g) | 2664 (44) | 2629 (45) | 35 (33) | |
| NBW (≥ 2500 g) | 79 (1) | 79 (1) | 0 | |
| GA, mean (SD), weeks | 31 (4) | 31 (4) | 30 (3) |
|
| GA classification, |
| |||
| Extremely preterm (< 28 weeks) | 989 (16) | 958 (16) | 31 (30) | |
| Very preterm (28 to < 32 weeks) | 3054 (51) | 3007 (51) | 47 (45) | |
| Moderate preterm (32–34 weeks) | 1681 (28) | 1658 (28) | 23 (22) | |
| Late preterm (35–36 weeks) | 193 (3) | 189 (3) | 4 (4) | |
| Term (≥ 37 weeks) | 83 (1) | 83 (1) | 0 | |
| Total length of stay, median (IQR), days | 33 (38) | 33 (38) | 47 (52) |
|
|
| ||||
|
| ||||
| Invasive ventilation, median (IQR), days | 0 (2) | 0 (2) | 1 (5) |
|
| Noninvasive ventilation, median (IQR), days | 0 (3) | 0 (3) | 1 (12) |
|
| Total ventilation, median (IQR), days | 1(6) | 1 (6) | 3 (20) |
|
| Duration of oxygen therapy, median (IQR), days | 5 (36) | 5 (36) | 3.5 (43) | 0.28 |
| Bronchopulmonary dysplasia, | 524 (9) | 508 (9) | 16 (15) |
|
| Antenatal steroids, | 1351 (41) | 1317 (41) | 34 (54) |
|
| Surfactant, | 1350 (35) | 1320 (35) | 30 (43) | 0.15 |
| Chronic lung disease by CXR, | 894 (15) | 865 (15) | 29 (28) |
|
| Apnea of prematurity, | 3205 (53) | 3136 (53) | 69 (66) |
|
|
| ||||
| Patent ductus arteriosus, | 981 (16) | 958 (16) | 23 (22) | 0.12 |
| Congenital heart disease, | 103 (2) | 95 (2) | 8 (8) |
|
|
| ||||
| Intraventricular hemorrhage, | ||||
| No intraventricular hemorrhage | 4737 (79) | 4657 (79) | 80 (76) | 0.48 |
| Grade I–II | 977 (16) | 959 (16) | 18 (17) | 0.81 |
| Grade III–IV | 286 (5) | 279 (5) | 7 (7) | 0.36 |
|
| ||||
| Sepsis, | 1952 (33) | 1910 (33) | 42 (40) | 0.13 |
| Necrotizing enterocolitis, | 415 (7) | 404 (7) | 11 (10) | 0.15 |
| Spirometry | Term ( | Preterm ( |
|
|---|---|---|---|
| FEV1, | 0.35 (1.02) | 0.14 (1.20) | 0.30 |
| FEV1, % Predicted | 104.5 (13.8) | 101.5 (16.0) | 0.27 |
| FVC, | 0.86 (1.18) | 0.73 (1.42) | 0.61 |
| FVC, % Predicted | 112.0 (16.5) | 110.2 (19.7) | 0.58 |
| FEV1/FVC, Z‐score | −0.81 (0.94) | −0.90 (1.05) | 0.63 |
| FEV1/FVC ratio | 79.7 (7.5) | 80.4 (6.82) | 0.53 |
| FEF25‐75, | −0.37 (0.83) | −0.53 (0.84) | 0.27 |
| FEF25‐75, % Predicted | 92.0 (19.5) | 88.5 (19.7) | 0.30 |
|
| |||
| TLC, | 0.48 (1.08) | 0.30 (1.38) | 0.43 |
| TLC, % Predicted | 106.1 (13.2) | 104.4 (16.9) | 0.53 |
| VC, | 0.63 (1.32) | 0.35 (1.61) | 0.31 |
| VC, % Predicted | 107.5 (15.8) | 104.1 (19.1) | 0.28 |
| IC, | 0.52 (1.41) | 0.82 (1.55) | 0.26 |
| IC, % Predicted | 108.9 (24.1) | 114.2 (26.9) | 0.24 |
| FRC, | 0.13 (1.12) | −0.26 (1.31) | 0.08 |
| FRC, % Predicted | 104.6 (23.2) | 97.4 (26.9) | 0.11 |
| ERV, | 0.37 (1.27) | −0.21 (1.49) |
|
| ERV, % Predicted | 116.2 (43.9) | 97.5 (44.9) |
|
| RV, | 0.05 (0.76) | 0.07 (1.34) | 0.92 |
| RV, % Predicted | 103.5 (28.0) | 108.0 (51.8) | 0.58 |
| RV/TLC, | −0.07 (0.82) | 0.07 (1.35) | 0.49 |
| RV/TLC, % Predicted | 98.3 (24.6) | 102.7 (40.4) | 0.48 |
|
| |||
| DLCO, | 0.10 (1.00) | −0.54 (1.12) |
|
| DLCO, % Predicted | 101.9 (14.2) | 94.0 (14.3) |
|
| DLCO Adj, | 0.07 (0.99) | −0.65 (1.13) |
|
| DLCO Adj, % Predicted | 101.5 (13.8) | 92.3 (14.5) |
|
| VA, | 0.24 (1.34) | −0.40 (1.63) |
|
| VA, % Predicted | 103.2 (14.8) | 96.5 (17.1) |
|
| DLCO/VA, | −0.11 (1.10) | −0.31 (1.02) | 0.27 |
| DLCO/VA, % Predicted | 100.1 (15.5) | 98.54 (13.7) | 0.53 |
|
| |||
| MIP, mmHg | 81.3 (20.7) | 71.3 (27.6) |
|
| MEP, mmHg | 88.7 (34.9) | 63.3 (28.2) |
|
| MVV, % Predicted | 90.2 (19.4) | 75.8 (20.5) |
|
|
| |||
| Symptom score (IQR) | 4.4 (0‐10.9) | 8.8 (0‐21.4) |
|
| Activity score (IQR) | 5.9 (0‐12.7) | 18.5 (0‐33.7) |
|
| Impact score (IQR) | 0 (0) | 3.6 (0‐12.5) |
|
| Total score (IQR) | 2.11 (0‐6.1) | 9.3 (3.7‐20.4) |
|
| Pattern | Definition | Termn | Preterm |
| OR | 95% CI |
|---|---|---|---|---|---|---|
| Abnormal volumes | Obstructive or restrictive pattern | 7 (14.6%) | 36 (34.3%) |
| 3.06 | 1.26–7.93 |
| Obstruction | FEV1/FVC < LLN; FVC > LLN | 7 (14.6%) | 25 (23.8%) | 0.28 | 1.79 | 0.75–4.54 |
| ‐ Dysanapsis | FEV1/FVC < LLN; FVC > ULN | 4 (8.3%) | 12 (11.4%) | 0.77 | 1.42 | 0.48–4.20 |
| Restriction | TLC < LLN | 0 (0%) | 12 (11.4%) |
| 13.0 | 0.75–224 |
| Hyperinflation | RV/TLC > ULN | 2 (4.2%) | 12 (11.4%) | 0.23 | 2.97 | 0.69–13.7 |
| Low DLCO | DLCO Adj < LLN | 1 (2.1%) | 17 (16.4%) |
| 9.18 | 1.47–98.3 |
| ‐ Primary vascular abnormality or emphysema | DLCO Adj < LLN, VA Normal/High | 1 (2.1%) | 6 (5.8%) | 0.43 | 2.88 | 0.45–33.7 |
| ‐ Low lung volume, poor expansion | DLCO Adj < LLN, VA < LLN, Kco > ULN | 0 (0%) | 2 (1.9%) | 0.99 | 2.37 | 0.11–50.2 |
| ‐ Loss of capillary and lung volume | DLCO Adj < LLN, VA < LLN, Kco Normal/Low | 0 (0%) | 9 (8.7%) | 0.06 | 9.65 | 0.55–169 |
| Neuromuscular weakness | MVV < 70% pred; and MIP or MEP < 60 mmHg | 2 (4.4%) | 26 (27.7%) |
| 8.22 | 2.01–36.2 |
| Spirometry | Preterm Non‐Hispanic Black ( | Preterm Hispanic ( | Unadjusted | Adjusted |
|---|---|---|---|---|
| FEV1, | −0.97 (0.78) | 0.56 (1.15) |
|
|
| FEV1, % predicted | 86.4 (10.8) | 107.2 (15.1) |
|
|
| FVC, Z‐Score | −0.69 (1.07) | 1.29 (1.20) |
|
|
| FVC, % predicted | 90.5 (15.0) | 117.9 (16.6) |
|
|
| FEV1/FVC, | −0.50 (1.12) | −1.06 (1.01) |
| 0.93 |
| FEV1/FVC ratio | 81.4 (6.7) | 80.1 (7.2) | 0.39 | 0.68 |
| FEF25‐75, | −0.36 (0.86) | −0.60 (0.88) | 0.23 | 0.98 |
| FEF25‐75, % Predicted | 91.0 (23.8) | 87.7 (18.8) | 0.47 | 0.80 |
|
| ||||
| TLC, | −1.24 (0.95) | 0.79 (1.21) |
|
|
| TLC, % Predicted | 86.0 (10.8) | 110.2 (16.1) |
|
|
| VC, | −1.20 (1.20) | 0.96 (1.75) |
|
|
| VC, % Predicted | 85.6 (14.2) | 111.4 (20.4) |
|
|
| IC, | −0.47 (1.10) | 1.30 (1.87) |
|
|
| IC, % Predicted | 91.7 (19.8) | 122.4 (33.0) |
|
|
| FRC, | −1.11 (1.16) | −0.02 (1.19) |
|
|
| FRC, % Predicted | 80.8 (20.3) | 101.7 (24.8) |
|
|
| ERV, | −0.91 (1.28) | 0.13 (1.47) |
| 0.17 |
| ERV, % Predicted | 75.4 (36.2) | 107.9 (44.8) |
| 0.13 |
| RV, | −0.45 (1.03) | 0.13 (1.29) |
|
|
| RV, % Predicted | 88.0 (30.9) | 109.4 (50.8) |
|
|
| RV/TLC, | 0.08 (1.20) | −0.04 (1.31) | 0.68 | 0.05 |
| RV/TLC, % Predicted | 103.0 (33.0) | 98.8 (40.1) | 0.63 | 0.05 |
|
| ||||
| DLCO, | −1.55 (0.91) | −0.06 (0.89) |
|
|
| DLCO, % Predicted | 81.0 (10.2) | 99.8 (12.0) |
|
|
| DLCO Adj, | −1.61 (0.93) | −0.18 (0.95) |
|
|
| DLCO Adj, % Predicted | 80.3 (10.4) | 98.1 (12.9) |
|
|
| VA, | −2.09 (1.50) | 0.30 (1.21) |
|
|
| VA, % Predicted | 78.9 (14.4) | 103.8 (13.2) |
|
|
| DLCO/VA, | 0.21 (1.22) | −0.44 (0.93) |
|
|
| DLCO/VA % Predicted | 104.9 (16.9) | 97.0 (12.1) |
| 0.06 |
|
| ||||
| MIP, mmHg | 71.0 (27.0) | 70.9 (28.3) | 0.99 | 0.28 |
| MEP, mmHg | 57.5 (24.1) | 64.4 (28.8) | 0.33 | 0.30 |
| MVV, % Predicted | 68.8 (20.0) | 78.5 (20.7) |
| 0.08 |
|
| ||||
| Symptom score (IQR) | 14.5 (6.3–34.2) | 6.8 (0–13.9) |
| 0.17 |
| Activity score (IQR) | 30.4 (12.1–59.5) | 12.3 (6.0–30.2) |
| 0.07 |
| Impact score (IQR) | 7.5 (0–22.2) | 1.6 (0–9.0) |
| 0.47 |
| Total score (IQR) | 13.8 (6.7–35.9) | 7.4 (2.5–15.9) |
| 0.16 |
|
Multivariable analysis variable | Beta (95% CI) |
|
|---|---|---|
|
| ||
| Race (Hispanic) | 0.33 (−0.41 to 1.08) | 0.37 |
| Race (Black) | −1.24 (−2.05 to −0.42) |
|
| Birth year | 0.01 (−0.02 to 0.05) | 0.42 |
| Gestational age | 0.01 (−0.08 to 0.10) | 0.82 |
| BPD | −0.64 (−1.26 to −0.02) |
|
| Weight for GA %ile | 0.00 (−0.01 to 0.00) | 0.45 |
|
| ||
| Race (Hispanic) | 0.32 (−0.47 to 1.10) | 0.42 |
| Race (Black) | −1.31 (−2.15 to −0.45) |
|
| Birth year | 0.07 (0.03 to 0.11) |
|
| Gestational age | −0.02 (−0.12 to 0.07) | 0.63 |
| BPD | −0.62 (−1.27 to 0.03) | 0.06 |
| Weight for GA %ile | 0.00 (−0.01 to 0.01) | 0.61 |
|
| ||
| Race (Hispanic) | 0.18 (−0.43 to 0.79) | 0.56 |
| Race (Black) | 0.12 (−0.54 to 0.78) | 0.71 |
| Birth year | −0.03 (−0.06 to −0.01) |
|
| Gestational age | 0.05 (−0.02 to 0.12) | 0.17 |
| BPD | −0.20 (−0.70 to 0.30) | 0.43 |
| Weight for GA %ile | 0.00 (0.00 to 0.01) | 0.74 |
|
| ||
| Race (Hispanic) | 0.08 (−0.62 to 0.78) | 0.82 |
| Race (Black) | 0.11 (−0.65 to 0.87) | 0.77 |
| Birth year | −0.07 (−0.11 to −0.04) |
|
| Gestational age | 0.04 (−0.04 to 0.13) | 0.31 |
| BPD | −0.05 (−0.62 to 0.53) | 0.88 |
| Weight for GA %ile | 0.00 (−0.01 to 0.01) | 0.93 |
|
| ||
| Race (Hispanic) | −0.42 (−1.27 to 0.43) | 0.33 |
| Race (Black) | −2.51 (−3.43 to −1.59) |
|
| Birth year | 0.02 (−0.02 to 0.06) | 0.34 |
| Gestational age | 0.02 (−0.08 to 012) | 0.68 |
| BPD | −0.19 (−0.89 to 0.51) | 0.59 |
| Weight for GA %ile | 0.00 (−0.01 to 0.01) | 0.64 |
|
| ||
| Race (Hispanic) | −0.93 (−1.81 to −0.05) |
|
| Race (Black) | −2.04 (−3.00 to −1.09) |
|
| Birth year | −0.08 (−0.12 to −0.03) |
|
| Gestational age | 0.01 (−0.09 to 0.12) | 0.80 |
| BPD | 0.57 (−0.15 to 1.30) | 0.12 |
| Weight for GA %ile | −0.01 (−0.01 to 0.00) | 0.17 |
|
| ||
| Race (Hispanic) | −0.90 (−0.78 to −0.01) |
|
| Race (Black) | −1.34 (−2.31 to −0.38) |
|
| Birth year | −0.09 (−0.14 to −0.05) |
|
| Gestational age | 0.00 (−0.11 to 0.10) | 0.96 |
| BPD | 0.73 (−0.01 to 1.46) |
|
| Weight for GA %ile | −0.01 (−0.01 to 0.00) | 0.20 |
|
| ||
| Race (Hispanic) | 1.08 (0.46 to 1.70) |
|
| Race (Black) | −0.04 (−0.71 to 0.63) | 0.90 |
| Birth year | 0.06 (0.03 to 0.09) |
|
| Gestational age | 0.09 (0.01 to 0.16) |
|
| BPD | −0.36 (−0.87 to 0.16) | 0.17 |
| Weight for GA %ile | 0.01 (0.00 to 0.01) |
|
- —Research funding provided by Southwestern Health Resources Academic Affiliation Committee.10.13039/100007914
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Congenital Diaphragmatic Hernia Studies · Respiratory Support and Mechanisms
Introduction
1
Preterm birth, defined as birth before 37 weeks gestation, affects roughly 1 in 10 live births in the United States. Critically, fetal lung development is incomplete at earlier gestations, and preterm birth may impair subsequent lung development and growth, increasing risk for life‐long lung disease. Pulmonary complications into early adulthood for individuals with a history of prematurity have been described, such as early onset chronic obstructive pulmonary disease (COPD), reactive airway disease, reduced exercise capacity, and pulmonary hypertension [1, 2, 3]. Abnormal lung growth leading to dysanapsis has also been reported [4]. Extremes of prematurity and neonatal diagnosis of bronchopulmonary dysplasia (BPD) are among several risk factors for long‐term disease [5]. The vast majority of preterm‐born adults studied to date come from primarily Caucasian cohorts, with most born internationally in the 1970s or 1980s [1, 6], and thus may not reflect the current U.S. population. Furthermore, the impact of race, ethnicity, and socioeconomic status remain unclear.
There is a critical unmet need to understand the implications of moderate to extreme preterm birth on long‐term lung function in a multi‐ethnic population born in the modern‐day post‐surfactant era. Here, we utilized a unique U.S.‐born multi‐ethnic preterm cohort born and cared for in the Parkland Hospital Neonatal Intensive Care Unit (NICU), the safety net hospital of Dallas County, Texas, to comprehensively study pulmonary function in adolescents and young adults born ≤ 32 weeks gestation or < 1500 gram birth weight. The primary objective of this study was to evaluate whether adolescents and adults with a history of moderate to extreme prematurity have evidence of reduced lung function, as documented by pulmonary function testing (PFT) including spirometry, lung volumes, diffusion capacity, and respiratory muscle forces. Given the lack of prior assessments in racial minority groups, assessment of whether lung function after preterm birth differed by racial/ethnic status was a secondary objective. The impact of neonatal and socioeconomic risk factors for long‐term reduced lung function were also assessed.
Methods
2
Participants
2.1
The Cardiopulmonary Sequelae in Adolescents and Adults Born Preterm Study was a long‐term follow up study from the Parkland Hospital Neonatal Intensive Care Unit (NICU) Registry [7, 8]. This single‐center cross‐sectional study prospectively enrolled term and preterm adolescents and young adults aged 12–40 from June 2021 to September of 2023. Preterm participants were identified as eligible if born at ≤ 32 weeks gestation or with a birthweight of < 1500 grams at Parkland Hospital. Term participants were eligible if they were born ≥ 37 weeks and had birthweight of > 2500 g, with birth history self‐reported. Term participants were excluded if they had a body mass index (BMI) > 40 kg/m^2^, pre‐existing cardiopulmonary disease, or use of cardiac or pulmonary medications. The complete study included health questionnaires, focused cardiopulmonary exam, echocardiography [8], comprehensive PFT, and overnight oximetry [7]; here we present results related to PFT. The study protocol was reviewed and approved by the UT Southwestern Institutional Review Board (STU 2020‐1332). All participants provided written consent, with assent obtained for adolescent participants.
Pulmonary Function Testing
2.2
Participants completed the St. George Respiratory Questionnaire (SGRQ) to assess for respiratory symptomatology [9]. All participants completed the following comprehensive PFT in accordance with ATS/ERS guidelines [10, 11, 12] [1]: spirometry (FEV1 = forced expiratory volume in 1 s; FVC = forced vital capacity; FEF25‐75 = forced mid‐expiratory flow) [2]; lung volumes (TLC = total lung capacity; VC = vital capacity; IC = inspiratory capacity; FRC = functional residual capacity; ERV = expiratory reserve volume; RV = residual volume) [3]; lung diffusion capacity (DLCO = diffusion capacity for carbon monoxide; DLCO Adj = diffusion capacity for carbon monoxide adjusted for hemoglobin; VA = alveolar volume); and [4] respiratory forces (MIP = maximal inspiratory pressure; MEP = maximal expiratory pressure; MVV = maximal voluntary ventilation). Predicted values were calculated using Global Lung Initiative (GLI) datasets [13]. GLI race neutral predicted and Z‐score values are presented, with the exception of FEF25‐75 values for which GLI race neutral values were unavailable and GLI race‐specific datasets were used. For disease classification, the ERS/ATS technical standard on interpretation was applied using Z‐score defined upper and lower limits to define pathology following interpretation algorithms [12].
Hispanic White and Non‐Hispanic Black were the two primary ethnicity/race combinations in the preterm population, accounting for 91% of enrolled preterm participants, and thus, preterm subgroup analysis was completed. To probe the contribution of socioeconomic factors, birth and adult addresses were geocoded for preterm participants and matched by census tract information to the Childhood Opportunity Index (COI) 2.0 2015 data set [14, 15]. Nationally standardized Z‐scores for subdomains of education, health/environment, social/economic, and total COI scores were computed.
Statistical Analysis
2.3
Statistical analysis was performed using Graphpad Prism version 10. Univariable comparisons of baseline/demographic characteristics, pulmonary function, and respiratory symptoms between term and preterm groups as well as preterm Non‐Hispanic Black and Hispanic groups were conducted using Chi‐square test for categorical variables, and unpaired t‐test (or Wilcoxon rank sum test if necessary) for continuous variables. Odds ratios were computed using Baptist‐Pike method for various pulmonary function profiles. Least squares multivariable regression analyses were conducted to assess for the impact of neonatal and socioeconomic factors between the preterm groups. Multicollinearity was assessed using the Variance Inflation Factor (VIF) with all values being less than < 2.5.
Additional methodologic details are provided in the online supplement.
Results
3
Baseline Characteristics
3.1
A total of 153 subjects were included in this study, of whom 105 were preterm (average gestational age 29.5 ± 2.5 weeks) and 48 were term (average gestational age 39 ± 1.1 weeks). Two preterm participants from the original data set were excluded due to inability to reliably complete any PFT. Baseline characteristics, including demographics, anthropometrics, and summary level neonatal characteristics are listed in Table 1. Preterm participants were slightly younger and more likely to be of Black race or Hispanic ethnicity, were overall shorter, and had significantly higher BMI compared to the term participants. Preterm participants were also more likely to self‐report a history of asthma, had similar tobacco use history, and had reduced strength as determined by lower handgrip muscle forces. Preterm Hispanic patients were younger, born in more recent birth years, and at earlier gestational age compared to Preterm Black participants, consistent with the changing demographics and neonatal survival of the Parkland NICU population [16]. To understand the expected generalizability of the results, the enrolled preterm participants were compared to the eligible preterm participants from the Parkland NICU Registry (Table 2). Enrolled preterm participants were slightly lower gestational age and birth weight than the overall eligible registry population, with higher rates of cardiopulmonary morbidity and longer length of hospital stay, suggesting a slightly sicker enrolled preterm population. Rates of neonatal neurologic and infectious complications were similar.
Pulmonary Function Tests and Respiratory Symptoms
3.2
Comprehensive lung function was compared between term and preterm participants. There were no statistically significant differences in FEV1, FVC, FEV1/FVC ratio, or lung volume %‐predicted or Z‐scores between term and preterm participants (Table 3), with the exception of ERV. However, diffusion capacity percent predicted and Z‐scores were significantly reduced in the preterm group compared with term subjects. Additionally, all measures of muscle forces including MVV, MIP, and MEP were significantly lower in adolescents and adults born preterm. Reductions in MIP, and to a lesser extent MEP, were strongly associated with peripheral muscle strength as measured by handgrip in both term and preterm participants (MIP term R^2^: 0.36, p < 0.0001; preterm R^2^: 0.29, p < 0.0001; Figure E1). Preterm participants also reported significantly greater respiratory symptoms across all domains of the St. George Respiratory Questionnaire (SGRQ). Key pulmonary function parameters are also presented graphically by gestational age in Figure 1.
Key pulmonary function parameters by gestational age categories. Error bars represent mean with standard deviation. FEV1 = forced expiratory volume in 1 s, FVC = forced vital capacity, TLC = total lung capacity, MVV = maximal voluntary ventilation, DLCO Adj = diffusion capacity for carbon monoxide adjusted for hemoglobin. [Color figure can be viewed at wileyonlinelibrary.com]
Despite the appearance of similar spirometry and lung volumes between term and preterm participants, application of the 2022 ERS interpretive strategies for PFT demonstrated multiple abnormal pulmonary function profiles (Table 4). Specifically, 34.3% of preterm‐born adolescents demonstrated an abnormal obstructive or restrictive ventilatory pattern, compared to 14.6% of term‐born controls (p = 0.01, OR 3.06). Rates of obstructive, dysanapsis and hyperinflation patterns were non‐significantly higher in the preterm participants, while restriction was significantly more common in the preterm participants (11.4% of the preterm population). Obstructive profiles were most prevalent in the extremely preterm group (35%), compared to the very preterm (21%) and moderately preterm (13%) groups. Notably, abnormally low DLCO was present in 16.4% of the preterm participants, versus only 2.1% of term (p = 0.01, OR 9.18), with a variety of impaired diffusion profiles. There was not a clear dose–response of prematurity, as 12.9%, 12.8%, and 26% had reduced DLCO (extreme, very, and moderately preterm, respectively). Neuromuscular weakness was also significantly more common in the preterm population, affecting 42% of the extremely preterm group versus 15% and 22% of the very and moderately preterm groups respectively.
Impact of Race and Ethnicity on Lung Function
3.3
Prior long‐term pulmonary follow up studies have included greater than 90% Non‐Hispanic white participants. Thus, we independently evaluated the impact of race/ethnicity on subsequent lung function. Preterm Non‐Hispanic Black and Hispanic White participants were compared with respect to neonatal factors and later lung function. Preterm Hispanic participants were born at a slightly lower gestational age, but in more recent birth years and with higher birth weight percentiles (Table 1). Hispanic preterm participants were also more likely to be treated with continuous positive pressure ventilation, diagnosed with BPD or sepsis, and required longer hospital length of stay (Table E1). Despite suggestion of a sicker Hispanic preterm population, significantly worse spirometric, volumetric, and diffusion capacity parameters were noted in the Non‐Hispanic Black preterm participants (Table 5). These differences persisted after adjusting for baseline differences (birth year, gestational age, weight for gestational age percentile as neonate, ever‐smoker, and BMI) using least squares multivariable regression. However, muscle forces and SGRQ respiratory symptoms were similar between groups after adjustment.
Impact of Neonatal Factors
3.4
Next, we assessed whether neonatal factors were associated with subsequent lung function parameters (Table 6). BPD diagnosis was associated with lower FEV1 and higher RV/TLC, suggesting potential for an obstructive with air trapping phenotype. Low weight for gestational age percentile was associated with lower DLCO, consistent with known associations between intrauterine growth restriction and impaired pulmonary vascularization [17]. More recent birth years were associated with improved FVC but lower FEF25‐75 and FEV1/FVC with higher RV/TLC, suggesting potential for a dysanaptic phenotype. Black race was associated with worse FEV1, FVC, TLC, RV, RV/TLC, and DLCO, but not FEV1/FVC ratio, suggesting potential for a restrictive ventilatory phenotype.
Impact of Socioeconomic Factors
3.5
There is growing recognition of race as a social rather than biologic construct [18], and socioeconomic factors may influence lung development. Given the substantial racial/ethnic differences in our preterm population, and the availability of birth addresses in the NICU database, we evaluated all preterm participants in relation to childhood opportunity index (COI) scores defined by birth or adult geocoded addresses. Birth address COI Z‐scores were below national averages (Z‐score < 0) in both non‐Hispanic Black and Hispanic White preterm participants, consistent with the lower socioeconomic status of our county hospital, but were significantly lower in the preterm Black participants (Table E2). Thus, we assessed whether childhood deprivation was predictive of later pulmonary function independent of race/ethnicity, with multivariable regressions adjusted for birth year, gestational age, weight for gestational age percentile, ever smoker status, and BMI (Table E3). FEF25‐75 was inversely associated with COI variables (e.g. lowest COI score associated with better FEF25‐75), while RV, RV/TLC, and MEP were directly associated with COI score (e.g. lower COI score associated with lower RV/TLC). This suggests slightly better lung function among preterm participants with the most severe reduction in COI scores, and thus differences in lung function cannot be explained by differences in socioeconomic status captured by birth COI. No associations between pulmonary function and COI were identified when adult addresses were used for geocoding, consistent with the hypothesis that childhood exposures influence lung development and growth and thus late outcomes.
Discussion
4
We assessed long‐term pulmonary function in a unique U.S.‐born multi‐ethnic preterm cohort recruited utilizing the Parkland Hospital NICU Registry. Our primary objective was to evaluate whether adolescents and adults with a history of moderate to extreme prematurity have evidence of reduced lung function, as documented by comprehensive PFT including spirometry, lung volumes, diffusion capacity, and respiratory muscle forces. We identified that roughly one in three adults born preterm meet criteria for airflow obstruction or restriction, one in six have an abnormally low diffusion capacity, and one in four have impaired respiratory muscle strength. Further, spirometric, volumetric, and diffusion capacity measures were significantly lower in Black preterm participants as compared to Hispanic White preterm participants. Neonatal risk factors included history of BPD and lower weight for gestational age percentiles. Lung function differences between non‐Hispanic Black and Hispanic preterm participants were not well explained by neonatal differences or available socioeconomic factors evaluated by the birth address COI.
Recognition of Various Profiles After Preterm Birth
4.1
This study represents the first assessment of comprehensive PFT in a multi‐ethnic U.S. born preterm population, and to our knowledge the only assessment to include respiratory muscle force testing in addition to standard pulmonary function testing. Among the limited studies evaluating lung function in adults born moderately to extremely preterm, most were completed in cohorts born in the 1970s and 1980s in an era of neonatal care quite different from our cohort. These studies have reported airflow obstruction as the main lung function impairment after preterm birth which appears to persist across the early lifespan [1, 6, 19, 20, 21, 22, 23, 24]. For example, Vollsaeter et al. had two population‐based cohorts perform lung function testing and demonstrated airway obstruction that persisted from mid‐childhood to adulthood, particularly if there was history of neonatal BPD [23]. Doyle et al. reported lung function trajectories in an extremely preterm Australian cohort at eight, eighteen and 25 years of age, demonstrating that 38% of the preterm cohort had an FEV1/FVC ratio below the 5th percentile, higher than in our study (24%). Part of this witnessed difference may be attributed to our lower rate of extremely premature infants ( ~ 29%) [20] Meta‐analyses of preterm late adolescent and adult lung function also report decreased expiratory airflows indicating airflow obstruction, particularly in those with BPD, and report improvements over more recent birth years [1, 25, 26]. Doyle et al. reported an individual participant level meta‐analysis of spirometry for 935 preterm individuals aged 16–33 (mean 21 years) born with very low birth weight (≤ 1500 g) or very preterm (< 32 weeks) [6]. Mean Z‐scores for FEV1, FVC, and FEV1/FVC ratio were lower in the preterm group, with roughly 23% of preterm‐born adults demonstrating airflow obstruction with FEV1/FVC ratio below the lower limit of normal [6]. While restrictive ventilatory defects have not been highlighted in any of these studies and many did not include lung volume measures, the individual participant level meta‐analysis demonstrated 11% with FVC below the lower limit of normal [6], potentially suggesting restriction and similar to our PFT profile findings here. Several studies have also reported reduced diffusion capacity in adults born preterm, suggestive of reduced gas exchange [27, 28]. This may also suggest pulmonary vascular disease, and we have previously reported increased rates of mild pulmonary hypertension in adults born preterm [3]. Significant limitations of these prior studies include the absence of racial minorities (96.1% non‐Hispanic white in the individual participant meta‐analysis) and inclusion of primarily European and Australian datasets, as well as inclusion of studies primarily from the pre‐surfactant era with birth years before the early 1990s.
An additional novel finding in our study is the presence of significantly lower measures of respiratory muscle strength in the preterm population, which have not previously been described. A prior study demonstrated normal MVV %‐predicted in 70 preterm‐born female adolescents with average gestational age of 35 weeks [29]. However, only females were tested and the average gestational age is significantly older than that included in our study. Importantly, respiratory muscle forces including MIP and MEP correlate strongly with skeletal muscle strength as demonstrated by hand grip [30, 31], and indeed these were strongly correlated in our study as well. Lower handgrip and skeletal muscle strength have been reported in several studies of preterm physiology, and we have previously linked this to mitochondrial dysfunction in animal models of preterm birth [8, 32, 33, 34]. There are important implications to these novel findings. First, whether exercise training can improve measures of respiratory muscle weakness merits further evaluation. Two recent studies demonstrate improvement in peak oxygen consumption with exercise training in adults born preterm, but the direct effect on skeletal muscle strength was not reported [35, 36]. Second, clinicians should consider that individuals born preterm may be more likely to need bilevel rather than continuous positive airway pressure should they develop sleep disordered breathing or hypercarbia.
Impact of Race, Ethnicity and Social Factors
4.2
Very few studies address the impact of race on lung function after preterm birth, yet we identify strikingly lower lung function in Blacks born preterm. A recent study from the BPD Collaborative demonstrated higher rates of death or prolonged hospital stay in preterm infants with BPD born to Black mothers [37]. In the first year of life, two small studies have reported differences in airway resistance in preterm Black infants [38], while a third study reported reduced FEV0.5 and FVC with no difference in the ratio [39], potentially consistent with our report of higher rates of restrictive ventilatory patterns in Blacks born preterm. This particular pattern of restriction has likely been under recognized in the prematurity outcomes literature, possibly due to lack of inclusion of multi‐ethnic populations. However, mechanisms of ventilatory restrictive patterns are unclear. Prior analyses of the general population note that Black populations having lower sitting height, and sitting height accounts for 35%–53% of the racial differences in lung volumes [40, 41]. Whether preterm birth impacts sitting height or thoracic growth specifically is unclear, though its impact on height is well documented.
Prior studies have demonstrated an association between lower FEV1 and FVC values with markers of unfavorable environments and lower socioeconomic status [40, 41, 42, 43, 44]. However, how socioeconomic status intersects with postnatal lung function after preterm birth is unclear. We hypothesized that lower childhood COI, rather than adult COI, would be associated with worse lung function, as childhood exposures may influence lung growth. No associations between adult COI scoring and lung outcomes were noted potentially consistent with this hypothesis. An unexpected relationship between preterm birth COI was identified, with the lowest COI scores having better FEF25‐75, RV, and RV/TLC ratios, possibly indicating subtle improvement in airflow. The exact reasons for this relationship are unclear, and we suspect additional unmeasured factors contribute. We note that our study population represented the lowest quartiles nationally by COI scores, and did not include higher socioeconomic brackets due to the reference population of our county hospital. Further, those in the lowest brackets of socioeconomic status measures may have qualified for socialized aid programs which may have contributed to long term outcome differences. Regardless, racial differences in our preterm populations cannot be explained by environmental and social factors using the COI scoring and further research is needed. At this point, it is unclear how the transition to race‐neutral reference equations will impact diagnostic decisions in the preterm population who may have impaired lung growth over time. Additional attention to this is needed in future studies.
Assessment of Study Design and Methodology
4.3
Since the majority of pulmonary function outcome studies after moderate to extreme preterm birth come from international cohort studies, it is important to assess the generalizability of our study to the U.S. population. We propose that our inclusion of a multi‐ethnic preterm population born during a more modern era of neonatal care is a significant strength. Parkland Hospital is a county non‐referral hospital, and while staffed by academic neonatologists, the NICU does not accept higher level of care transfers, making the included population a reasonable sampling of real‐world data. The higher rates of cardiopulmonary morbidity and lower gestational age in the enrolled participants compared to the overall Parkland NICU database suggests our findings could over‐estimate the disease burden in the Parkland preterm population. However, we note BPD rates in the Parkland population have historically been low compared to national averages, as the Parkland NICU has participated in the Neonatal Research Network for several decades [45, 46]. Thus, it is also possible that our findings of most former preterm participants having normal lung function may over‐estimate health in a national sample with higher BPD rates. The availability of significant neonatal data is a major strength that permitted us to determine which neonatal risk factors were associated with pulmonary function outcomes, as the birth years of our cohort predate routine use of electronic health records which may be mined for more recent cohorts. Another strength is that we have interpreted PFT with respect to ventilatory patterns, rather than relying on single‐value differences between term and preterm individuals. A limitation of the study was poor matching by race/ethnicity in the term and preterm participants. Although we found that preterm Hispanic White individuals exhibited better lung function compared to preterm non‐Hispanic Blacks, we were unable to compare these former preterm populations to a term‐born group consisting of similar ethnic/racial background. However, given the movement away from inclusion of race/ethnicity in normative values, we do not believe this hinders the overall study conclusions.
Conclusion
5
In conclusion, we identified that roughly one in three adults born moderately to extremely preterm meet criteria for airflow obstruction or restriction, one in six have abnormally low diffusion capacity, and one in four have impaired respiratory muscle strength, with overall worse lung function in Black preterm participants as compared to Hispanic White preterm participants. Neonatal risk factors included history of BPD and lower weight for gestational age percentiles. Given that lung function differences between non‐Hispanic Black and Hispanic preterm participants were not well explained by neonatal differences or socioeconomic factors, future studies are needed to assess additional variables that may influence lung growth and subsequent function, including environmental exposures, nutrition and somatic growth.
Subject Category
14.3 Neonatal Lung Disease & BPD.
Author Contributions
Nataly J. Sanchez‐Solano: investigation, writing – original draft, methodology, writing – review and editing, formal analysis. Tyler J. Wall: investigation, writing – original draft, writing – review and editing, methodology, formal analysis. Gregory P. Barton: investigation, writing – original draft, methodology, writing – review and editing, conceptualization, formal analysis, project administration. Dan M. Dane: investigation, methodology, writing – review and editing. Connie C. W. Hsia: conceptualization, investigation, methodology, writing – review and editing. Kara N. Goss: conceptualization, investigation, funding acquisition, writing – original draft, methodology, validation, writing – review and editing, formal analysis, project administration, supervision, data curation.
Ethics Statement
The study protocol was reviewed and approved by the UT Southwestern Institutional Review Board (STU 2020‐1332). All participants provided written consent, with assent obtained for adolescent participants.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Figure E1: Correlation of respiratory muscle forces with handgrip strength. Table E1: Neonatal characteristics by racial/ethnic background among preterm non‐hispanic black and preterm hispanic white participants. Table E2: Childhood opportunity index z‐scores of preterm participants by race/ethnicity. Table E3: Preterm multivariable regression analysis of childhood opportunity index variable associated with pulmonary function measures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. J. Kotecha , J. T. D. Gibbons , C. W. Course , et al., “Geographical Differences and Temporal Improvements in Forced Expiratory Volume in 1 Second of Preterm‐Born Children: A Systematic Review and Meta‐Analysis,” JAMA Pediatrics 176 (2022): 867–877.35759258 10.1001/jamapediatrics.2022.1990 PMC 9237805 · doi ↗ · pubmed ↗
- 2D. S. Bui , J. L. Perret , E. H. Walters , et al., “Association Between Very to Moderate Preterm Births, Lung Function Deficits, and COPD at Age 53 Years: Analysis of a Prospective Cohort Study,” Lancet Respiratory medicine 10 (2022): 478–484.35189074 10.1016/S 2213-2600(21)00508-7 · doi ↗ · pubmed ↗
- 3K. N. Goss , A. G. Beshish , G. P. Barton , et al., “Early Pulmonary Vascular Disease in Young Adults Born Preterm,” American Journal of Respiratory and Critical Care Medicine 198 (2018): 1549–1558.29944842 10.1164/rccm.201710-2016 OCPMC 6298636 · doi ↗ · pubmed ↗
- 4E. A. Mc Ginn , E. W. Mandell , B. J. Smith , J. W. Duke , A. Bush , and S. H. Abman , “Dysanapsis as a Determinant of Lung Function in Development and Disease,” American Journal of Respiratory and Critical Care Medicine 208 (2023): 956–963.37677135 10.1164/rccm.202306-1120 PPPMC 10870865 · doi ↗ · pubmed ↗
- 5B. Thébaud , K. N. Goss , M. Laughon , et al., “Bronchopulmonary Dysplasia,” Nature Reviews Disease Primers 5 (2019): 78.10.1038/s 41572-019-0127-7PMC 698646231727986 · doi ↗ · pubmed ↗
- 6L. W. Doyle , S. Andersson , A. Bush , et al., “Expiratory Airflow in Late Adolescence and Early Adulthood in Individuals Born Very Preterm or With Very Low Birthweight Compared With Controls Born at Term or With Normal Birthweight: A Meta‐Analysis of Individual Participant Data,” Lancet Respiratory medicine 7 (2019): 677–686.31078498 10.1016/S 2213-2600(18)30530-7 · doi ↗ · pubmed ↗
- 7N. J. Sanchez‐Solano , G. P. Barton , T. Martinez‐Fernandez , M. Lee , and K. N. Goss , “Sleep‐Disordered Breathing in a Multi‐Ethnic Cohort of Preterm Adolescents and Adults: Assessment of Neonatal and Subsequent Risk Factors,” Journal of Clinical Sleep Medicine 21 (2024): 519–528.10.5664/jcsm.11440 PMC 1187408239492576 · doi ↗ · pubmed ↗
- 8G. P. Barton , A. Chandra , N. Sanchez‐Solano , J. D. Berry , and K. N. Goss , “Smaller Left Ventricular Size But Preserved Function in Adolescents and Adults Born Preterm,” Journal of the American Heart Association 13 (2024): e 035529.39248261 10.1161/JAHA.124.035529 PMC 11935619 · doi ↗ · pubmed ↗