Virtual reality interventions in the assessment and treatment of alcohol use disorder - a systematic scoping review on methodology
Olivia Gaddum, Stefan Gutwinski, Alva Lütt, Daa Un Moon, Anne Beck, Nadja Ruckser, Alessandro Turno, Robert Schöneck, Felix Bermpohl, Nikolaos Tsamitros

TL;DR
This review examines how virtual reality is used to assess and treat alcohol use disorder, highlighting methodological trends and areas for improvement.
Contribution
The paper provides a systematic scoping review of VR methodologies in AUD research, identifying gaps and suggesting standardization for future studies.
Findings
Most studies used VR cue exposure to induce craving, with consistent positive results in subjective craving induction.
VR scenarios commonly included bars, pubs, and restaurants, with some using aversive environments like hospitals.
There is significant variability in study duration and session numbers, indicating a need for standardized protocols.
Abstract
Virtual reality (VR) technology has been increasingly employed to develop innovative treatments for Alcohol use disorder (AUD) and overcome limitations of currents therapies. However, previous research in this field has yielded inconclusive results. To improve the quality and comparability of studies, a critical analysis of the research methodology employed in this field is necessary. This scoping review aims to provide an overview of existing studies with a focus on their objectives, methodology, treatment paradigms, and VR design characteristics. A systematic literature research was conducted in the electronic databases MEDLINE (PubMed), APA PsychInfo, APA PsychArticles, PSYINDEX (EBSCOhost), Scopus, Web of Science and by search in the reference list of included publication to identify relevant publications. Clinical studies and study protocols using VR for the assessment or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
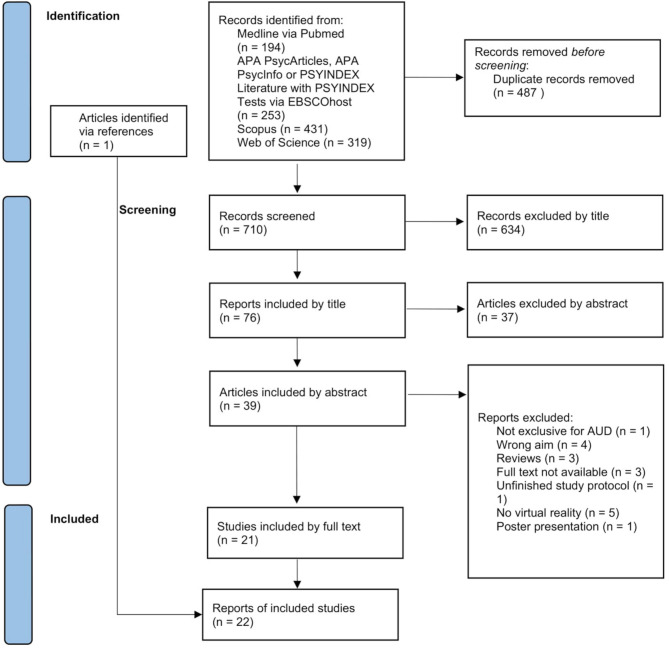 Figure 1
Figure 1- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVirtual Reality Applications and Impacts · Olfactory and Sensory Function Studies · Behavioral Health and Interventions
Introduction
Alcohol use disorder (AUD) is a severe mental health disorder characterized by craving, referring to a strong desire or compulsion to drink alcohol. Currently applied evidence-based treatment approaches for AUD exhibit significant shortcomings with relapse rates after treatment reaching up to 60–85% [1–3]. Given the substantial impact on individual and global health and economics, there is an urgent need for new, promising interventions for AUD to mitigate its negative consequences [1, 4].
VR, a technology that enables realistic simulation of different real-life scenarios, has been rapidly developing since the late 1990s. In recent years, the newer generations of VR applications have been increasingly used for therapeutic interventions in mental health due to their low costs and improved quality [5, 6]. The successful application of virtual reality exposure therapy (VRET) for anxiety disorders has served as a model for adapting and enhancing existing therapies in the field of alcohol and substance use disorders [7]. Clinical guidelines recommend cognitive behavioral therapy (CBT) for AUD [8], while cue exposure therapy (CET), a behavioristic approach based on the effectiveness of exposure therapy for anxiety disorders, has not been well-established, mainly due to difficulties in the practical implication [9]. CET relies on habituation, operant conditioning and cognitive restructuring. Here, visual, auditory, tactile, or olfactory attributes related to the substance, act as conditioned stimuli, eliciting cue-induced craving. The aim of CET is to extinguish craving through repeated non-reinforced exposure, thereby improving clinical outcomes [10, 11]. Although new meta-analytic data support the effectiveness of CET, they also highlight methodological shortcomings in the studies and indicate heterogeneity of results [12]. These mainly result from discrepancies in the applied active interventions and control conditions [12]. Authors also highlight the need for methodological innovations, e.g. Virtual reality-based approaches [12]. Virtual reality cue exposure therapy (VR-CET) provides CET in virtual environments, overcoming several obstacles of conventional CET and enhancing its practicability and effectiveness [13].
A recent development is the combination of cognitive behavioural therapy (CBT) and VR, resulting in a new treatment option for patients with AUD: the VR-assisted CBT (VR-CBT). VR-CBT consists of the implementation of CBT strategies in the context of exposure to high-risk scenarios, aiming to reduce craving through non-reinforced exposure by activating, uncovering, and modifying risk-related beliefs, thought patterns, emotions, and physiological responses [14, 15]. Another proposed therapeutic approach for AUD using VR is the virtual approach-avoidance task training (VAAT-training) [16]. It is argued that realistic VR environments could enhance the effects of the computerized approach-avoidance task training, where participants are instructed to actively push alcoholic beverages away (avoid) and pull non-alcoholic beverages towards them (approach). Reaction times for avoidance and approach can be interpreted as an indicator of craving [16]. An alternative approach to reducing craving is covert sensitization, a conditioning-based aversion therapy in which maladaptive behaviors are repeatedly paired with unpleasant stimuli in the imagination [17]. Choi and Lee adapt this imagery-based technique for use in virtual reality (virtual covert sensitazion, VCS) [18]. Moreover, a new and promising experimental paradigm seems to be emerging from preclinical studies: environmental enrichment (EE). With the aim of increasing the complexity of the simulated environment, EE combines complex social, cognitive, and physical stimulations to reduce craving and relapse risk. While studies in laboratory animals have yielded mixed results [19], Barillot et al. [20] are the first in the attempt of translating EE to humans for the treatment of AUD, evaluating the efficacy of exposure to EE combining physical and cognitive activity with mindfulness in VR to prevent AUD relapse.
Research on clinical VR has faced criticism from experts, who have described it as the “wild west” for being technology-driven, heterogenous and lacking standards and guidelines [21]. The interpretation of existing study results on VR therapy for AUD is limited due to significant methodological shortcomings, such as the use of heterogenous technologies, procedures, and VR stimuli. Furthermore, interventions are frequently inadequately defined, categorised and reported [22, 23]. Langener et al. [22], Ghiţă et al. [23], Segawa et al. [24] and Mazza et al. [25] have already published systematic reviews regarding VR therapy for AUD and other addictive disorders, underlining the need for further research. However, their work focused primarily on efficacy and treatment mechanisms rather than methodology. This review aims to provide an overview of the study landscape, particularly focusing on methodology to facilitate better planning of essential future studies and to improve the overall quality of the study situation.
Following this objective, relevant studies have been identified, analyzed and classified according to their:
- Type and characteristics of study design (e.g. randomized controlled trials, controlled trials).
- Aim and classification of the approaches used (e.g. assessment vs. treatment).
- Clinical setting and VR intervention procedures as number, frequency and duration of sessions and utilization of VR tools, via treatment protocol analysis.
- Characteristics of VR scenarios and presented alcohol cues.
Methods
This review was conducted in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines [26].
A systematic literature research was performed on the 19th of July 2024 using the electronic databases MEDLINE via Pubmed and APA PsycArticles, APA PsycInfo, and PSYINDEX Literature with PSYINDEX Tests via EBSCOhost. A second systematic literature research was carried out on the 19th of April 2025 using the electronic databases Scopus and Web of Science.
The keywords used were standardized MeSH (PubMed) or Thesaurus (EBSCO) search terms with synonyms for each term included automatically. The search terms were: “virtual reality” AND (“alcohol” OR “drink”). Two independent reviewers conducted each search iteration: OG and NT in the first, and OG and NR in the second. First, duplicates were removed. Second, all remaining studies were screened in three iterations: by title, abstract and full text. Third, the references of the selected studies were screened to identify further studies. Any disagreements among the reviewers were addressed in consultation with AB and SG. The following PRISMA flowchart (Fig. 1) visualizes the stages of the data screening process. No review protocol was registered or published, as scoping reviews were not eligible for registration in the available databases at the time of the study.
In- and exclusion criteria
A research protocol was developed a priori to determine in- and exclusion criteria. The technology is only referred to as VR when a head mounted display (HMD) had been used.
The inclusion criteria were as follows:
- A VR intervention has been used to assess or treat AUD.
- Participants meet criteria for alcohol use disorder (AUD) according to the DSM-5, or are otherwise identified as being on the AUD spectrum (e.g., via ICD-10 or validated screening tools such as AUDIT).
- Participants were ≥ 18 years old.
- Clinically relevant outcome measures: either alcohol consumption or symptoms based on the DSM-5 criteria, e.g. craving.
In addition, the following exclusion criteria were defined:
- Other diagnosed SUD (apart from nicotine/tobacco).
- Studies with outcomes associated with non-specific or secondary consequences of alcohol consumption, e.g. cognitive function, were not included in this review as these are not primary endpoints of clinical therapy practices.
- No original data (e.g., reviews, book chapters).
- Languages other than English.
Data extraction
The following data were extracted: title, author, study type, publishing journal, publication year, country of the study, sample size, gender, diagnosis, VR scenarios and alcohol cues, treatment approach, structure of the sessions, the utilized hard- and software, and whether ethical approval was reported, given the clinical nature of the population under study. Additionally, the main results and objectives of each study were extracted and displayed. The data are shown in Tables 1 and 2.
Table 1. Generall information on the studiesYearTitleAuthorsAimLocationStudy type n Journal2024Study on the efficiency of virtual reality in the treatment of alcohol use disorder: study protocol for a randomized controlled trialNègre F et al.TreatmentFranceStudy protocol, prospective RCT156Trials2024Virtual reality-assisted cognitive behavioral therapy for patients with alcohol use disorder: a randomized feasibility studyThaysen-Petersen D et al.Feasibility of TreatmentDenmarkRandomized feasibility study10Frontiers in Psychiatry2024Craving induction through virtual reality cue-exposure for patients with alcohol dependence in rehabilitation treatmentTsamitros N et al.Feasibility of TreatmentGermanyCT21Scientific Reports2023Virtual reality-assisted cognitive behavioural therapy for outpatients with alcohol use disorder (CRAVR): a protocol for a randomised controlled trialThaysen-Petersen D et al.TreatmentDenmarkStudy protocol, prospective RCT102BMJ Open2023Effect of environmental enrichment on relapse rates in patients with severe alcohol use disorder: protocol for a randomised controlled trialBarillot L et al.TreatmentFranceStudy protocol, RCT135BMJ Open2023The efficacy of virtual reality exposure therapy for the treatment of alcohol use disorder among adult males: a randomized controlled trial comparing with acceptance and commitment therapy and treatment as usualDeng H et al.TreatmentChina & Malaysiastudy protocol, prospective RCT120Frontiers in Psychiatry2023Effects of virtual reality-based cue exposure therapy on craving and physiological responses in alcohol-dependent patients-a randomised controlled trialZhang J et al.TreatmentChina & MalaysiaRCT57BMC Psychiatry2023An explorative single-arm clinical study to assess craving in patients with alcohol use disorder using Virtual Reality exposure (CRAVE)-study protocolLütt A et al.AssessmentGermanystudy protocol, explorative single-arm clinical study60BMC Psychiatry2023Immersive virtual plus-maze to examine behavior and psychophysiological-related variables in young people with problematic alcohol and cannabis consumptionMoreno-Fernández RD et al.AssessmentSpainCT50Neurobiology of Stress2020Predictors of changes in alcohol craving levels during a virtual reality cue exposure treatment among patients withaAlcohol use disorderHernández-Serrano O et al.TreatmentSpainsingle-blinded RCT42Journal of Clinical Medicine2020Alcohol craving in heavy and occasional alcohol drinkers after cue exposure in a virtual environment: the role of the sense of presenceSimon J et al.AssessmentBelgiumsingle-blinded CT40Frontiers in Human Neuroscience2020A randomized controlled trial of a virtual reality based, approach-avoidance training updates program for alcohol use disorder: a study protocolMellentin AI et al. TreatmentGermany, Poland & Denmarkstudy protocol, RCT204BMC Psychiatry2020Virtual reality-cue exposure therapy for the treatment of alcohol use disorder: preliminary resultsFigueras-Puigderrajols N et al.TreatmentSpainRCT28Annual Review of Cybertherapie and Telemedicine2019aCraving and anxiety responses as indicators of the efficacy of virtual reality-cue exposure therapy in patients diagnosed with alcohol use disorderGhiţă A et al.TreatmentSpainRCT8Annual Review of Cybertherapie and Telemedicine2019bCue-elicited anxiety and alcohol craving as indicators of the validity of ALCO-VR software: a virtual reality studyGhiţă A et al.AssessmentSpainCT27Journal of Clinical Medicine2017Behavioral, craving, and anxiety responses among light and heavy drinking college students in alcohol-related virtual environmentsGhiţă A et al.AssessmentSpainCT25Annual Review of Cybertherapie and Telemedicine2015The effect of virtual covert sensitization on reducing alcohol craving in heavy social drinkersChoi YJ, Lee JHTreatmentSouth KoreaCT40Virtual Reality2014Can virtual reality be useful to assess subjects with alcohol dependency? Development of a new assessment protocol for patients with alcoholismSpagnoli G et al.AssessmentItalysingle-blinded RCT50European International Journal of Science and Technology2010Virtual reality cues for binge drinking in college studentsRyan JJ et al.AssessmentUSACT23Cyberpsychology, Behavior and Social Networking2009Quantitative electroencephalographic (qEEG) correlates of craving during virtual reality therapy in alcohol-dependent patientsLee SH et al.TreatmentSouth KoreaCT53Pharmacology, Biochemistry and Behavior2008Assessing reactivity to virtual reality alcohol based cuesBordnick PS et al.AssessmentUSACT40Addictive Behaviors2008Social pressure-induced craving in patients with alcohol dependence: application of virtual reality to coping skill trainingLee JS et al.AssessmentSouth KoreaCT28Psychiatry Investigation
Table 2. Information on study protocolsAuthor & YearPatient populationApproachStudy protocolToolsVR-EnvironmentCuesResultsMeasuresDropoutNègre et al. (2024)All diagnosed with AUD;(n = 78) VR-CET + CBT;(n = 78) CBT-onlyVR-CET + CBTPre-treatment assessment; 8 sessions consisting of 4 CBT group sessions (90 min/week) & 4 individual CBT sessions (90 min/week; BT) or 4 supervised individual exposure sessions (VR-CET);duration of exposure varying according to time needed to reduce craving, moving on to next environment when comfortable level of emotion or craving is reached, exposure repeatable if necessary; if craving remains high at the end of a session, time is extended;post-treatment assessment: 6 month follow-up, for a total of 8 months (8 sessions take 2 months to complete)HP reverb G2 HMD, controllers in the form of joysticks, Victus laptop by HP Laptop 16-s0025nf NVIDIA GeForce RTX 4060, C2Care softwareSupermarket, house party, home alone, metroEnvironment, avatars, advertisement, alcoholic beveragesn.a. (study protocol)TLFB (number of drinks consumed at 8 months), TCTQ (craving), VAS (craving), AUDIT-C (frequency of hazardous drinking episodes), EtG (DH toxicology monitoring), GAD-7 (anxiety), PHQ-9 (depression), Sense of Self-Efficacy Questionnaire (self-efficacy), PTQ (rumination), QEP questionnaire (state of presence), Cybermalaise Questionnaire (cybersickness)n.a.Thaysen-Petersen et al. (2024)N = 10 diagnosed with AUD, 1:1 allocated to CBT or VR-CBTVR-CBTPre-treatment assessment; 3 sessions of conventional CBT (1/week, 45–60 min) or VR-assisted CBT (1/week);post-treatment evaluation: 1 month follow-up after 3rd treatment sessionOculus Quest V.2 HMD, 30 different 360° high-risk videos produced using a GoPro CameraRestaurant (6 moments: arrival, ordering food & drinks, drinks served, drinking problem revealed, friend offers shots, friends want to go out)Alcoholic beverages, people, food4/5 experienced craving during VR exposure, 1 no, 2 low, 1 moderate, 1 high craving, overall generally low craving during VR exposure; 3/5 reported transient simulator sickness; median reduction of alcohol consumption greater in VR-CBT at one-week FU (94% vs. 72%) and one-month FU (98% vs. 55%)SSQ (VR-induced simulator sickness), TLFB (alcohol consumption), GAF (subjective assessment of functioning), VAS (craving), PACS (craving), AUDIT (AUD severity), DUDIT (level of drug intake & selected criteria for substance abuse), BDI-II (depression), BAI (anxiety)1 (exclusion before first treatment session due to initiation of disulfiram), resulting in 9 patientsTsamitros et al. (2024)N = 23 diagnosed with ADVR-CETPre-treatment assessment; 1 session: neutral VR environment (waiting room) for familiarization, followed by VR cue exposure environment with alcoholic beverage of participants choice;algorithm of the VR-CET: craving assessment before, 30 s after starting & every 90 s during VR-CET;2 levels: craving < 5/10 during first 3 min (level 1), change in VR environment (level 2): darkening of surrounding space & focusing a light source to the alcoholic beverage; otherwise, participants stayed in level 1 for the entire time; individual duration of VR session between 5 & 14 min;intervention discontinued: very low craving levels (during first 5 min craving of 0 or 1/10) or no more changes in craving levels (after first 3 min, 3 subsequent ratings with the same value when craving ≤ 5/10, or 4 subsequent ratings when craving > 6/10) or 3 decreasing craving levels (2 ratings indicated a reduced value from max. value)Vive Pro Eye HMD, desktop PC (Intel Core i512500, GeForce RTX 3070 Ti graphic card), 2 wireless tracking sensors (HTC VIVE SteamVR Base Station 2.0)Living room, wine bar, pubAlcoholic beverages (beer, red wine, white wine, schnaps, vodka)19/21 increased craving (VAS), 2 consistently low;sig. craving increase from before to maximum during VR & sig. decrease from maximum to 20 min after VR, no sig. difference from before to 20 min after VR; no sig. craving (AUQ) change from pre to after VR, sig. change after removal of 1 outlier; tolerable craving, no acute risk of relapse at end of study;strong sense of presence & negligible symptoms of cybersickness;sig. decrease in pos. affect from pre to post VR; no sig. difference in neg. affectVAS (craving), AUQ (craving), IPQ (presence), SSQ (cybersickness), PANAS (mood), interview (feedback to adjustments of the VR content)2 (exclusion before start because they never consciously experienced craving)Thaysen-Petersen et al. (2023)All diagnosed with AUD,(n = 51) VR-CBT,(n = 51) CBTVR-CBTPre-treatment assessment;14 individual CBT sessions: both study arms (60 min), VR-CBT: 1st session to identify high-risk situations for individualisation of VR exposure (15 min) during sessions 2–14 with CBT strategies, 5 different VR locations with 6 different grades;follow up: 3, 9, & 12 months (after inclusion)Oculus Quest V.2 HMD, 30 different 360° high-risk videos produced using a GoPro CameraPub, bar/party, restaurant, home, supermarketAlcoholic beverages, people, food, cigarettesn.a. (study protocol)TLFB (alcohol consumption), CIWA-Ar (withdrawal), GAF (subj. assessment of functioning), SCIP (psychopathology), VAS (craving), PACS (craving), AUDIT (AUD screening), DUDIT (drug intake, criteria for substance abuse), BDI-II (depression), BAI (anxiety), SSQ (cybersickness), NEQ (neuroconnective endophenotype), interviewsn.a.Barillot et al. (2023)N = 135 diagnosed with AUD, randomised at a 1/1 ratio & exposed to EE or TAUEEPre-treatment assessment;6 EE sessions (during 9 days) consisting of 20 min guided mindfulness while exploring a VE (combining physical activity, cognitive activity & mindfulness in VR);cognitive bike to practice a dual cognitive & physical task; post-treatment evaluation: 2 weeks, 1 & 3 month follow-up after treatment (relapse)Sensory reality pod by Sensiks: multisensory cabin (sounds, smells, airflow, heat) with VR; cognitive bike (Vélo-cognitif) by RevLim; cognitive exercises designed by HappyNeuron,Relaxing natural places (forest, sandy beach), places with cues associated with alcohol consumption (street, party), stressful places (parachute jump, plane)Alcoholic beverages, avatars, cigarettes, coins, cards, smells (forest, beach, alcohol, tobacco, coffee, gasoline)n.a. (study protocol)TLFB (relapse), CDT (relapse), GGT (relapse), OCDS (craving), VAS (craving), IAT (craving, drug-seeking behaviour, attentional bias), FFMQ (mindfulness), HR, RR & salivary cortisol, MPSEQ (richness of daily environment)n.a.Deng et al. (2023)All diagnosed with AUD; (n = 40) VRET, (n = 40) ACT,(n = 40) TAU CGVR-CETPre-treatment assessment;4 weeks of ACT (8 sessions, 60 min/each) or VR-CET (12 sessions, 25 min each/3times per week: 5 min of relaxation, 10 min of exposure to high-risk situation, & 10 min of exposure to aversive situation) +TAU or TAU (8 sessions of non-therapeutic activities, 60 min/each), post-treatment evaluation, follow-up 12 & 24 weeks after start of interventionOculus Quest VR equipmentRelaxation scene (4 landscapes), high-risk scene (street barbecue stands, restaurant, bar, home), aversive situation (visual & auditory stimuli depicting harmful effects of alcohol)Alcoholic beverages, scentsn.a. (study protocol)AUDIT (AUD severity), PACS (craving), HAM-A (severity of anxiety symptoms), HAM-D (severity of depression symptoms), ERP in EEGn.a.Zhang et al. (2023)All diagnosed with AUD; (n = 29) CCT+VR-CE, (n = 28) CCTVR-CETConventional clinical treatment for AD or CCT with the addition of VR cue exposure: 3 sessions per week (1 day apart) for 8 min;post-treatment assessmentOculus quest VR equipment, VR scene shoot with Insta360Pro2 panoramic camera from Insta360 Innovation Technology CoPrivate room in a Chinese restaurant with complex plot designAlcoholic beverages, scents, people, foodSig. lower post-VR-CET changes in VAS & HR before & after cue exposure +VR-CE group than CCT group & before treatment, + VR-CE group no sig. difference in changes in SC & RS than CCT group & before treatmentVAS (caving), HR, SC, RS6 in + VR-CE group dropped (4 automatically during study, 2 missing data), 7 in CCT group dropped (4 automatically during study, 3 missing data)Lütt et al. (2023)N = 60 diagnosed with AUDVR-CETPre-treatment assessment;1 unique session (20 min): alternation of 2 baseline & 2 risk scenarios;post-treatment assessment: short-term follow-up on craving every hour for 3 h afterVIVE Pro EyeUnspecific context (clean, white waiting room), “non-room” (black room with horizon & bright blue grid for spatial orientation) high-risk scenarios (living room, corner pub, wine bar)Alcoholic beverages, peoplen.a. (study protocol)AUQ (craving), OCDS (craving), CAS-A (craving), AUDIT (AUD screening), ADS (AUD severity), LDH (alcohol consumption), VAS (craving & cybersickness), FMSS (cybersickness) IPQ (presence), HR, HRV, EDA, pupillometryMoreno-Fernández et al. (2023)(n = 27) AU,(n = 10) AU + C,(n = 33) CGElevated plus-maze (EPM) using VRPre-treatment assessment;1 session EPM experience with a first (5 min of free exploration) & a second part (3 trials, 2 min to find & touch the boxes)Meta Quest 2Metallic elevated platformn.aAU & AU + C sig. higher craving after VR compared to CG, AU + C sig. higher EDA values during & after VR compared to CG, AU sig. higher ratio of sAA over sCORT (AOCg) compared to CG groupAUDIT (risky consumption: female ≥ 6; male ≥ 8 points), CAST (risky consumption: >4 point for both sexes-), STAI-t, MACS (craving), EDA, HR, salvia samples for sCORT & sAA levelsHernández-Serrano et al. (2020)All diagnosed with AUD & resistant to TAU;(n = 27) TAU;(n = 15) TAU + VR-CETVR-CET8 sessions: 2 assessments (hierarchy of drinks & environments, 20s each), 6 VR-CET sessions (50 min., 2/week) with increasing exposure, patients had to score < 40% of their initial craving 3 times in a row (every 60s) to continueOculus Rift S HMD, sensors, touch controllers, ALCO-VR Software, cotton pads (scents)Pub, bar, restaurant, at homeEnvironments, alcoholic beverages, scentsSig. intragroup changes in craving from pre to post in the VR-CET groupAUDIT (AUD severity), MACS-VR (craving), Stroop (attentional bias), VAS (craving)37 out of 79, 20 in VR-CET & 17 in TAUSimon et al. (2020)18–35 years old,(n = 21) LSDs,(n = 18) heavy drinkersVR-CET1 session for 1 h: 1 min acclimatization, exploring main parts of the environment for 30–60 s each, 2–3 min free exploration, 2 min re-exploration of one partOculus Rift HMD, Software from In VirtuoBar with drinksEnvironment, avatars, scents, alcoholic beveragesCraving sig. higher in heavy than occasional drinkers after immersion;perceived ecological validity sig. predicted craving: moderation effect, with stronger increase in craving with perceived ecological validity in heavy drinkers than occasional drinkers; no mediation effect observedAUDIT (classification of participants), VAS (craving), ITC-SOPI (experience of immersion), UPPS-P (impulsivity), STAI (anxiety)1 out of 40 (cybersickness)Mellentin et al. (2020)Detoxified AUD patients; (n = 68) in each group; AATP on PC & TAU; AATP in VR & TAU; TAUVAAT-training6 VR-sessions (30 min, 3/week) VR- or PC based AATPn.a.Bar with drinksBar, drinks, bartendern.a. (study protocol)MINI (assessment of psychiatric disorders), EUROP-ASI (AUD severity); TLFB (alcohol consumption), VAS (cue-induced craving)n.a.Figueras-Puigderrajols et al. (2020)all diagnosed with AUD & resistant to TAU;(n = 12) VR-CET;(n = 16) TAUVR-CETPre-treatment assessment;6 VR-sessions (1 h) & debriefing afterwards, post-treatment evaluationOculus Rift S HMD, two sensors, a touch controller for each hand; ALCO-VR softwarePub, bar, restaurant, at-homeEnvironments, alcoholic beverages, scentsNo sig. results, but VR-CET group greater decrease in craving levelsAUDIT (AUD severity), STAI (anxiety), MACS (craving), Stroop (attentional bias)n.a.Ghiţă et al. (2019a)all diagnosed with AUD & resistant to TAU; (n = 3) VR-CET & (n = 5) CBTVR-CETPre-treatment assessment;6 VR-sessions (1 h): containing the participants´ preferred alcoholic beverages;post-treatment evaluationOculus Rift HMD, sensors, touch controllers, ALCO-VR softwarePub, bar, restaurant, at-homeEnvironments, alcoholic beverages, scentsSig. reduction in both groups for craving & anxiety responses;VR-CET group showed lower scores of anxiety & craving responses than CBT groupAUDIT (AUD severity), MACS (craving), MACS-VR (craving), STAI (anxiety), VAS (cue-induced craving & anxiety)n.a.Ghiţă et al. (2019b)(n = 13) abstinent AUD patients: (n = 8) male, (n = 5) female; (n = 14) social drinking students: (n = 2) male, (n = 12) femaleVR-CET1 VR-session (10-15 min.), gradually increasing exposure (5 drinks, 4 environments)Oculus Rift HMD, ALCO-VR software, touch controllers scentsNeutral (white room), at-home, bar, restaurant, pubEnvironments, alcoholic beverages, scentsAUD group reported sig. higher scores in self-reported anxiety & alcohol craving levels than the SD group & reported sig. increased craving in all four VR environments in comparison to the neutral VR environmentAUDIT (AUD severity), MACS (craving), MACS-VR (craving), STAI (anxiety), VASn.a.Ghiţă et al. (2017)college students; (n = 5) male, (n = 20) female; (n = 13) LSDs, (n = 12) HSDsVR-CET1 session: participants could choose between alcoholic/non-alcoholic drinks from a menu in each situation, afterwards, they had to observe it for 10 s & rate their craving & anxietyOculus Rift DK2 HMD, joystickAll with alcohol cues: Restaurant, bar, bedroom, chill-out areaEnvironments, commercials, alcoholic beveragesHSDs chose alcoholic drinks sig. more frequently, whereas there wasn´t a sig.difference in self-reported craving or anxiety in the situations.SDU (standard drink units), AUDIT (AUD severity), VAS (craving, anxiety)n.a.Choi & Lee (2015)College students, (n = 20) LDs, (n = 20) HSDsVCS1 session: participants instructed to look at the avatar on the monitor, listen to the sounds & experimenter’s voice, control avatar to follow the routes; evaluation of baseline alcohol craving (AUQ, alcohol-IAT, eye-tracking test & alcohol-Stroop test), virtual hospital followed by subway scenario, narrated by experimenterHMD, 2 controllers, stereo headphonesAversive situations: hospital (health-risk diagnosis, advise to stop drinking), subway (criticism of others for vomitingEnvironments, avatarsHSDs showed sig. greater reduction in craving & sig. weaker positive association with alcohol (IAT scores) after VCS than LDs; sig. effect in dwell time & stroop bias scores in both groupsAUQ (craving), alcohol-IAT (implicit craving), eye-tracking test (implicit craving), alcohol-Stroop test (implicit craving)Spagnoli et al. (2014)All diagnosed with AD,(n = 25) experimental, (n = 25) control;(n = 30) male, (n = 20) femaleVR-CET1 VR-session, participants visited each room chronologically, researcher asked various questions (e.g. regarding emotions, drinking behavior)HMD, Gamepad with joysticks, NeuroVR SoftwarePool, apartment, office (job interview), restaurantEnvironments, alcoholic beverages, food, peopleExperimental group reported more self-efficacy, no sig. differences in motivation for changeSCID (personality disorders), GSE (self-efficacy), MAC-2 A (motivation for change)n.a.Ryan et al. (2010)College students:(n = 15) binge drinkers,(n = 8) non-binge drinkersVR-CET1 VR-session: participants visited each room for 5 min (relaxation, 4 alcohol cue rooms) & gave ratings after each roomHMD, controller, The Scent PaletteUnderwater (neutral), bar, party, kitchen, argumentEnvironment, avatars, scents, alcoholic beveragesSig. higher craving in kitchen & party scenarios in binge group compared to non-binge drinkers11-point Likert-type scale (craving, attention to the sight and smell of alcohol, thoughts about drinking)n.a.Lee et al. (2009)(n = 38) detoxified ADs: (n = 20) VR-CE, (n = 18) TAU;(n = 15) healthy controlsVR-CET & aversive situation10 VR-sessions (2/week), each 30 min; switch to the following stage occurred when craving > 10 min (high risk situation) or dysphoria > 10 min (aversive situation) had been experienced;VAS after each scenarioStereoscopic display, two projectors, joysticks, VR-GogglesRelaxation, individual high risk situation & Aversive situation (vomiting)Environment, alcoholic beverages, scentsEEG alpha power sig. increased among VR-CET group. VR-CET was sig. more effective in decreasing craving than TAU.VAS (craving), EEGn.a.Bordnick et al. (2008)Non-treatment seeking patients;(n = 33) AD, (n = 7) alcohol abuse;(n = 32) male, (n = 8) femaleVR-CET1 VR-session: 5 min. relaxation, each room for 3 min. with rating after every scenario, debriefing afterwardsHMD, The Scent Palette, Wireless game pad, HMD, tracker, VR-ACRAS SoftwareAquarium scenes hotel bar, kitchen, argument situation, partyEnvironments, scents (alcohol, food, smoke), people, alcoholic beveragesCravingsig. higher in scenes with alcohol cues, sig. lower in argument scenes, lowest in neutral environmentAAS (attention to cues), VAS (craving)n.a.Lee et al. (2008(n = 14) abstinent males with AD, (n = 14) healthy controlsVR-CET1 VR-session, 4 VR blocks:1. no cues, no social pressure; 2. no cues, social pressure; 3. cues, no social pressure; 4. cues, social pressure; VAS before & after each blockHMD, tracker, speakersPub (with alcohol cues), street (without cues)Environment, alcoholic beverages, advertisementHigh cravings when generally exposed to alcohol cues in patients with AUD; increased craving due to social pressure in CGVAS (craving)n.a.
Data synthesis
The findings were organized narratively and grouped according to intervention type, following standard practice in scoping reviews. This approach aligns with the PRISMA-ScR guidelines, which recommend mapping key concepts.
Fig. 1. Visualization of study selection using a PRISMA flowchart
Results
General overview
The literature research yielded 1.197 studies. After removing duplicates, 701 articles remained for further screening. Following title, abstract and full-text screening, 21 articles met the inclusion criteria. An additional study [27] was identified via screening of references, bringing the total to 22 studies included in this review. For an overview of the screening process, see Fig. 1, and for a detailed overview of the included studies and their characteristics, see Table 1.
Characteristics of included studies
Four of the 22 studies (18%) [27–30] were completed randomized controlled trials (RCTs), one was a RCT with preliminary results [31] and one was a randomized feasibility study [15], examining a total of 185 participants. Nine studies (41%) [10, 16, 32–38] were controlled trials without randomization, involving a total of 325 participants. Additionally, one study was a feasibility trial for the treatment [39]. Five study protocols of RCTs (23%) [10, 14, 20, 40, 41] and one study protocol for an explorative single-arm clinical study [42] were further included.
Ethical approval was explicitly stated in 17 of the 22 included studies. For the remaining five studies [18, 31, 34, 37, 43], no mention of ethical approval was found, which does not necessarily indicate that approval was not obtained, but rather that it was not reported in the published manuscript.
Across all completed studies, 413 patients (76%) and 138 healthy controls (24%) were examined. Of the participants, 321 (78%) were diagnosed with AUD, alcohol dependence (AD), or alcohol abuse, while 92 (22%) were categorized as “binge drinkers”, “heavy drinkers”, “heavy social drinkers” (HSDs) or with problematic alcohol use based on objective measurements (e.g., AUDIT). Healthy controls were described as “healthy control group”, “light drinkers” (LDs), “light social drinkers” (LSDs), “social drinking students” or “non-bingers”. The study protocols aim to assess 777 patients with AUD, with no healthy controls.
Six studies were conducted in Spain [28, 29, 31, 32, 36, 38], three in South Korea [18, 37, 43] two in the USA [33, 34], and one each in Denmark [15], Belgium [35], Italy [27], Germany [39] China and Malaysia [30]. Two of the study protocols will be conducted in Denmark [14, 44], two in France [20, 40], and one each in Germany [42], China and Malaysia [41].
Aims and approaches
Nine studies [27, 32–36, 38, 42, 43] intended to elicit craving in individuals with AUD in order to test VR as an assessment tool for AUD, whereas twelve studies [14, 15, 20, 28, 30, 31, 37–41, 43] induced craving with the broader scope of investigating the efficacy of VR as a potential treatment for AUD or as a therapy-adjacent tool. One studie applied VCS treatment with the aim of reducing both implicit and explicit craving [18].
Most of the studies examined VR-CET, one study [44] used a stress paradigm in the VAAT-training, one ongoing study used mindfulness and EE in VR [20] and one study evaluated the preliminary efficacy and feasibility of the VR-CBT [15] for an ongoing RCT [14].
Out of 16 studies reporting results, twelve [18, 28–30, 32–37, 39, 43], reported significant changes in craving, while one only reported descriptive scores [15] and three [27, 31, 38] showed non-significant changes. The study using VCS reported significant weaker positive association with alcohol after the treatmannt than the LDs, while dwell time and stroop bias scores showed significant changes in both groups [18]. The four studies reporting physiological and biological correlates of craving showed significant changes in electroencephalography (EEG) alpha power [37], heart rate (HR) [30, 32], salivary alpha-amylase (sAA), salivary cortisol (sCORT) levels [19], while no significant changes were found in respiration [30] and results on electrodermal activity (EDA) were inconsistent [30, 32].
Clinical setting and VR procedures
The study protocols were heterogeneous. The nine studies using VR as an assessment tool as well as the study evaluating the preliminary efficacy and feasibility of a VR-CBT and the study using VCS [18] conducted one VR session, with a duration ranging from seven [32] to 23 min [34].
The studies which aimed to treat AUD conducted an average of seven VR sessions, ranging from two [16] to thirteen [14] with the duration ranging from 8 min [30] to 60 min [31, 36].
While most studies exposed participants to all available VR-CE scenarios, two studies [28, 36] involved increasing exposure levels within each session from the lowest to the highest intensity. In the feasibility assessment study by Tsamitros et al. exposure was applied to the highest-risk scenario until maximum craving was reached [39].In the study by Hernández-Serrano [28], participants had to score less than 40% of their initial craving level in each scenario in order to continue to the next and higher exposure level. In the study by Nègre et al. [40], the duration of the exposure varied according to the time needed to reduce the participants’ craving, as participants moved on to the next environment only when a lower level of craving was reached.
The most frequently used hardware was an Oculus-Rift HMD (Oculus VR, Irvine, CA, USA), reported in six studies [28, 29, 31, 35, 36, 38]. The ALCO-VR software (developed by the VR-Psy Lab, University of Barcelona, Spain) was the most frequently used software, utilized in four studies (carried out by the same research group) [28, 29, 31, 38].
Physiological and biological correlates of craving were measured by Lee et al. [37] via EEG, by Zhang et al. [30] via HR, SC and Respiration and by Moreno-Fernández et al. [32] via EDA, HR, sAA and sCORT levels. Ongoing studies are assessing physiological correlates of craving via HR [20, 42], heart rate variability (HRV) [42], EDA [42], Pupillometry [42], Respiration [20, 42], sCORT [20] and EEG [41]. Besides the physiological correlates of craving, subjective craving measurements were measured in all of the above studies. Subjective craving measurements used were the visual analogue scale (VAS) [14, 15, 20, 28, 30, 32, 34–39, 43, 44], the Alcohol Urge Questionnaire (AUQ) [18, 42] or Mannheimer Craving Scale (MaCS) [31, 32, 36]. Choi and Lee [18] assessed implicite craving as attentional bias toward alcohol cues via eye-tracking (dwell time), Stroop test (response time) and Implicit Association Test.
Furthermore, nine studies [20, 28–31, 36, 37, 41] reported the additional application of alcoholic scents as olfactory cues. The VR sessions according to the study protocol of Barillot et al. [20] will take place in a multisensory cabin that generates sounds, air and heat in addition to olfactory cues.
Virtual reality scenarios
All studies that utilized cue exposure included at least one VR scenario of a bar, pub, party or restaurant, presenting alcoholic beverages, with the exception of Choi and Lee [18], who implemented a virtual covert sensitization paradigm. Their aversive scenarios included a hospital setting, where medical staff advised the user to stop drinking due to health risks, and a subway setting, where the user was criticized by other passengers for vomiting. Nine [14, 20, 27, 28, 33, 34, 36, 41, 42] studies presented at least four different VR scenarios in each session. Other environments included a living room or kitchen at home, parties, a park, a pool, a supermarket and alcoholic advertisements. Six studies [20, 33, 34, 36, 41, 42] additionally included a neutral environment with no alcohol-related cues. The VR intervention in the study of Lee et al. [44] and Deng et al. [41] differed from other included studies by incorporating three successive stages of VR scenarios: relaxation (neutral, landscape), high-risk situation (alcohol cues) followed by an aversive situation (vomiting, harmful effects of alcohol consumption, similar to Choi & Lee [18]. A similar flow was used in the study of Barillot et al. [20], in which relaxing natural places (forest, sandy beach) precede scenarios with cues associated with alcohol consumption (bar, party), which are then followed by immersive stressful contexts (parachute jump, airplane turbulence).
Discussion
This scoping review highlights substantial methodological variability in current studies assessing VR applications for AUD. Most research to date has employed variations of the CE paradigm, with newer approaches such as VR-CBT, VAAT, and EE still under investigation in ongoing trials. While some studies allowed personalization of virtual environments, e.g., selecting preferred drinks or settings, most used similar cue elements, predominantly visual (e.g., alcoholic beverages, bars, bartenders), with a few incorporating olfactory stimuli or aversive scenarios. Hardware and software choices also lacked standardization, though the Oculus Rift headset and ALCO-VR software were used most frequently.
The VR-interventions varied considerably in duration (7–60 min) and number of the sessions (2–13). The VR-CET studies employed various, and occasionally arbitrary, procedures for craving habituation, illustrating the absence of consensus on therapeutic structure. Moreover, only four studies included objective physiological and biological parameters while others were relying instead solely on subjective assessments such as VAS, which are susceptible to expectancy effects and reporting bias. The influence of patients’ expectations on outcomes when using novel technology can also lead to biased results. Most studies lacked randomization, increasing the risk of selection bias, and often failed to report essential methodological details, such as detailed participant characteristics, VR equipment specifications, number of dropouts, or full study protocols. These inconsistencies limit the comparability of findings and hinder the synthesis of robust conclusions regarding intervention efficacy.
Recent study protocols indicate a promising shift toward more rigorous methodologies, including randomized controlled trial designs [14, 20, 40, 41, 44], and the integration of physiological measurements such as heart rate variability and electrodermal activity [20, 41, 42]. Additionally, there is increasing attention to safety and tolerability, with some protocols incorporating standardized assessments of cybersickness, including the FMSS [42], SSQ [14] and the Cybermalaise Questionnaire [41].
This methodological enhancements are crucial as safety concerns, adverse effects like cybersickness, and general tolerability aspects may influence the adherence to potential future applications.
Despite these improvements, most existing studies focused on short-term effects, without measuring relevant long-term outcomes, such as abstinence or relapse rates. Only one randomized feasibility study [15] and four study protocols for prospective RCT [14, 20, 40, 41] included follow up measures in their study protocols, indicating that longitudinal evaluation remains underrepresented. This gap in outcome planning reflects a broader inconsistency in methodological priorities, limiting the ability to systematically assess and improve the impact of VR interventions in AUD treatment.
Strengths and limitations
A systematic literature search in accordance with PRISMA was conducted in various electronic databases and the references were screened to include as many studies as possible. However, only studies in English were considered, and one full text was not available [45]. Additionally, registered studies without the publication of a study protocol were not searched, excluding unpublished research.
Areas for future research
The review underscores the urgent need for the development and adaption of standardized methodological frameworks to evaluate VR applications in AUD research.
Since the induction or reduction of craving within the VR scenario is only a rough indication of clinically relevant measures, future treatment studies using VR-CET should focus on long-term outcome measures, such as abstinence rates or number of relapses. For example, patient follow-up studies after 3, 6 and 12 months could focus on the long-term effect of VR-CET on alcohol consumption. Similarly, assessment studies would benefit from the implementation of objective measurements, such as heart rate variability and electrodermal activity to reduce reporting bias towards a novel intervention, as they have been used previously to improve understanding of alcohol-related cues [46].
There is also a lack of systematic evaluation of feasibility, dose-response relationship, and safety parameters within both VR-CET and assessment studies. Standardized measures of adverse effects should be routinely incorporated and reported to inform tolerability and implementation potential.
Innovative methodological approaches including the use of averse stimuli used by two studies and one study protocol show early promising results in craving. Incorperating aversive stimuli in VR is an advantage to unpleasant aversive stimuli in reallife due to their dehumanizing effects, as well as to CS based upon imagination, reliing on the individual’s capability to imagine [18]. Even though one study yielded promising results using a virtual plus maze as an instrument to explore VAAT within AUD [32], future research could focus more on this approach. Previous findings of the computer-assisted version of this treatment paradigm were encouraging, showing lower relapse rates at two weeks and one-year follow-up, possibly associated with an underlying reduced cue-induced mesolimbic brain activity [10, 16, 47, 48]. The implementation of CBT interventions into VR is another promising development [14]. Since CBT interventions have proven effective in treating patients with AUD [49], this could also be a promising addition to current VR use in the assessment and treatment of AUD. However, these strategies require rigorous testing in standardized formats to determine their replicability and clinical value.
Finally, although many studies used similar technical set-ups (Oculus Rift HMD as hardware and ALCO-VR as software), their VR interventions took place during different stages of VR technological advancement, without taking into account the effect of new relevant characteristics, such as realism, presence, immersion, usability and user satisfaction. These factors may critically shape user engagement and therapeutic outcomes, and their systematic evaluation and reporting should be considered essential components of future research design.
Conclusion
This scoping review highlights the growing interest in applying VR technologies to the assessment and treatment of AUD, particularly through CET. While current research has primarily focused on variations of the CE paradigm, emerging approaches such as VR-CBT, VAAT, and exposure to aversive stimuli are beginning to gain attention through ongoing trials. The heterogeneity in study protocols, session designs, and outcome measures, combined with a reliance on subjective assessments and limited long-term data, poses challenges for comparability and clinical translation. Future VE-CET studies should provide a classification of the exact exposure procedure applied and an explanation of the rationale behind it, e.g. graded, flooded or variable approach. Although the impact of these differences on effectiveness has not been studied, previous studies suggest focusing on scenarios involving cues most likely to induce craving and considering multiple scenarios. Mild subjective craving levels induced can be considered sufficient for treatment purposes. Recent developments, including the integration of physiological measurements, standardized cybersickness assessments, and randomized controlled designs, are promising steps toward more rigorous evaluation. Future research should prioritize long-term outcome measures such as abstinence and relapse rates, explore the integration of evidence-based psychotherapeutic methods like CBT, and assess the impact of evolving VR technologies on user experience and treatment efficacy. Addressing these gaps will be critical for establishing VR as a viable and effective tool in the clinical management of AUD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Riva G, Serino S. Virtual reality in the assessment, Understanding and treatment of mental health disorders. J Clin Med, 2020. 9(11).10.3390/jcm 9113434 PMC 769302133114623 · doi ↗ · pubmed ↗
- 2Tsamitros N et al. [The application of virtual reality in the treatment of mental disorders]. Nervenarzt, 2022.10.1007/s 00115-022-01378-z PMC 985991736053303 · doi ↗ · pubmed ↗
- 3Hernández-Serrano O et al. Determinants of Cue-Elicited alcohol craving and perceived realism in virtual reality environments among patients with alcohol use disorder. J Clin Med, 2021. 10(11).10.3390/jcm 10112241 PMC 819672134064120 · doi ↗ · pubmed ↗
- 4Langener S et al. Clinical relevance of immersive virtual reality in the assessment and treatment of addictive disorders: A systematic review and future perspective. J Clin Med, 2021. 10(16).10.3390/jcm 10163658 PMC 839689034441953 · doi ↗ · pubmed ↗
- 5Hernández-Serrano O et al. Predictors of changes in alcohol craving levels during a virtual reality cue exposure treatment among patients with alcohol use disorder. J Clin Med, 2020. 9(9).10.3390/jcm 9093018 PMC 756566932962176 · doi ↗ · pubmed ↗
- 6Ghiţă A et al. Cue-Elicited anxiety and alcohol craving as indicators of the validity of ALCO-VR software: A virtual reality study. J Clin Med, 2019. 8(8).10.3390/jcm 8081153 PMC 672376431382353 · doi ↗ · pubmed ↗