Ureteroscopy vs Shockwave Lithotripsy to Remove Kidney Stones in Children and Adolescents: A Nonrandomized Clinical Trial
Gregory E. Tasian, David I. Chu, Caleb P. Nelson, W. Robert DeFoor, Justin B. Ziemba, Jing Huang, Xianqun Luan, Michael Kurtz, Christina B. Ching, Pankaj Dangle, Anthony J. Schaeffer, Renea Sturm, Wayland Wu, Christopher Bayne, Nicolas Fernandez, Michael E. Chua, Romano DeMarco

TL;DR
A study compared two kidney stone removal methods in children and found similar success rates but better recovery with shockwave lithotripsy.
Contribution
The study provides real-world evidence on patient-reported outcomes and stone clearance for two common pediatric kidney stone treatments.
Findings
Ureteroscopy and shockwave lithotripsy had similar stone clearance rates (71% vs 68%) in children and adolescents.
Ureteroscopy was linked to more pain, urinary symptoms, and missed school compared to shockwave lithotripsy.
Shockwave lithotripsy showed better patient-reported outcomes despite similar stone clearance.
Abstract
What are the outcomes following ureteroscopy vs shockwave lithotripsy for kidney stone removal in children and adolescents? In this nonrandomized clinical trial including 1142 children and adolescents who underwent kidney stone surgery at 31 North American centers, stone clearance occurred in 71% of patients who underwent ureteroscopy compared with 68% of those who underwent shockwave lithotripsy, but this difference was not statistically significant. Ureteroscopy was associated with greater pain interference, urinary symptoms, and missed school 1 week after surgery. There was no clinically meaningful difference in kidney stone clearance with ureteroscopy vs shockwave lithotripsy, but shockwave lithotripsy was associated with better lived experience. This nonrandomized clinical trial compares kidney stone clearance and patient-reported experiences among children and adolescents…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | All patients (N = 1142) | Treatment group | |
|---|---|---|---|
| Ureteroscopy (n = 953) | Shockwave lithotripsy (n = 189) | ||
| Age, y | |||
| Median (IQR) | 15.6 (12.6-17.3) | 15.6 (12.6-17.2) | 15.6 (12.5-17.6) |
| Group | |||
| 8-11 | 235 (20.6) | 191 (20.0) | 44 (23.3) |
| 12-15 | 397 (34.8) | 341 (35.8) | 56 (29.6) |
| 16-18 | 402 (35.2) | 338 (35.5) | 64 (33.9) |
| 19-21 | 108 (9.5) | 83 (8.7) | 25 (13.2) |
| Sex | |||
| Female | 690 (60.4) | 590 (61.9) | 100 (52.9) |
| Male | 452 (39.6) | 363 (38.1) | 89 (47.1) |
| Race | |||
| Asian | 15 (1.3) | 14 (1.5) | 1 (0.5) |
| Black | 41 (3.6) | 38 (4.0) | 3 (1.6) |
| White | 884 (77.4) | 738 (77.4) | 146 (77.2) |
| Other race | 39 (3.4) | 29 (3.0) | 10 (5.3) |
| Multiple races | 53 (4.6) | 46 (4.8) | 7 (3.7) |
| Missing or unknown | 110 (9.6) | 88 (9.2) | 22 (11.6) |
| Ethnicity | |||
| Hispanic | 130 (11.4) | 110 (11.5) | 20 (10.6) |
| Non-Hispanic | 902 (79.0) | 750 (78.7) | 152 (80.4) |
| Missing or unknown | 110 (9.6) | 93 (9.8) | 17 (9.0) |
| BMI, median (IQR) | 22.2 (18.6-27.4) | 22.2 (18.7-27.7) | 21.6 (17.5-26.5) |
| No. of stones in treated kidney, median (IQR) | 1 (1-2) | 1 (1-2) | 1 (1-2) |
| Cumulative stone size in treated kidney, median (IQR), mm | 7.0 (5.0-11.0) | 7.0 (4.0-11.0) | 8.8 (6.0-11.2) |
| Largest stone size in treated kidney, median (IQR), mm | 6.0 (4.0-9.0) | 6.0 (4.0-9.0) | 7.6 (6.0-9.9) |
| Largest stone size group, mm | |||
| No stone detected | 57 (5.0) | 55 (5.8) | 2 (1.1) |
| <7 | 516 (45.2) | 451 (47.3) | 65 (34.4) |
| 7 to <10 | 334 (29.2) | 246 (25.8) | 88 (46.6) |
| 10 to <15 | 124 (10.9) | 100 (10.5) | 24 (12.7) |
| ≥15 | 51 (4.5) | 46 (4.8) | 5 (2.6) |
| Missing size | 45 (3.9) | 41 (4.3) | 4 (2.1) |
| Missing or unknown | 15 (1.3) | 14 (1.5) | 1 (0.5) |
| Stone location | |||
| No stone | 57 (5.0) | 55 (5.8) | 2 (1.1) |
| Lower pole kidney | 236 (20.7) | 170 (17.8) | 66 (34.9) |
| Non–lower pole kidney | 351 (30.7) | 257 (27.0) | 94 (49.7) |
| Ureter (includes ureteropelvic junction) | 483 (42.3) | 457 (48.0) | 26 (13.8) |
| Missing or unknown | 15 (1.3) | 14 (1.5) | 1 (0.5) |
| History of prior stone surgery | 198 (17.3) | 162 (17.0) | 36 (19.0) |
| Primary indication for stone surgery | |||
| Elective | 164 (14.4) | 97 (10.2) | 67 (35.4) |
| Pain | 706 (61.8) | 635 (66.6) | 71 (37.6) |
| Urinary tract infection | 226 (19.8) | 178 (18.7) | 48 (25.4) |
| Other | 46 (4.0) | 43 (4.5) | 3 (1.6) |
| Presurgical drainage | |||
| None | 836 (73.2) | 658 (69.0) | 178 (94.2) |
| Stent | 280 (24.5) | 271 (28.4) | 9 (4.8) |
| Nephrostomy tube | 10 (0.9) | 10 (1.0) | 0 |
| Other | 5 (0.4) | 3 (0.3) | 2 (1.1) |
| Missing or unknown | 11 (1.0) | 11 (1.2) | 0 |
| Presentation to emergency department before index surgery | 718 (62.9) | 643 (67.5) | 75 (39.7) |
| Structural kidney abnormality in treated side | |||
| Any abnormality | 122 (10.7) | 112 (11.8) | 10 (5.3) |
| Horseshoe kidney | 3 (0.3) | 3 (0.3) | 0 |
| Malrotation | 7 (0.6) | 7 (0.7) | 0 |
| Pelvic kidney | 5 (0.4) | 5 (0.5) | 0 |
| Other | 103 (9.0) | 93 (9.8) | 10 (5.3) |
| Comorbid condition | |||
| Neurogenic bladder | 90 (7.9) | 80 (8.4) | 10 (5.3) |
| Ventilator dependent | 12 (1.1) | 12 (1.3) | 0 |
| Neuromuscular disorder | 149 (13.0) | 118 (12.4) | 31 (16.4) |
| Hematologic disorder | 50 (4.4) | 42 (4.4) | 8 (4.2) |
| Oxygen support | 26 (2.3) | 25 (2.6) | 1 (0.5) |
| Cardiac risk factors | 36 (3.2) | 32 (3.4) | 4 (2.1) |
| Structural central nervous system abnormality | 32 (2.8) | 26 (2.7) | 6 (3.2) |
| Developmental delay | 138 (12.1) | 115 (12.1) | 23 (12.2) |
| Epilepsy | 71 (6.2) | 66 (6.9) | 5 (2.6) |
| Food insecurity | |||
| Often true | 11 (1.0) | 9 (0.9) | 2 (1.1) |
| Sometimes true | 69 (6.0) | 59 (6.2) | 10 (5.3) |
| Never true | 917 (80.3) | 764 (80.2) | 153 (81.0) |
| Missing or unknown | 145 (12.7) | 121 (12.7) | 24 (12.7) |
| Stone clearance | Ureteroscopy, No. (% [95% CI]) | Shockwave lithotripsy, No. (% [95% CI]) | Risk difference (95% CI) |
|---|---|---|---|
| Overall | 474 (71.2 [63.8-78.5]) | 105 (67.5 [61.0-74.1]) | 3.6 (−6.2 to 13.5) |
| Stone size, mm | |||
| <7 | 215 (73.8 [54.8-92.9]) | 32 (79.6 [69.4-89.7]) | −5.7 (−25.9 to 14.4) |
| 7-10 | 137 (68.7 [55.8-81.6]) | 53 (64.1 [50.1-78.2]) | 4.6 (−14.6 to 23.8) |
| >10-15 | 52 (67.3 [44.3-90.2]) | 12 (51.7 [32.2-71.1]) | 15.6 (−12.6 to 43.8) |
| Stone location | |||
| Lower pole kidney | 99 (68.9 [55.4- to 82.5]) | 31 (67.7 [51.4-84.1]) | 1.2 (−18.2 to 20.5) |
| Non–lower pole kidney | 120 (65.8 [53.4-78.3]) | 56 (60.9 [50.6-71.2]) | 4.9 (−12.0 to 21.8) |
| Ureter (includes ureteropelvic junction) | 223 (84.9 [70.1-99.7]) | 15 (93.5 [82.4-104.5]) | −8.6 (−26.3 to 9.2) |
| PRO instrument | Weighted mean score (95% CI) | Procedure effect of ureteroscopy vs shockwave lithotripsy, controlling for baseline, β (95% CI) | |||
|---|---|---|---|---|---|
| Baseline | Postoperative | ||||
| Ureteroscopy (n = 721) | Shockwave lithotripsy (n = 146) | Ureteroscopy (n = 553) | Shockwave lithotripsy (n = 119) | ||
| PROMIS | |||||
| Pain intensity | 45.4 (43.3-47.6) | 41.1 (39.6-42.7) | 49.3 (47.1-51.5) | 42.8 (41.3-44.2) | 3.3 (0.9-5.6) |
| Pain interference | 51.7 (48.9-54.5) | 45.4 (43.5-47.3) | 58.7 (56-61.5) | 48.7 (46.7-50.7) | 5.0 (2.3-7.8) |
| Anxiety | 50.9 (48-53.7) | 47 (45.1-48.8) | 52 (48.6-55.2) | 46.1 (44.3-47.9) | 1.7 (−0.6 to 4) |
| Peer relationships | 48.3 (46.6-50.1) | 48.5 (47-49.9) | 46.8 (44.6-48.9) | 47.8 (45.9-49.6) | −1.3 (−3.5 to 0.9) |
| Sleep disturbances | 56.6 (54.2-59.1) | 52.8 (51.1-54.4) | 56.5 (53.7-59.3) | 52.4 (50.7-54.1) | 1.0 (−0.9 to 3) |
| Stress experiences | 54.6 (52.1-57.1) | 51.2 (49.5-52.9) | 53.5 (51.1-55.8) | 49.3 (47.4-51.2) | 0.6 (−1.6 to 2.8) |
| DVSS value (range, 0-30; urinary symptoms) | 7 (6.2-7.8) | 6.4 (5.7-7) | 7.2 (6.3-8.2) | 5.5 (4.9-6.2) | 0.8 (−0.4 to 1.95) |
| QUIKSS score (range, 0-56; urinary symptoms) | 13.8 (11.5-16.2) | 8.4 (7-9.8) | 19.4 (16.9-22) | 19.4 (16.8-22) | 3.9 (1.2-6.7) |
| Postoperative follow-up | Ureteroscopy, No. (% [95% CI]) | Shockwave lithotripsy, No. (% [95% CI]) | Difference (95% CI) |
|---|---|---|---|
| Participant missed school in the last week | |||
| Week 1 | 407 (85.5 [79.0-92.1]) | 63 (64.3 [54.8-73.8]) | 21.3 (9.7-32.8) |
| Week 3 | 115 (23.3 [12.9-33.7]) | 12 (12.1 [5.7-18.6]) | 11.2 (−1.0 to 23.4) |
| Week 6 | 68 (11.9 [5.3-18.5]) | 15 (14.0 [7.4-20.6]) | −2.1 (−11.4 to 7.2) |
| Caregiver missed work in the last week | |||
| Week 1 | 338 (58.1 [45.8-70.3]) | 44 (37.3 [28.6-46]) | 23.0 (11.0-35.0) |
| Week 3 | 72 (14.0 [5.3-22.7]) | 5 (4.4 [0.6-8.2]) | 13.4 (1.0-25.8) |
| Week 6 | 41 (3.7 [0.9-6.6]) | 7 (6.1 [1.7-10.6]) | −1.3 (−10.9 to 8.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Pediatric Urology and Nephrology Studies · Methemoglobinemia and Tumor Lysis Syndrome
Introduction
Kidney stones affect individuals across their lifespan and often necessitate surgical intervention.^1,2^ Ureteroscopy, an endoscopic surgery, and shockwave lithotripsy, a noninvasive procedure, are the most frequently used procedures to remove kidney and ureteral stones in children and adolescents.^3^ For children, both procedures are typically performed as outpatient surgeries under general anesthesia, but they differ in invasiveness and recovery. Ureteral stents, a driver of pain and urinary symptoms,^4^ may be placed with either modality but are used more commonly following ureteroscopy.^5^ After surgery, residual stone fragments often remain,^6,7^ which may move or grow, resulting in pain and additional surgery.
Clinical guidelines recommend ureteroscopy or shockwave lithotripsy for pediatric patients with ureteral stones and kidney stones smaller than 20 mm.^8,9^ This recommendation is graded C due to consistently low-quality evidence from observational studies and 3 randomized clinical trials. Most studies have demonstrated higher stone clearance for ureteroscopy than shockwave lithotripsy.^10^ None have considered patient experiences after surgery. Despite the uncertainty^10^ and equal weight of the recommendations for ureteroscopy and shockwave lithotripsy, 70% to 80% of youths in the US undergo ureteroscopy to remove kidney stones.^5,11^
The Pediatric Kidney Stone (PKIDS) Care Improvement Network was established to strengthen the evidence base supporting the treatment of children with nephrolithiasis. The PKIDS study arose from patients’ expressed need for improved understanding of the effectiveness of different stone surgeries and the impact of these procedures on their lives. We hypothesized that ureteroscopy would be associated with higher stone clearance^12^ and with lower physical, emotional, and social health compared with shockwave lithotripsy.
Methods
Study Design and Setting
The PKIDS study (NCT04285658) was an investigator-initiated, nonrandomized clinical trial embedded in the clinical care of children and adolescents undergoing kidney stone surgery between March 16, 2020, and July 31, 2023, at 31 medical centers in 22 US states and 1 Canadian province that participate in the PKIDS Network (eFigure 1 in Supplement 1). PKIDS was designated a National Patient-Centered Clinical Research Network (PCORnet) study due to the inclusion of medical centers that contribute data to 5 PCORnet clinical research networks. Institutional review board approval was obtained from the Children’s Hospital of Philadelphia, which served as the data coordinating center. Patients provided informed consent, with caregivers providing consent for children younger than 18 years who assented to participate and for patients who were unable to provide consent or assent. The trial followed the Transparent Reporting of Evaluations With Nonrandomized Designs (TREND) reporting guideline for nonrandomized clinical trials.
Trial Population
We screened English- or Spanish-speaking patients aged 8 to 21 years undergoing ureteroscopy or shockwave lithotripsy for unilateral or bilateral kidney stones, and we enrolled eligible patients. The only exclusion criterion was a clinical situation in which delay to surgery would increase risk (eg, an obstructing stone and fever).
The lower age limit of 8 years was chosen to decrease heterogeneity of patient experiences introduced by using parent-proxy reports for younger children.^13^ We included patients up to age 21 years to align with pediatric care age ranges from the American Academy of Pediatrics.^14^ We ascertained characteristics of participants (preoperatively) and of surgeons and medical centers (before trial opening) that could influence choice of surgery, outcomes, or both.^15^ Participants self-reported race (Asian, Black, White, multiple races, or other race [not further specified]) and ethnicity (Hispanic or non-Hispanic). These data were collected to determine the representativeness of the trial population relative to patients treated with ureteroscopy and shockwave lithotripsy in the US. Three adolescents with nephrolithiasis and 4 parents of children with nephrolithiasis selected patient-reported outcomes (PROs), informed recruitment and retention efforts, and contextualized results.
Outcomes
The primary outcome was stone clearance, defined as the absence of any stone larger than 4 mm in the operated kidney or ureter on ultrasonography 6 (±2) weeks after surgery. We collected all postoperative ultrasonographic images to ascertain stone clearance over longer time periods in sensitivity analyses. Ultrasonography is the preferred imaging for children with kidney stones, given its high sensitivity for kidney stones and lack of ionizing radiation.^16,17^ We chose 4 mm as the cut point because ultrasonography overestimates stone size by approximately 2 mm, a value commonly used to define stone clearance on computed tomography,^18,19,20^ and the risk of future surgery is greater for residual fragments larger than 2 mm.^21^ Ultrasonographic images were obtained in routine care and were interpreted by radiologists at each site (eAppendix 1 in Supplement 1). Results were reported using a standardized template (eAppendix 2 in Supplement 1). A pediatric radiologist (S.B.) blinded to the treatment groups interpreted a random 10% sample of preoperative and postoperative images. A second pediatric radiologist (S.V.) blinded to the treatment groups independently interpreted images with discordant local and central outcomes, with the final determination of stone clearance made by consensus.
The secondary outcomes were PROs at 1 week after surgery. Patient stakeholders selected pain intensity, pain interference (pain that disrupts daily functioning), anxiety, psychological stress, sleep disturbance, peer relationships, and urinary symptoms as the most meaningful postoperative experiences. Questionnaires were administered preoperatively, at the primary PRO end point of 1 week postoperatively, and at 3, 6, and 12 weeks postoperatively. All PROs except urinary symptoms were measured using English and Spanish versions of Patient-Reported Outcomes Measurement Information System (PROMIS) questionnaires administered through REDCap using computer adaptive testing.^22,23^ These questionnaires are validated for children aged 8 to 17 years and are recommended for studies with small numbers of young adults.^24^ We calibrated scores to the PROMIS T scale.^25,26^ Urinary symptoms were measured with the Dysfunctional Voiding Symptoms Score (DVSS),^27^ which is validated in children with bowel and bladder dysfunction, and the Questionnaire for Urinary Issues—Kidney Stone Surgery (QUIKSS) (eAppendix 3 in Supplement 1). The QUIKSS was developed by PKIDS investigators and patient partners for the PKIDS study using PROMIS methodology for item construction^28^ to capture urinary symptoms experienced after stone surgery. Additional outcomes included missed school and work up to 6 weeks postoperatively and emergency department visits, hospitalizations, and surgical reintervention within 3 months of index surgery. Health care encounters were obtained through medical record review and self-report, which were independent sources of outcomes to capture care received at different health systems from where the index surgery occurred.
Comparators
The comparators were ureteroscopy and shockwave lithotripsy. Treatment type was a clinical decision made by the urologist and patient or caregiver (or both) and was performed per the urologist’s discretion. We examined heterogeneity of treatment effect (HTE) for the following prespecified categories: stone clearance by stone size (<7, 7-10, >10-15, or >15 mm) and stone location (ureter or ureteropelvic junction, non–lower pole kidney, or lower pole kidney). Stone size was the linear measurement of the largest stone in the operated kidney or ureter and was classified as a categorical variable to be more interpretable to clinicians. We examined HTE for PROs by sex (female or male) and age (8-11, 12-14, 15-18, or 19-21 years).
Statistical Analysis
The enrollment target of 1290 kidneys or ureters with an expected 4:1 ureteroscopy to shockwave lithotripsy ratio had 80% power with α = .05 to detect a 15% difference^29^ in stone clearance between treatments, a difference that patients and caregivers expressed would change treatment decisions. The study was not powered for HTE analyses. Intention-to-treat analysis was performed based on the index surgery selected. The primary analysis used multiple imputation for the outcome (eTable 1 in Supplement 1).
We used propensity score methods to reduce confounding. The propensities for surgery type were estimated using a multivariable logistic regression model that included patient (eg, stone size and location and kidney anomaly), surgeon (eg, strength of preference for ureteroscopy) (eTable 2 in Supplement 1), and institutional (eg, patient volume) (eTable 3 in Supplement 1) characteristics. The propensity score model was constructed using covariates without incorporating the outcome. The weights remained consistent across all imputed datasets.
All analyses used inverse probability weighting and random intercepts for site. Stone clearance was evaluated per kidney or ureter using logistic regression analysis, and estimated stone clearance rates were generated for each procedure. We used linear regression analysis to evaluate PROs at the participant level at 1 week and other time points after surgery, adjusting for baseline scores. We assessed minimal important change by quantifying the differences in PROMIS T scores between treatments^30^ and the proportion of participants whose urinary symptom scores at 1 week exceeded 50% of the SD of baseline scores.^31^ To explore recovery trajectory, separate models were fit for 3, 6, and 12 weeks after surgery. HTE was analyzed using stratified analyses.
We performed the following sensitivity analyses: (1) complete data, (2) different assumptions for missing data, (3) stone clearance considering ultrasonographic images obtained up to 16 weeks and closest to 6 weeks after surgery, (4) weighting by misclassification of stone clearance based on central imaging review, (5) exclusion of patients older than 18 years, and (6) exclusion of patients with kidney anomalies reported in Table 1. We also compared PROs excluding patients who had a stent placed at time of index surgery.
Assessment of Generalizability
We compared demographics of study participants to patients aged 8 to 21 years who had ureteroscopy or shockwave lithotripsy during the same period at 58 institutions that contribute data to PCORnet. We compared demographics and affected body regions, defined by the Pediatric Medical Complexity algorithm,^32,33^ of patients aged 8 to 21 years who had ureteroscopy or shockwave lithotripsy during the same period at PKIDS sites and non-PKIDS sites in PCORnet.
A 2-sided α = .05 was used for statistical tests. Analyses were performed using R, version 4.4 (R Project for Statistical Computing). Details are provided in the trial protocol and statistical analysis plan in Supplement 2.^34^
Results
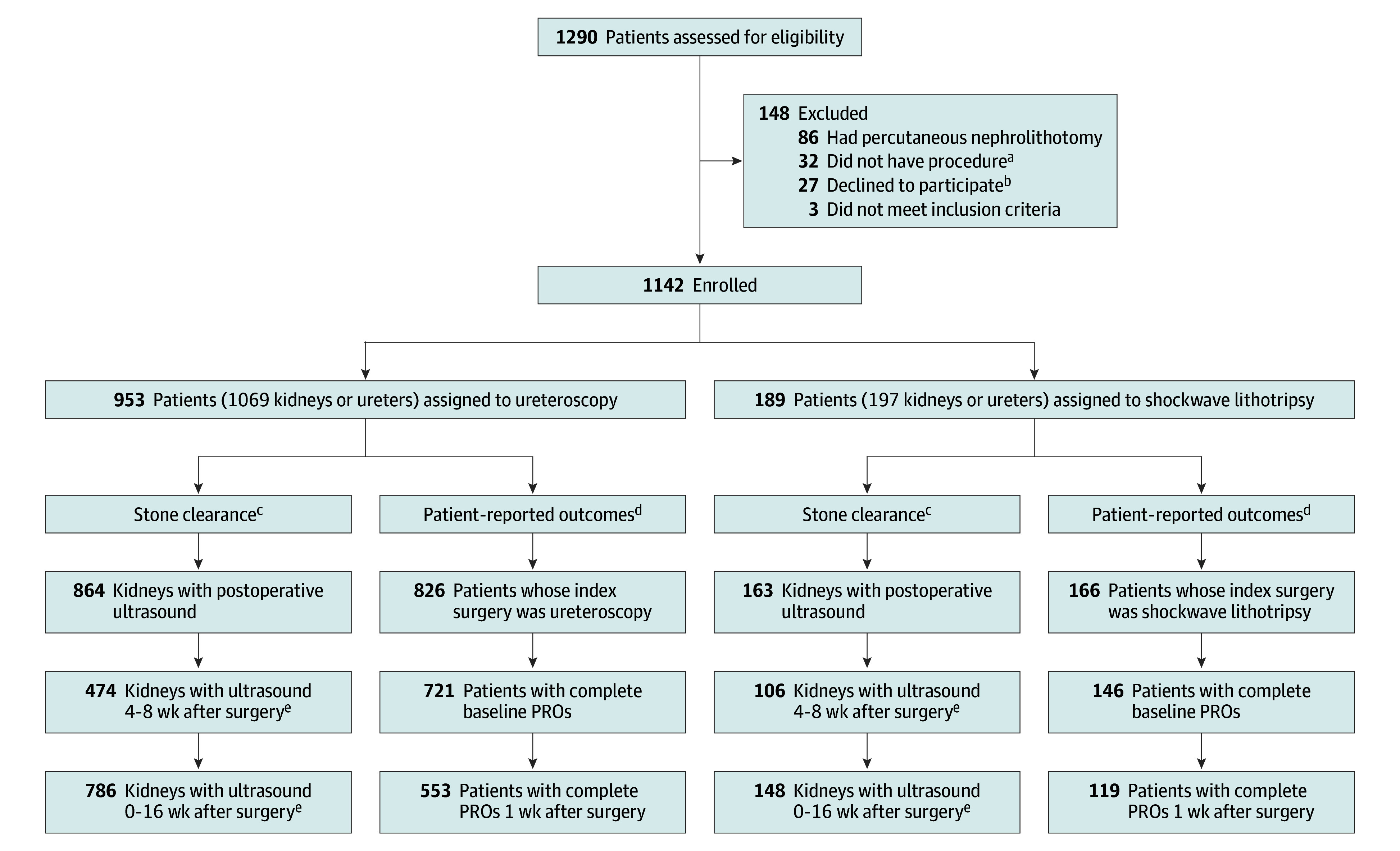
This study included 1142 patients (690 females [60.4%] and 452 males [39.6%]), with a median age of 15.6 years (IQR, 12.6-17.3 years) (Table 1). In terms of race and ethnicity, 15 patients (1.3%) identified as Asian, 41 (3.6%) as Black, 884 (77.4%) as White, 39 (3.4%) as other race, and 53 (4.6%) as multiple races; 130 patients (11.4%) identified as Hispanic and 902 (79.0%) as non-Hispanic. Race and ethnicity were missing or unknown for 110 patients (9.6%). A total of 124 urologists treated 1069 and 197 kidneys or ureters with ureteroscopy and shockwave lithotripsy (n = 953 and 189 patients), respectively (Figure). The median stone size was 6.0 mm (IQR, 4.0-9.0 mm). Of the 1142 patients, 116 (10.2%) received bilateral simultaneous or staged ureteroscopy and 7 (0.6%) received bilateral staged shockwave lithotripsy. A total of 83 of 1069 (7.8%) and 3 of 197 (1.5%) kidneys had ipsilateral repeat ureteroscopy or shockwave lithotripsy after the index surgery, respectively. The top indication for both treatments was pain (Table 1).
Flow Diagram of Patients Who Underwent Ureteroscopy or Shockwave Lithotripsy for Kidney Stone RemovalaParticipants did not receive ureteroscopy or shockwave lithotripsy.bParticipants who withdrew but allowed data collection remained in the analysis cohort.cStone clearance evaluated at the kidney level.dTreatment group allocation and patient-reported outcome (PRO) evaluation are at the patient level.eUltrasonography studies either reported no stone present or had measured stone size.
Surgeon and hospital characteristics are reported in eTables 4 and 5 in Supplement 1. After propensity score weighting, 86 of 88 patient, surgeon, and hospital characteristics had standardized mean differences of less than 0.10 between groups, and all had standardized mean differences of less than 0.25 (eFigure 2 and eTable 4 in Supplement 1).
Of the 109 patients who had a stent placed before ureteroscopy, 78 (71.5%) had stones in the kidney and 31 (28.4%) had stones in the ureter. Ureteral stents were placed at time of index surgery for 841 procedures for 767 of 953 patients (80.4%) receiving ureteroscopy and for 6 procedures for 5 of 189 patients (2.6%) receiving shockwave lithotripsy. The median stent duration was 5 days (IQR, 4-14 days) for ureteroscopy and 21 days (IQR, 10-23 days) for shockwave lithotripsy. For the ureteroscopy group, 527 of 841 participants (62.7%) had a stent on a string removed at home or in the clinic, and 285 of 841 (33.9%) had a stent removed by cystoscopy under general anesthesia. Six participants (100%) receiving shockwave lithotripsy had stents removed under general anesthesia. Overall, 285 of 953 (29.9%) patients who underwent ureteroscopy and 6 of 189 (3.2%) patients who underwent shockwave lithotripsy had secondary procedures under general anesthesia after the index surgery.
In the ureteroscopy and shockwave lithotripsy groups, patients underwent ultrasonography examinations for 474 of 1069 kidneys (44.3%) and 106 of 189 kidneys (56.1%), respectively, 4 to 8 weeks after surgery; in addition, patients had undergone ultrasonography examinations for 786 of 1069 kidneys (73.5%) and 148 of 197 kidneys (75.1%), respectively, by 16 weeks after surgery. The median time after surgery was 6.3 weeks (IQR, 4.7-9.1 weeks). Overall, 547 of 1142 patients (47.9%) and 852 of 1142 patients (74.6%) had undergone ultrasonography 4 to 8 weeks and by 16 weeks after surgery, respectively.
Primary Outcome: Stone Clearance
Stone clearance occurred in 474 patients who underwent ureteroscopy (71.2% [95% CI, 63.8%-78.5%]) and in 105 patients who underwent shockwave lithotripsy (67.5% [95% CI, 61%-74.1%]), a difference that was not statistically significant (risk difference, 3.6% [95% CI, −6.2% to 13.5%]). On central review of 258 participants, stone clearance for 15 patients (5.8%) differed from local interpretations. The sensitivity (97.0%) and specificity (79.0%) of local ultrasonography interpretation were similar between treatments.
We did not consider stones larger than 15 mm in HTE analyses, as only 46 (4.8%) and 5 (2.6%) patients underwent ureteroscopy or shockwave lithotripsy, respectively, for stones larger than 15 mm. There was no difference in clearance for stones 15 mm or smaller or by stone location (Table 2). When the largest stone size was analyzed as a continuous variable, clearance for shockwave lithotripsy decreased for stones larger than 10 mm, while clearance for ureteroscopy remained stable (eFigure 3 in Supplement 1).
Secondary Outcomes
Adjusting for preoperative symptoms, ureteroscopy was associated with higher pain intensity, pain interference, and QUIKSS urinary symptoms at 1 week postoperatively compared with shockwave lithotripsy (Table 3 and eFigure 4 in Supplement 1). There were no statistically significant differences in DVSS values between groups. A total of 238 of 553 patients in the ureteroscopy group (43.0% [95% CI, 36.5%-60.9%]) had QUIKSS urinary symptom scores at 1 week that exceeded 50% of the SD of the baseline scores compared with 33 of 120 in the shockwave lithotripsy group (27.5% [95% CI, 19.5%-35.5%]), a difference of 21.2% (95% CI, 6.6%-35.8%) (eTable 5 in Supplement 1). There were no differences in PROs between treatments after week 1. Patients who received ureteroscopy missed more school (risk difference, 21.3% [95% CI, 9.7%-32.8%]) and caregivers missed more work (risk difference, 23.0% [95% CI, 11.0%-35.0%]) in the week after surgery (Table 4). There were no differences in emergency department visits, hospitalizations, or unanticipated surgery between treatments (eTable 6 in Supplement 1). Ureteroscopy among patients aged 19 to 21 years was associated with worse urinary symptoms at week 1 compared with younger patients undergoing ureteroscopy, an association that did not exist for shockwave lithotripsy (eFigure 5 in Supplement 1). There were no sex differences in PROs between treatments (eFigure 6 in Supplement 1).
Sensitivity Analyses
Results were similar to primary analyses in complete data analyses (eTables 7 and 8 in Supplement 1) when the primary outcome window was extended to 16 weeks after surgery (eTable 9 in Supplement 1), when missing stone clearance outcomes were assumed to be all not cleared or all cleared (eTable 10 in Supplement 1), and when patients aged 19 to 21 years (eTable 11 in Supplement 1) and patients with kidney anomalies (eTable 12 in Supplement 1) were excluded. When models were weighted using misclassification estimates from central ultrasonography review, stone clearance was higher for ureteroscopy than shockwave lithotripsy for stones larger than 10 to 15 mm (risk difference, 35.5% [95% CI, 0.5%-70.5%]) (eTable 13 in Supplement 1). When missing outcomes were replaced with interval values ranging from 25% lower to 25% higher than complete data estimates, results only changed at the extremes or with assumptions of differential clearance (eFigures 7 and 8 and eTables 14 and 15 in Supplement 1). There was no association between ureteroscopy and greater pain and urinary symptoms among patients who did not have stents (eTable 16 in Supplement 1).
Assessment of Generalizability
The sex distribution of participants was similar to PCORnet populations. Study participants were younger, and there was a higher proportion of White patients than in PCORnet populations (eFigures 9-12 in Supplement 1). Except for patients at PKIDS sites who had more musculoskeletal and neurologic conditions, affected body systems of patients treated at PKIDS and non-PKIDS sites in PCORnet were similar (eTable 17 in Supplement 1).
Discussion
This nonrandomized clinical trial embedded in clinical care comparing ureteroscopy and shockwave lithotripsy in children and adolescents generated 4 clinically meaningful findings. First, we did not detect clinically meaningful differences in stone clearance between ureteroscopy and shockwave lithotripsy, despite more patients in the ureteroscopy group having repeat surgery to clear stones. Second, compared with ureteroscopy, shockwave lithotripsy was associated with less pain and lower urinary symptoms during the first week after surgery. Third, patients who received shockwave lithotripsy missed less school and their caregivers missed less work than patients who received ureteroscopy. Fourth, compared with shockwave lithotripsy, 10 times as many patients who underwent ureteroscopy (285 of 953 [29.9%] vs 6 of 189 [3.2%]) required a second procedure under general anesthesia to remove a ureteral stent. This evidence generated from contemporary clinical care calls into question current clinical practice, wherein most children and adolescents with kidney stones receive ureteroscopy.^5^
Stone clearance for ureteroscopy in this study (71.2%) was lower than the 87% reported in a systematic review of primarily retrospective studies of pediatric patients using different imaging modalities.^35^ It is similar to the 68% clearance determined by ultrasonography in a multisite study of adults.^36^ We did not detect statistically significant differences in stone clearance by stone size or location; however, clinically meaningful differences may exist, as this study was not powered to detect HTE. There was some evidence that ureteroscopy was associated with higher clearance of stones larger than 10 mm, which is consistent with reports of lower clearance for stones larger than 10 mm treated with shockwave lithotripsy.^37^ The potential for lower stone clearance with shockwave lithotripsy compared with ureteroscopy should be discussed for patients with stones larger than 10 mm.
Although minimal important change values have not been established for pediatric surgery, differences in pain intensity and pain interference 1 week after ureteroscopy exceeded 3 PROMIS T-score points, a commonly used threshold for minimal important change.^30^ Nearly twice as many patients undergoing ureteroscopy had QUIKSS urinary symptoms scores at 1 week that exceeded 50% of the SD of baseline scores, another definition of minimum important change.^31^ Differences in urinary symptoms were not detected in DVSS values, which were less sensitive after kidney stone surgery compared with scores on the QUIKSS, which has not been validated. The greater pain and urinary symptoms with ureteroscopy were likely driven by ureteral stents,^38^ as the significance of the differences between groups was lost when excluding patients who received a stent, although the power to detect differences was lower due to the smaller sample size. The greater symptoms were particularly pronounced in adolescents who may preferentially benefit from shockwave lithotripsy or from the elimination of stents when feasible if ureteroscopy is selected.
There are several aspects of this study for clinicians to consider when determining how these results should influence their practice. By engaging patients and caregivers in the study design, these results reflect outcomes that are meaningful to patients. The impact of ureteroscopy and shockwave lithotripsy on physical, emotional, and social health and on return to school and work demonstrated in this study was previously unknown. Second, these results reflect the spectrum of children and adolescents with kidney stones treated at medical centers representative of pediatric kidney stone care. These findings can be used to improve selection of shockwave lithotripsy or ureteroscopy and to counsel patients on expected postoperative experiences.
Limitations
This study has limitations. One limitation is the lack of participant randomization. The PKIDS study was designed as a nonrandomized clinical trial because of the lack of clinical equipoise between ureteroscopy and shockwave lithotripsy, which makes randomization difficult, if not impossible. Although we balanced many patient-, surgeon-, and health system–level confounders, the possibilities of unmeasured confounding and bias remain. Second, 547 of 1142 patients (47.9%) underwent ultrasonography within the 4-to-8-week postoperative window, and 852 of 1142 (74.6%) underwent ultrasonography by 16 weeks after surgery. Postoperative imaging was affected by the COVID-19 pandemic, which began when the study opened. Although other studies have shown that stone clearance increases with greater time from index surgery,^39^ sensitivity analyses considering ultrasonographic images obtained by 16 weeks and different missingness assumptions were similar to the primary analysis except for extreme scenarios. Third, ultrasonography has limited ability to differentiate a cluster of small fragments after surgery from a single larger residual stone. Because residual stones 2 mm or larger are more likely to lead to future surgery and stone growth, misclassification of the size of residual fragments would be clinically meaningful.^40^ Fourth, we did not consider the effect of postoperative analgesics on PROs. Finally, we did not consider intraoperative technical aspects that may impact procedural effectiveness.
Conclusions
Among patients aged 8 to 21 years with kidney and ureteral stones in this nonrandomized clinical trial, shockwave lithotripsy resulted in no clinically meaningful differences in stone clearance and better lived experiences during the first week after surgery compared with ureteroscopy. However, shockwave lithotripsy was associated with better PROs. These findings raise questions about the preference for ureteroscopy in practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Routh JC, Graham DA, Nelson CP. Epidemiological trends in pediatric urolithiasis at United States freestanding pediatric hospitals. J Urol. 2010;184(3):1100-1104. doi:10.1016/j.juro.2010.05.018 20650479 · doi ↗ · pubmed ↗
- 2Tasian GE, Ross ME, Song L, . Annual incidence of nephrolithiasis among children and adults in South Carolina from 1997 to 2012. Clin J Am Soc Nephrol. 2016;11(3):488-496. doi:10.2215/CJN.07610715 26769765 PMC 4791823 · doi ↗ · pubmed ↗
- 3Routh JC, Graham DA, Nelson CP. Trends in imaging and surgical management of pediatric urolithiasis at American pediatric hospitals. J Urol. 2010;184(4)(suppl):1816-1822. doi:10.1016/j.juro.2010.03.117 20728146 · doi ↗ · pubmed ↗
- 4Harper JD, Desai AC, Maalouf NM, . Risk factors for increased stent-associated symptoms following ureteroscopy for urinary stones: results from STENTS. J Urol. 2023;209(5):971-980. doi:10.1097/JU.0000000000003183 36648152 PMC 10336697 · doi ↗ · pubmed ↗
- 5Tasian GE, Maltenfort MG, Rove K, . Ureteral stent placement prior to definitive stone treatment is associated with higher postoperative emergency department visits and opioid prescriptions for youth having ureteroscopy or shock wave lithotripsy. J Urol. 2023;209(6):1194-1201. doi:10.1097/JU.0000000000003389 36812398 · doi ↗ · pubmed ↗
- 6Lovegrove CE, Geraghty RM, Yang B, . Natural history of small asymptomatic kidney and residual stones over a long-term follow-up: systematic review over 25 years. BJU Int. 2022;129(4):442-456. doi:10.1111/bju.15522 34157218 · doi ↗ · pubmed ↗
- 7Lombardo R, Tzelves L, Geraghty R, . Follow-up of urolithiasis patients after treatment: an algorithm from the EAU Urolithiasis Panel. World J Urol. 2024;42(1):202. doi:10.1007/s 00345-024-04872-y 38546854 · doi ↗ · pubmed ↗
- 8Assimos D, Krambeck A, Miller NL, . Surgical management of stones: American Urological Association/Endourological Society guideline, part I. J Urol. 2016;196(4):1153-1160. doi:10.1016/j.juro.2016.05.090 27238616 · doi ↗ · pubmed ↗