Novel Mutation Associated With Papillary Thyroid Cancer
Deepashree Gupta, Israa Laklouk, Sang Ngo, Masha Livhits

TL;DR
A new FAT1 gene mutation is found in a case of papillary thyroid cancer, suggesting a potential new genetic link to this type of cancer.
Contribution
This is the first reported case linking FAT1 mutation to papillary thyroid cancer.
Findings
A FAT1p.V912I mutation was identified in a patient with papillary thyroid cancer.
The patient had three foci of papillary thyroid cancer confirmed by histopathology.
FAT1 mutations were previously linked to head and neck cancer but not thyroid cancer.
Abstract
The widespread adoption of molecular testing for cytologically indeterminate thyroid nodules has revealed mutations not previously described in thyroid cancer. The current study reports a novel case of papillary thyroid cancer with a FAT1 mutation. A 47-year-old female presented with a palpable thyroid nodule. Ultrasound revealed a dominant left mid 1.3 cm TI-RADS 4 thyroid nodule. Fine needle aspiration revealed atypia of undetermined significance (Bethesda III); molecular testing with Afirma Genomic Sequencing Classifier was suspicious and identified a FAT1p.V912I c.2734G>A mutation. The patient underwent left thyroid lobectomy. Histopathology revealed papillary thyroid cancer in the index nodule, as well as 2 other foci of papillary thyroid cancer. FAT1 mutation has been previously associated with head and neck squamous cell carcinoma but has not been reported in the context of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
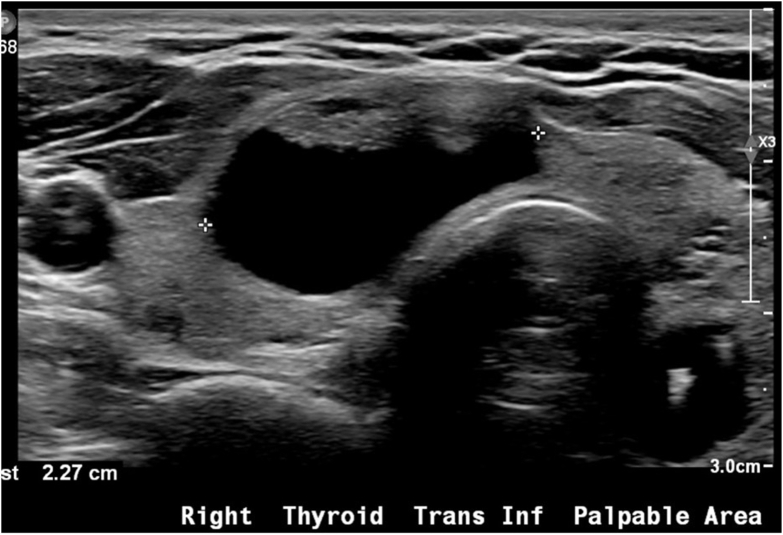 Figure 1
Figure 1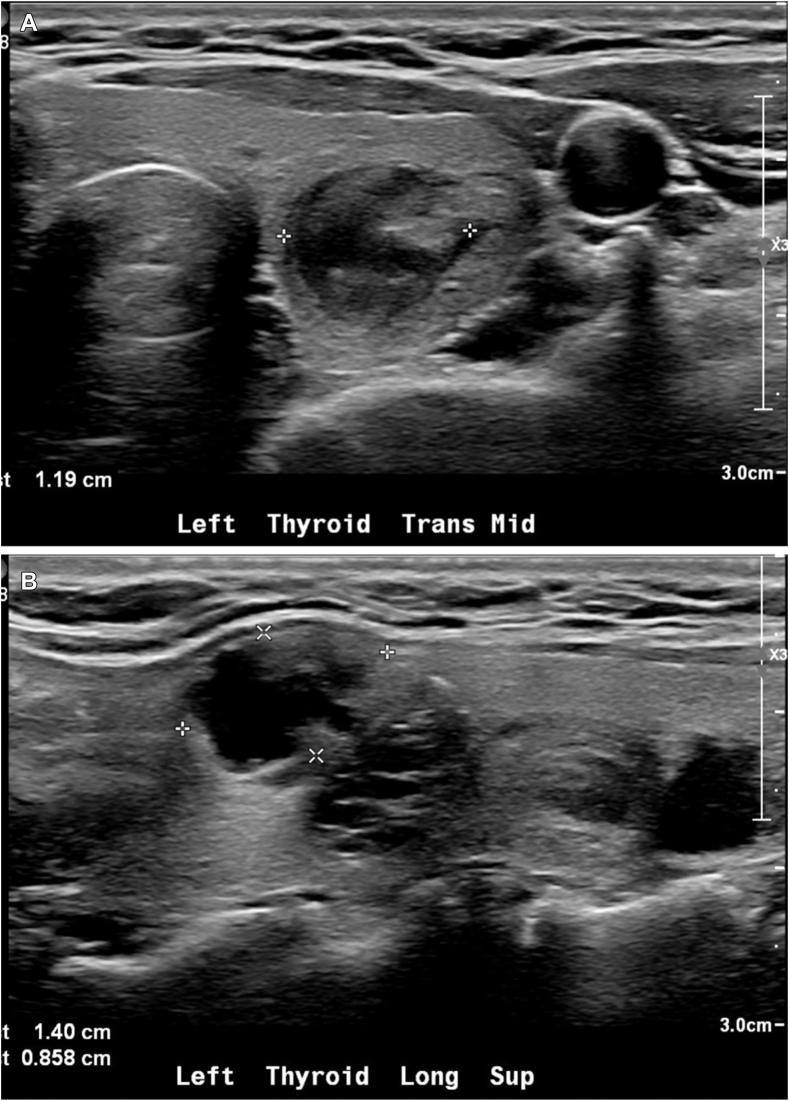 Figure 2
Figure 2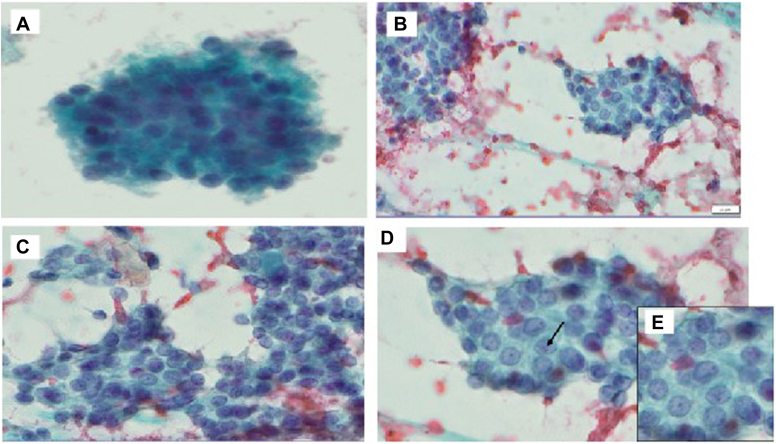 Figure 3
Figure 3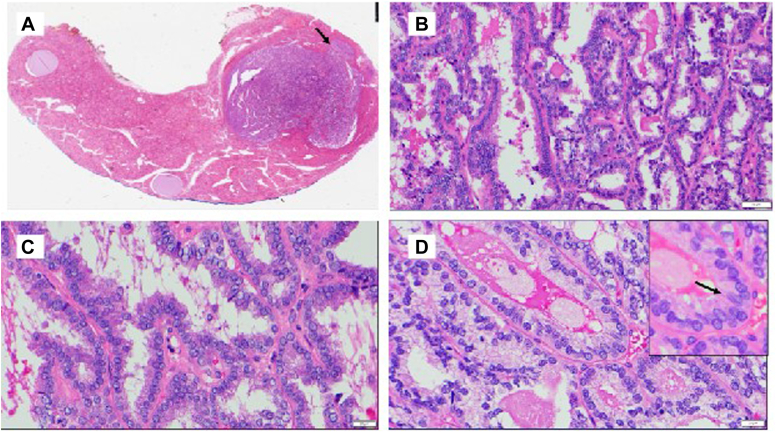 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · BRCA gene mutations in cancer · Genetic factors in colorectal cancer
Highlights
- •PTC is typically driven by BRAF, RAS, RET/PTC point mutations, causing overactivation of the MAPK pathway, accounting for approximately 70% of PTC cases
- •PTC with FAT1 mutation did not demonstrate BRAF V600E mutation or high-grade pathologic features, possibly activating MAPK by an alternative mechanism
- •This case highlights the importance of considering molecular testing in thyroid nodules, as novel mutations may be detected
Clinical RelevanceWe are presenting this case of papillary thyroid cancer with a novel mutation. FAT1 mutation has not been described in the literature pertaining to differentiated thyroid cancer. We have described the clinical presentation, fine needle aspiration, molecular marker, and final pathology findings associated with this mutation.
Introduction
Papillary thyroid cancer (PTC) is the most common form of thyroid cancer, accounting for 70% to 80% of all thyroid cancer cases. PTC is generally indolent with an excellent prognosis. The most common site of spread and recurrence is the cervical lymph nodes. Molecular alterations in the MAP kinase signaling pathway are the most common driver for the development of classic PTC, and mutations in BRAF V600E are found in more than 50% of cases.1 In contrast, follicular variant of PTC is most commonly associated with a mutation in the RAS family. The increasing use of molecular testing for cytologically indeterminate thyroid nodules has provided additional insight into less common mutations that may be associated with thyroid cancer. FAT1 is a tumor suppressor involved in signaling pathways including MAPK/ERK.2 FAT1 mutations have been previously described in human cancers including squamous cell carcinoma,3 but have not been identified in thyroid cancer. This case describes a novel FAT1 mutation in an indeterminate thyroid nodule confirmed to be PTC on histopathology.
Case Report
A 47-year-old female with a history of basal cell carcinoma presented to endocrine clinic with a palpable neck mass. Clinically, the patient denied fatigue, weight changes, heat/cold intolerance, bowel/skin changes, or cardiovascular symptoms. She reported no compressive symptoms. There was no history of exposure to ionizing radiation. She was not known to have a family history of thyroid cancer or endocrine disorders because she was adopted. The patient did not have a history of hypothyroidism or hyperthyroidism and was not on thyroid hormone replacement when she presented for her initial thyroid nodule workup. Her thyroid-stimulating hormone was normal at 0.9 mcIU/mL (0.3-4.7 mcIU/mL).
Ultrasound revealed multiple thyroid nodules, including a 2.3 cm mixed cystic and solid right inferior thyroid nodule (Fig. 1), 1.3 cm solid and hypoechoic left mid thyroid nodule (Fig. 2 A and B), and 1.4 cm mixed cystic and solid left superior thyroid nodule. Fine needle aspiration was performed on the solid left mid thyroid nodule and resulted as atypia of undetermined significance (Bethesda 3) (Fig. 3). Molecular testing with Afirma Gene Sequencing Classifier (GSC) had a suspicious result with a FAT1p.V912I c.2734G>A mutation.4 Other mutations including BRAF V600E, RET/PTC, and RAS mutations were not identified. The risk of malignancy was estimated at 50% due to the suspicious Afirma GSC result.Fig. 1. Thyroid ultrasound image of right thyroid cystic nodule. The nodule measured 2.3 × 1.3 × 2.3 cm and was TI-RADS 2. It had no internal vascularity.Fig. 2. Thyroid ultrasound images of left mid thyroid solid and hypoechoic nodule. The nodule measured 1.3 × 1.2 × 1.2 cm and was TI-RADS 4. It did have internal vascular flow. A, Antero-posterior view; B, Longitudinal view.Fig. 3. Fine needle aspiration (FNA) images. A, FNA shows moderate cellularity composed of clusters of follicular cells forming follicular structure. B and C, follicular cells exhibiting overlapping, mild irregular nuclear contours, and rare grooving. D and E, follicular cells exhibiting overlapping, mild irregular nuclear contours, and rare grooving (arrow).
The patient underwent a left thyroid lobectomy. Histopathology revealed 3 foci of PTC (Table). The index solid nodule with the FAT1 mutation was a 1.4 cm mixed papillary and follicular PTC with no high-grade features such as lymphovascular invasion, tumor necrosis, or increased mitosis (Fig. 4). Immunohistochemistry confirmed a thyroid derived cell lineage with positive PAX8, TTF1, and Thyroglobulin in the index nodule. An additional 1.3 cm follicular variant of PTC was identified in the superior left thyroid lobe, also lacking high-grade features. A third 0.1 cm classic variant of PTC was identified in the superior left thyroid lobe with no high-grade features. Immunohistochemistry was performed for BRAF V600E, and only the classic microcarcinoma was positive. The additional tumors could not be sent for FAT1 testing due to lack of availability of immunohistochemistry. Molecular testing with Afirma GSC can only be performed on indeterminate fine needle aspiration samples, not surgical histopathology.TableHistopathologic Features of 3 Foci of Papillary Thyroid Carcinoma Identified in Left Thyroid LobeVariant of PTCLocationSizeMolecular alterationDescriptionMixed papillary and follicularMid1.4 cmFAT1 mutation (by Afirma GSC)Mixed papillary and follicular architecture, with more than 10% papillary structures present. No high-grade features.FollicularSuperior1.3 cmNoneEncapsulated follicular cell-derived neoplasm. No high-grade features.ClassicSuperior0.1 cmBRAF V600E mutation (identified by IHC)No high-grade features.Abbreviations: GSC = Gene Sequencing Classifier; IHC = immunohistochemistry; PTC = papillary thyroid cancer.Fig. 4. Final pathology images. A, Low power view shows a 1.4 cm nodule composed of a well-differentiated follicular cell-derived neoplasm that is well-demarcated but unencapsulated, with a peripheral edge exhibiting significant irregularity (arrow). (1X) B, The tumor displays mixed papillary and follicular architectures with a complex anastomosing pattern. (200X) C, Short papillary architectures with fibrovascular cores. (400X) D, The follicular cells exhibit nuclear features of papillary thyroid carcinoma (PTC) (crowding, elongation of the nuclei, irregular nuclear contours, and occasional grooving (arrow). (400X).
Discussion
We present a case of a patient with multifocal PTC harboring a somatic FAT1 mutation identified with preoperative molecular testing. The tumor with the FAT1 mutation did not have aggressive histopathology features. The patient underwent surgical thyroid lobectomy and remains under surveillance.
FAT1 encodes a protocadherin and is among the most commonly mutated genes in human cancers.5 It functions as a tumor suppressor by regulating cell proliferation and migration through signaling pathways including MAPK/ERK, Wnt/β-catenin, and Hippo.2 Mutations in FAT1 can disrupt these pathways and promote tumorigenic processes like epithelial-mesenchymal transition that drive tumor progression.2^,^5, 6, 7 Although FAT1 mutations have been previously associated with squamous cell carcinoma and breast cancer,3 their role in PTC has not been characterized.
The pathogenesis of PTC is most commonly driven by point mutations in BRAF, RAS, or RET/PTC chromosomal rearrangements, resulting in overactivation of the MAPK pathway.8^,^9 These mutations account for approximately 70% of PTC cases.10 PTC with a BRAF V600E mutation can be associated with more aggressive tumor features, including tall cell variant.11 Histopathological analysis in this patient revealed a BRAF V600E mutation in the smallest tumor, but it was notably absent from the tumor carrying the FAT1 mutation. None of the tumors in this case exhibited high-grade features.
Given the involvement of FAT1 in the MAPK pathway in other cancers, the presence of a FAT1 mutation in this patient raises the possibility of an alternative route for MAPK activation in PTC. The mechanism by which FAT1 influences MAPK in tumorigenesis remains unclear.2 In medullary thyroid cancer, loss of FAT1 function has been shown to promote cell proliferation, underscoring its role as a tumor suppressor in the thyroid.12 In contrast, overexpression of FAT1 has been shown to suppress oncogenic phenotypes in thyroid cancer cells.13
This case highlights the importance of considering molecular testing in thyroid nodules, as novel mutations like FAT1 may be detected. The detection of rare mutations could have implications for prognostication and the development of targeted drug therapies. Further studies are needed to characterize the significance of FAT1 mutations in PTC, including their pathophysiology and potential role in tumor aggressiveness, metastatic potential, and impact on patient outcomes.
Disclosure
The authors have no conflicts of interest to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yoo S.K.Lee S.Kim S.J.Comprehensive analysis of the transcriptional and mutational landscape of follicular and papillary thyroid cancers Plos Genet 1282016 e 10062392749461110.1371/journal.pgen.1006239 PMC 4975456 · doi ↗ · pubmed ↗
- 2Peng Z.Gong Y.Liang X.Role of FAT 1 in health and disease Oncol Lett 21520213983377722110.3892/ol.2021.12659 PMC 7988705 · doi ↗ · pubmed ↗
- 3Chen Z.G.Saba N.F.Teng Y.The diverse functions of FAT 1 in cancer progression: good, bad, or ugly?J Exp Clin Cancer Res 41120222483596532810.1186/s 13046-022-02461-8PMC 9377080 · doi ↗ · pubmed ↗
- 4Allele description [Variation Report for NM_005245.4(FAT 1):c.2734 G>A (p.Val 912Ile)]https://www.ncbi.nlm.nih.gov/clinvar/RCV 001702145/
- 5Wang Z.Lin K.Xiao H.A pan-cancer analysis of the FAT 1 in human tumors Sci Rep 12120222159810.1038/s 41598-022-26008-1PMC 975114236517565 · doi ↗ · pubmed ↗
- 6Morris L.G.Kaufman A.M.Gong Y.Recurrent somatic mutation of FAT 1 in multiple human cancers leads to aberrant Wnt activation Nat Genet 45320132532612335443810.1038/ng.2538 PMC 3729040 · doi ↗ · pubmed ↗
- 7Hu X.Zhai Y.Kong P.FAT 1 prevents epithelial mesenchymal transition (EMT) via MAPK/ERK signaling pathway in esophageal squamous cell cancer Cancer Lett 397201783932836655710.1016/j.canlet.2017.03.033 · doi ↗ · pubmed ↗
- 8Network C.G.A.R.Integrated genomic characterization of papillary thyroid carcinoma Cell 159320146766902541711410.1016/j.cell.2014.09.050PMC 4243044 · doi ↗ · pubmed ↗