An AI-Based Telerehabilitation Solution to Improve Mobility in People With Multiple Sclerosis (the PLATINUMS Project): Protocol for an Implementation and Evaluation Study
Lars Hvid, Susan Coote, Massimiliano Pau, Alon Kalron

TL;DR
The PLATINUMS project aims to develop and test an AI-based telerehabilitation system to improve mobility for people with multiple sclerosis.
Contribution
The project introduces a novel AI-driven telerehabilitation system designed to be accessible, cost-effective, and suitable for home-based use.
Findings
The system will be evaluated for feasibility, usability, and preliminary efficacy in a multicenter randomized controlled trial.
The project will assess the validity of remote mobility tests using the PLATINUMS platform.
The system aims to address accessibility and standardization barriers in traditional rehabilitation for MS patients.
Abstract
Multiple sclerosis (MS) is a chronic, progressive, and neurodegenerative disease affecting more than 2.8 million people globally. Mobility impairments are among the most significant challenges faced by people with MS, leading to physical inactivity, deconditioning, and disability progression (for some, even irreversible disability). This negatively impacts mental health, social participation, and quality of life while placing a considerable economic burden on society. Exercise can improve mobility and mitigate disability progression, but facility-based options are often inaccessible, especially for those in remote areas. Telerehabilitation offers a promising alternative, but current systems are limited by complexity and hardware requirements. The PLATINUMS (Implementation of an Advanced Telerehabilitation Solution for People With Multiple Sclerosis) project proposes an AI-driven…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
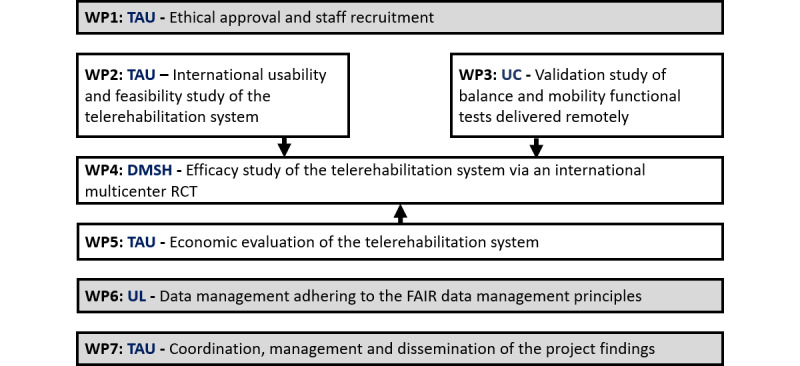 Figure 1
Figure 1 Figure 2
Figure 2|
| Year 1 | Year 2 | Year 3 | ||||||||||||
|
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | |||
|
| ✓ |
|
|
|
|
|
|
|
|
|
|
| |||
|
|
| ✓ | ✓ | ✓ | ✓ |
|
|
|
|
|
|
| |||
|
| T2.1. Installation of the telerehabilitation system, including private data security and cloud data management |
| ✓ |
|
|
|
|
|
|
|
|
|
| ||
|
| T2.2. Harmonization between staff members operating the telerehabilitation system and intervention program |
| ✓ |
|
|
|
|
|
|
|
|
|
| ||
|
| T2.3. Testing the system on a small group of participants for feasibility (patient/therapist), integrity, security, and proper transfer of data |
|
| ✓ | ✓ | ✓ |
|
|
|
|
|
|
| ||
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ |
|
|
|
|
|
| |||
|
| T3.1. Development of mobility assessment tests to be delivered remotely via the telerehabilitation system |
| ✓ | ✓ |
|
|
|
|
|
|
|
|
| ||
|
| T3.2. Establishing reliability and validity of the remote mobility tests |
|
| ✓ | ✓ | ✓ | ✓ |
|
|
|
|
|
| ||
|
| T3.3. Developing standardized instructions and training materials |
|
|
|
|
| ✓ |
|
|
|
|
|
| ||
|
|
|
|
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| |||
|
| T4.1. Coordination between staff members operating the intervention programs and blind assessors on all procedures related with the outcome measures |
|
|
|
|
| ✓ |
|
|
|
|
|
| ||
|
| T4.2. Implementation of intervention programs |
|
|
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ |
|
| ||
|
| T4.4. Data analysis of remote and clinical outcome measures |
|
|
|
|
|
|
|
|
| ✓ | ✓ |
| ||
|
| T4.5. Assessing adherence to and satisfaction with (among participants/therapists) the telerehabilitation intervention program |
|
|
|
|
|
|
|
|
| ✓ | ✓ |
| ||
|
|
|
|
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| |||
|
| T5.1. Identifying the perspective of the economic evaluation and finalizing the specific study questions in terms of economics |
|
|
|
|
| ✓ |
|
|
|
|
|
| ||
|
| T5.2. Identifying all the costs associated with the implementation of the telerehabilitation system and intervention program |
|
|
|
|
| ✓ |
|
|
|
|
|
| ||
|
| T5.3. Following costs of the RCT and identifying all the benefits of the telerehabilitation system and intervention program |
|
|
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ |
|
| ||
|
| T5.4. Cost-effectiveness (cost-utility) analyses |
|
|
|
|
|
|
|
|
|
| ✓ |
| ||
|
| TS.5. Interpretation and reporting of results |
|
|
|
|
|
|
|
|
|
|
| ✓ | ||
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
|
| 17.1. Dissemination of project findings |
|
|
|
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Meetings | Fc | Od | O | O | O | F | O | O | O | O | O | F | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Sclerosis Research Studies · Telemedicine and Telehealth Implementation · Long-Term Effects of COVID-19
Introduction
Multiple sclerosis (MS) is a chronic and progressive disease of the central nervous system that affects more than 2.8 million people worldwide (35.9 per 100,000 people) [1]. One of the most common problems reported by people with MS is impaired mobility, specifically the inability to walk safely and independently [2,3]. Approximately 85% to 90% of people with MS report difficulties with mobility during the disease course [4], and these difficulties can commence very early after onset [5,6]. Due to progression of the disease, most people with MS will eventually require a walking aid (ie, a cane or walker) [7], and in some more severe cases, mobility is possible only by using a wheelchair or scooter [8]. Decreased mobility is, in part, also caused by reductions in physical activity [9], likely mediated through deconditioning of different physiological systems (eg, the cardiorespiratory system) [10]. At some critical points, mobility is limited to such an extent that there is an irreversible disability, resulting in secondary health conditions that are difficult, if not impossible, to treat [11]. This progression of disability also impacts mental health, which further contributes to decreased social, recreational, and vocational participation in society and ultimately results in a poor quality of life [12]. The decrease in participation and work productivity, in combination with an increase in secondary health conditions and medical needs, significantly impacts the global economy worldwide [13,14]. Since MS is the leading cause of disability in young and middle-aged adults, maintaining mobility is essential. Therefore, measures to combat or reverse this downward spiral and progression of disability must be developed and implemented to reduce the burden of this disease.
Exercise can improve mobility and perhaps decrease the rate and extent of disability (ie, impaired physical function) in people with MS [15,16]. Exercise programs based in hospitals and clinical facilities, particularly among other people with MS or under the supervision of MS experts, may help people with MS participate in exercise or exercise at a higher, more intense level [17]. However, a lack of access to these programs, especially for those who live in remote areas where there are few options or where there are health care and medical facilities but no MS experts, may make it difficult to engage in facility-based exercise training programs [18-20]. The COVID-19 pandemic highlighted the need to find alternative solutions to increase exercise and physical activity in the population with MS. In a series of studies involving members of the present consortium, we reported that physical activity and exercise activities, especially at moderate and high intensities, decreased during the pandemic in people with MS [21,22]. Moreover, the research consortium has strongly concluded that to ensure the continuity of exercise training for people with MS during future pandemics, health care stakeholders should be highly encouraged to provide training via advanced remote technologies concurrently with professional guidance and support [23].
Telerehabilitation has excellent potential for providing accessible and cost-effective options for exercise in the home environment for people with MS, particularly if there is ongoing communication with knowledgeable exercise personnel who ensure that exercise is carried out safely and optimally (ie, required movements are performed correctly). However, only a few studies have tested the capability of telerehabilitation to increase exercise and physical activity participation in people with MS, with some encouraging results [24-26]. Nevertheless, despite the advantages associated with the use of telerehabilitation, several limitations still exist that prevent the use of this technology on a large scale. In particular, most commercially available solutions do not provide feedback when the patient does not perform the exercise correctly or require special hardware (eg, movement sensors) that can be hard to set up for nonexpert users [27].
In this project, we intend to implement cutting-edge artificial intelligence (AI) technology designed by WizeCare [28] for a home-based exercise therapy program for people with MS. One of the advantages of this system is its technical simplicity. The system requires only a mobile phone, tablet, or personal computer and has no need for additional third-party hardware. This feature is essential for people with MS with low digital literacy [29]. Moreover, the technology incorporates an AI algorithm that calculates the range of motion and movement speed based on acquired videos of the user performing a specific exercise, enabling real-time feedback and positive encouragement during practice. Lastly, the system includes over 800 exercise drills classified according to targeted body regions and aspects of treatment (ie, flexibility, strength, or coordination) that the therapist can customize to create a personalized exercise program according to each patient’s goals and needs. Notably, the telerehabilitation system has been implemented in numerous health care services with thousands of users (mainly in orthopedic rehabilitation) and has yielded encouraging results in conjunction with positive feedback from patients, physical therapists, and stakeholders. Nonetheless, it has never been systematically tested in the population with MS.
Therefore, our overall goal is to implement an innovative telerehabilitation exercise training system for people with MS by assessing its efficacy in improving mobility. For this primary aim, we propose a pilot multicenter randomized controlled trial (RCT) in established MS centers across the European Union community in Italy, Ireland, and Denmark, as well as in Israel, to establish trial feasibility and to compare exercise delivery via telehealth with usual care. Further innovative aims of the project include (1) assessing the impact of a telerehabilitation exercise training program on mood and quality of life; (2) validating a set of remote mobility clinical tests delivered via the telerehabilitation system to evaluate balance and functional mobility in people with MS; and (3) examining the cost-effectiveness and value of the telerehabilitation exercise intervention program for people with MS. This information is scarce in the treatment of people with MS.
Ultimately, the knowledge obtained from this research will be relevant not only for people with MS; it is expected to also be of great value in understanding the most helpful way to deliver the benefits of home-based exercise therapy to other vulnerable populations, including many older adults who may appear healthy but are not, and others with neurological impairments (eg, stroke or Parkinson disease).
Methods
Overview
Our main objective is to collect evidence to facilitate the implementation of an innovative AI telerehabilitation exercise training system in MS clinical practice. After the completion of working package (WP) 1, which focuses on obtaining ethical approval and recruiting staff, our first objective (WP2) will be to investigate the usability and feasibility of the WizeCare system in MS centers in 4 European countries, encompassing a range of people with MS with varying disabilities and demographics. The second objective (WP3) will be to develop and psychometrically test a range of mobility measures collected by the telehealth system. The third objective (WP4) will be to compare exercise delivered via telehealth with usual care. The primary outcome will be trial feasibility, with preliminary efficacy for mobility, mental health, social participation, and quality of life outcomes. The fourth objective (WP5) will be to conduct an economic evaluation of exercise program delivery via telehealth compared with in-person care. The final objective will be to work collaboratively with clinicians, policymakers, and people with MS and to widely disseminate the knowledge generated by this program to optimize implementation. Figure 1 presents the WPs of the PLATINUMS (Implementation of an Advanced Telerehabilitation Solution for People With Multiple Sclerosis) project, while Table 1 illustrates its expected timeframe.
PLATINUMS (Implementation of an Advanced Telerehabilitation Solution for People With Multiple Sclerosis) project overview based on working packages (WPs). DMSH: Danish Multiple Sclerosis Hospitals; FAIR: findable, accessible, interoperable, and reusable; RCT: randomized controlled trial; TAU: Tel Aviv University; UC: University of Cagliari; UL: University of Limerick.
Research and Innovation Questions
This innovative project will include 5 key research questions (RQs), which we propose will fill in the gaps in our current knowledge.
RQ1 (WP2) is as follows: In people with MS, what is the usability and feasibility of an advanced telerehabilitation system in facilitating remote exercise training? Qualitative and quantitative measures will be used to evaluate the usability and feasibility of the telerehabilitation system in 4 countries. Following necessary system upgrades and adaptations, findings will be incorporated into the feasibility multicenter RCT (WP4). Based on data from other patient populations, we hypothesize that the innovative telerehabilitation system will score highly for usability and feasibility among the participants with MS.
RQ2 (WP3) is as follows: In people with MS, are scores provided by clinical mobility tests obtained via tele-rehabilitation valid and reliable? Evidence for remote mobility evaluation does not currently exist for people with MS. We will evaluate 5 tests developed from commonly used clinical measures. We hypothesize that innovative remote mobility tests will demonstrate good-to-excellent validity and reliability.
RQ3 (WP4) is as follows: In people with MS, is a large multicenter RCT possible, and can it show preliminary efficacy of an individualized exercise program delivered via telerehabilitation to improve mobility compared with in-person physical therapy? An international pragmatic multicenter feasibility RCT will be conducted to compare the effectiveness of delivering the individual exercise program via telerehabilitation versus in person by a physiotherapist. We hypothesize that both exercise intervention programs will improve mobility in people with MS; however, nonsignificant differences in mobility outcome measures between groups (telerehabilitation vs usual care) will be demonstrated.
RQ4 (WP4) is as follows: In people with MS, does an individualized exercise program delivered via telerehabilitation have a comparable effect on mood and quality of life (QoL) compared with standard physical therapy (facility based)? This RQ will be answered in the planned international multicenter feasibility RCT, preceded by a feasibility and usability study. Consequently, our hypothesis is that mood and QoL will be improved in participants whose symptoms are significant at baseline.
RQ5 (WP5) is as follows: In people with MS, does a personalized exercise program delivered via telerehabilitation yield comparable cost-effectiveness value compared with standard physical therapy (facility based)? We hypothesize that the telerehabilitation system will be more cost-effective than personal exercise provided by a physiotherapist. We will account for several potential confounders, such as (1) disability, (2) geographic location, and (3) comorbidities.
Methodology, Approach, and Study Population
The different WPs of the research project and timeline are presented in Figure 1 and Table 1. The first phase of this project will examine the system usability and feasibility of an innovative advanced telerehabilitation system in people with MS (WP2). The system usability and feasibility study will be conducted in each participating country (Israel, Italy, Ireland, and Denmark) with a small group of people with MS (n=10 per center) with varying disability. Participants will be recruited according to the following criteria: aged 18 years or older; confirmed diagnosis of MS based on the McDonald criteria [30] (both relapsing-remitting and progressive MS); an Expanded Disability Status Scale (EDSS) score of 2.5-6.5; willing to travel to the local study site for the evaluation sessions; and internet service, and having a device (eg, smartphone, tablet, or PC) equipped with a camera that meets the technical specifications recommended by the telerehabilitation system manufacturer. Individuals who have had a documented relapse during the past 3 months will be excluded, as will those who are unable to follow simple instructions.
Following assessment and exercise prescription, participants will complete an exercise program delivered by the telerehabilitation system. The short-term program will include 8 exercise training sessions (45- to 60-minute sessions twice weekly for 4 weeks). The amount of training throughout the short-term program will be sufficient for collecting data and taking note of the safety, usability, and feasibility of the advanced rehabilitation technologies [31]. The primary outcome measure of WP2 will be collected at the end of the short-term telerehabilitation exercise program with the Telehealth Usability Questionnaire (TUQ) [32], a solid, robust, and versatile tool used to measure the quality of the telehealth system’s interaction and services. In addition, qualitative data will be collected through semistructured interviews with key stakeholders (people with MS and therapists) and analyzed thematically.
In parallel with the system feasibility and usability study, we plan to develop and psychometrically test a set of remote balance and functional mobility tests delivered via the telerehabilitation system (WP3). We will adapt and manualize 5 remote mobility tests that are collected through the telerehabilitation system: the 30-second sit-to-stand (30STS) test, timed-up-and-go (TUG) test, functional reach test (FRT), 20-second single-leg stance (20SLS) test, and the Short Physical Performance Battery (SPPB). The SPPB includes the following tests: side-by-side stand (10 seconds), semitandem stand (10 seconds), tandem stand (10 seconds), a gait speed test over 3 meters, and a 5-time repeated chair stand test. Upon completion of the developmental phase, we will conduct a test-retest reliability study for in-person and telehealth data capture and a criterion validity study comparing telehealth and in-person data with 15 people with MS (EDSS 2.5-6.5) at each site (n=60).
To examine the efficacy of the advanced telerehabilitation solution for people with MS, we propose an international feasibility multicenter RCT (WP4). We will include a target sample of 24 participants per country (in 4 countries; 96 participants in total) based on the stepped rule of thumb proposed by Whitehead et al [33], who estimated the optimal sample size for an early-stage/pilot RCT to be 24. Importantly, as the results may differ across countries, we consider each country an individual site for the feasibility RCT. Statistical analysis will be performed for the total group and each country separately. The participants will be randomly allocated (individual randomization) into one of two groups: (1) home-based telerehabilitation exercise training via the WizeCare platform [28] or (2) usual care. The sample criteria for the feasibility multicenter RCT will be the same as those for WP2.
Intervention and Comparators
As previously mentioned, the telerehabilitation intervention program will be delivered through the AI telerehabilitation platform designed and marketed by WizeCare [28]. WizeCare is a medium-sized digital health company that has developed an innovative solution for remote physical therapy and exercise training at home. The system includes over 800 exercises that encompass strength, coordination, and flexibility, targeting the lower and upper body and core muscle groups and joints, enabling the therapist to create a tailored exercise program. Moreover, the system includes a technology called MoveAI (patent no. US 11,636,777 B2), which identifies, tracks, and analyzes the user’s movement without requiring customized sensors but instead using the camera available on a smartphone, tablet, or PC. This will provide the user (ie, patient) with immediate feedback and guidance. Figure 2 illustrates key features of the telerehabilitation digital platform. The system is safe and has been confirmed by several security certificates of the highest standard (ISO/IEC 27001:2013; ISO27799:2016; AMAR [Israeli standard]: 29460001). Additional data on adherence and compliance will be collected via the WizeCare telerehabilitation platform.
Key elements of the telerehabilitation digital platform.
The telerehabilitation exercise intervention program will comprise a 10-week, physiotherapist-prescribed, evidence-based, individualized exercise program based on the exercise guidelines for people with MS and the physiotherapist’s clinical reasoning [34]. Eligible participants will receive tailored exercise instructions, which will include performing 8 to 10 exercises in accordance with their abilities and functional needs. Following the first week of training, the participant will be contacted by a physical therapist (via video or audio chat through the system) to monitor participation, progress, and adverse events. Participants in the telerehabilitation group will be compared to those in usual care. Since the term “usual care” is broad, particularly across countries, and physical activity participation varies, participants in both groups will provide weekly information about their physical activity based on the FITT-VP (frequency, intensity, time, type, volume, and progression) principles [35]. To measure adherence, all participants will receive a diary and be requested to log their exercises and submit reports weekly. The report submission will be monitored weekly with a phone call by a physical therapist.
Outcome Measures for the Feasibility Multicenter RCT
The outcome measures for WP4 will include the 30STS [36] (primary outcome), SPPB [37], 6-minute walk test (6MWT) [38], timed 25-foot walk test (T25FWT) [39], mini-BESTest (balance) [40], FRT [41], and a self-report questionnaire, the 12-item MS Walking Scale (MSWS-12) [42]. In accordance with the project’s secondary aims, we will examine the impact of the intervention programs on mood (ie, depression and anxiety with the State-Trait Anxiety Inventory [STAI] [43] and Quick Inventory of Depression Symptomology [QIDS] [44]), quality of life (EQ-5D-5L [45]) and the impact of MS (29-question Multiple Sclerosis Impact Scale; MSIS-29 [46]).
All outcome measures will be collected at baseline (at the initiation of the intervention program), and after the intervention period’s completion. Assessors (physical therapists) will be blinded to group allocation, and patient report outcomes will be collected using an online form. Other significant disease-related factors collected solely at baseline (together with demographic and relevant clinical information) will include perceived fatigue (Modified Fatigue Impact Scale; MFIS [47]) and cognition (Symbol Digit Modality Test; SDMT [48]). Additionally, we will collect baseline information on digital literacy, which may confound the intervention’s effectiveness. All outcome measures used for the study have been validated in people with MS and are recommended for rehabilitation and clinical trials.
Data Analysis and Statistical Plan
Each research question is addressed through specific outcome measures. For RQ1, usability and feasibility will be assessed via the TUQ, adherence rates, dropout rates, and stakeholder interviews, with qualitative data analyzed thematically. RQ2 involves psychometric evaluation of remote assessments (e.g., SPPB, STS, and TUG) using intraclass correlation coefficients for test-retest reliability and Pearson correlations to compare remote and in-person scores. RQ3 and RQ4 outcomes (eg, 30STS, MSWS-12, EQ-5D-5L, STAI, and QIDS) will be analyzed using linear mixed models to assess within- and between-group effects over time. The primary analysis will follow an intention-to-treat principle, including all randomized participants in the groups to which they were originally assigned, regardless of adherence to the intervention protocol. A per-protocol analysis may be conducted as a secondary exploratory analysis. Missing data will be addressed using multiple imputation, assuming data are missing at random, and sensitivity analyses will be performed to assess the robustness of results.
As part of RQ5, the study also incorporates a comprehensive economic evaluation of the telerehabilitation system, which complements the clinical analyses and addresses a critical gap in MS rehabilitation research. A cost-utility analysis will be conducted to compare the telerehabilitation intervention and usual care, using incremental cost-effectiveness ratios derived from health care service use data and EQ-5D-5L–based quality-adjusted life years. Cost data will include implementation, infrastructure, maintenance, training, support services, and any differences in health service use or patient-reported outcomes. These data will be collected alongside the RCT to ensure alignment between clinical effectiveness and economic impact.
Ethical Considerations
Ethical approval has been obtained for WP2 from the Sheba Institutional Review Board (IRB; SMC-1154-24; May 1, 2024); the University of Limerick Education and Health Sciences Research Ethics Committee (2025_01_17_EHS; May 11, 2025); and the Central Denmark Region Committees on Health Research Ethics (1-10-72-140-24). Approval of the ethics application for WP3 is expected by September 2025. Ethics applications for the remaining WPs, including the multicenter feasibility RCT (WP4) and the economic evaluation (WP5), will be submitted to the appropriate IRB in each participating country prior to their initiation.
For WP2, all participants provide written informed consent prior to enrollment. The consent process includes comprehensive information on the study procedures, risks, benefits, and data confidentiality. All collected data are deidentified prior to analysis and securely stored in accordance with institutional data protection policies. Participants in WP2 do not receive financial compensation but may be reimbursed for travel expenses when applicable. Compensation for WP3 and future phases will be determined and approved through local IRB processes. No identifiable images or personal information will be included in the manuscript or any supplementary materials. If such materials are necessary for dissemination, explicit written consent will be obtained and submitted as required.
Results
The PLATINUMS project received official funding in February 2024. Data collection for WP2 (the system usability and feasibility study) began in April 2025 across participating sites in Israel, Italy, Ireland, and Denmark. WP3 (validation of remote mobility measures) is scheduled to launch in September 2025, and the multicenter RCT (WP4) is planned to begin in January 2026. Project coordination and dissemination activities (WP7) have been ongoing since March 2025. Initial findings from WP2 are expected to be available by October 2025, with preliminary publications planned for mid-2026.
Discussion
The PLATINUMS project aims to evaluate an innovative AI-based telerehabilitation system for people with MS, and if successful, it is expected to significantly advance the way rehabilitation is delivered to this population. The system is designed to provide accessible, individualized exercise programs with real-time feedback and therapist supervision, thereby overcoming some of the longstanding barriers to facility-based care. Through its structured, multiphase approach, the project will generate essential data on usability, feasibility, clinical validity of remote assessments, and preliminary efficacy of telerehabilitation interventions.
This protocol builds on a growing body of research demonstrating the potential of telerehabilitation to support physical function in people with MS while addressing several limitations observed in earlier studies. A recent scoping review identified two main categories of telerehabilitation interventions, exergaming and web-based physical therapy, both of which have shown promising results in improving gait and balance in people with MS [49]. For example, exergaming systems such as Microsoft Kinect–based virtual reality and home-based balance training tools led to significant improvements in ambulation speed, dynamic balance, and postural control [50,51]. Similarly, web-based physical therapy programs, including both those with real-time supervised and asynchronous formats, have demonstrated improvements in gait function and balance scores [52,53].
While previous interventions often lacked scalability or relied on specialized hardware, the PLATINUMS system leverages AI and widely available consumer devices, making it more practical for widespread use. The planned international feasibility trial further enhances the study’s relevance by including participants across diverse health care contexts, thereby increasing the potential for future implementation.
A particular strength of this study is its integration of technological innovation with a rigorous clinical and economic evaluation. By examining feasibility alongside psychometric testing and cost-effectiveness, the project will provide comprehensive insights into the practicality of scaling up such solutions in real-world settings. The inclusion of both patient-centered outcomes and system-level data will allow for a nuanced understanding of how AI-driven telerehabilitation can influence care delivery for people with MS. Still, as this is a protocol, all conclusions must remain provisional until data collection is complete. It will be important to interpret future findings with an understanding of the feasibility trial’s exploratory nature.
Several limitations and potential challenges should be acknowledged. First, as a feasibility study, the sample size may not be sufficient to detect small but clinically meaningful effects, and findings may not be generalizable beyond the populations and settings involved. Second, adherence to home-based interventions can be variable and difficult to monitor objectively outside controlled settings. To address this, we will incorporate remote use tracking, patient engagement strategies, and therapist follow-up. Third, technical issues such as hardware compatibility, internet connectivity, and user literacy may affect intervention delivery. These will be documented throughout the study and considered in the interpretation of results. Importantly, as with any AI-enabled solution, algorithm transparency, how well it can adapt to individual needs, and potential biases must be critically evaluated before broader deployment. Given that this is a feasibility protocol, any conclusions will remain provisional until the trial is completed and the data are evaluated.
Looking forward, the outcomes of this study are expected to inform the design of a fully powered RCT, as well as broader efforts to integrate digital health technologies into routine clinical practice. The knowledge generated may also prove relevant to other neurological conditions where mobility impairments are prevalent. A dedicated dissemination strategy has been developed to ensure that findings reach key stakeholders, including clinicians, patients, and health policy decision-makers. Ultimately, the PLATINUMS project seeks not only to assess a novel intervention but to lay the groundwork for a more accessible, personalized, and sustainable model of rehabilitation for people with MS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Walton C King R Rechtman L Kaye W Leray E Marrie RA Robertson N La Rocca N Uitdehaag Bvan der Mei I Wallin M Helme A Angood Napier C Rijke N Baneke P Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition Mult Scler 202012261418161821 10.1177/13524585209708413317447533174475 PMC 7720355 · doi ↗ · pubmed ↗
- 2Heesen CBöhm J Reich C Kasper J Goebel M Gold S Patient perception of bodily functions in multiple sclerosis: gait and visual function are the most valuable Mult Scler 2008081479889110.1177/135245850808891618505775135245850808891618505775 · doi ↗ · pubmed ↗
- 3Green R Cutter G Friendly M Kister I Which symptoms contribute the most to patients' perception of health in multiple sclerosis?Mult Scler J Exp Transl Clin 2017332055217317728301 10.1177/20552173177283012890481110.1177_205521731772830128904811 PMC 5588807 · doi ↗ · pubmed ↗
- 4van der Feen Fde Haan Gvan der Lijn I Heersema D Meilof J Heutink J Independent outdoor mobility of persons with multiple sclerosis - A systematic review Mult Scler Relat Disord 20200137101463 10.1016/j.msard.2019.10146331678858 S 2211-0348(19)30452-331678858 · doi ↗ · pubmed ↗
- 5Kalron A Dvir Z Achiron A Walking while talking--difficulties incurred during the initial stages of multiple sclerosis disease process Gait Posture 201007323332510.1016/j.gaitpost.2010.06.00220594850 S 0966-6362(10)00160-820594850 · doi ↗ · pubmed ↗
- 6Skjerbæk Anders G Dalgas U Stenager E Boesen F Hvid LG The six spot step test is superior in detecting walking capacity impairments compared to short- and long-distance walk tests in persons with multiple sclerosis Mult Scler J Exp Transl Clin 20239420552173231218127 10.1177/205521732312181273810580610.1177_2055217323121812738105806 PMC 10722939 · doi ↗ · pubmed ↗
- 7Souza A Kelleher A Cooper R Cooper RA Iezzoni LI Collins DM Multiple sclerosis and mobility-related assistive technology: systematic review of literature J Rehabil Res Dev 20104732132310.1682/jrrd.2009.07.00962066534720665347 · doi ↗ · pubmed ↗
- 8Zanotto T Sosnoff JJ Backus D Yarnot R Worikat NA Abou L Peterson EW Rice LA Characteristics and consequences of falls among people with multiple sclerosis who use wheelchairs or scooters: Differences between injurious and non-injurious falls Mult Scler Relat Disord 20230573104631 10.1016/j.msard.2023.10463136963170 S 2211-0348(23)00135-936963170 · doi ↗ · pubmed ↗