Decompensated Hypothyroidism in a Patient With Cirrhosis: A Rare Presentation of Severe Hypothyroidism With Hypertension
Kareem Malas, Grant Herrington, Nam Pham, Adan Mora

TL;DR
A rare case of severe hypothyroidism with hypertension in a cirrhosis patient is presented, highlighting the challenges of diagnosis and treatment.
Contribution
This paper presents a unique clinical case linking decompensated hypothyroidism and hypertension in a cirrhosis patient.
Findings
A 79-year-old cirrhosis patient showed severe hypothyroidism with high blood pressure.
Intravenous levothyroxine improved the patient's condition within 4 days.
Hypertension may result from compensatory vasoconstriction in low cardiac output.
Abstract
Decompensated hypothyroidism (DH) is a rare endocrine emergency with a high mortality rate, particularly challenging to distinguish from hepatic encephalopathy (HE) in patients with cirrhosis due to overlapping symptoms. We present a case of a 79-year-old woman with advanced cirrhosis and a history of multiple HE-related admissions, who exhibited altered mental status, hypothermia, bradycardia, and unusually high blood pressure. Laboratory findings revealed a severely elevated thyroid-stimulating hormone level (335.10 µUI/mL; reference range, 0.40-4.50 µUI/mL) and low free thyroxine level (0.2 ng/dL; reference range, 0.8-1.8 ng/dL), confirming DH. Adrenal insufficiency was ruled out. Intravenous levothyroxine was administered with a dose adjustment over 4 days, leading to significant clinical improvement by hospital day 1 and recovery to baseline by day 4. This case highlights the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
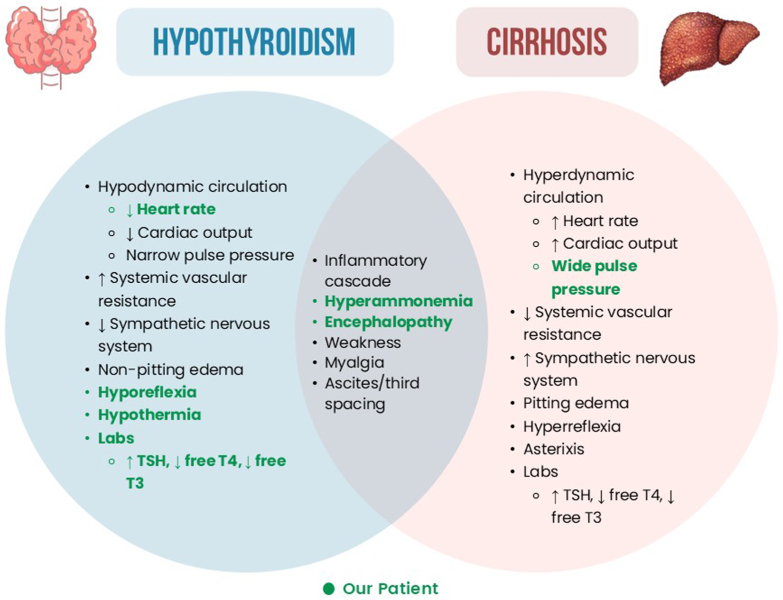 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Thyroid Disorders and Treatments · Liver Disease Diagnosis and Treatment
Highlights
- •Decompensated hypothyroidism (DH) can mimic or worsen hepatic encephalopathy (HE), complicating diagnosis in cirrhosis
- •Hypothyroidism can elevate ammonia, worsening HE in patients with cirrhosis
- •Thyroid function should be re-evaluated in patients with cirrhosis with bradycardia and hypothermia
- •DH-induced low cardiac output may cause paradoxical, compensatory hypertension
- •Age and comorbidities should be considered when choosing intravenous thyroid replacement strategy
Clinical RelevanceThe case highlights the diagnostic challenges of decompensated hypothyroidism (DH) in cirrhosis, where symptoms can overlap. This report emphasizes the need for thyroid function evaluation in encephalopathy and importance of individualized thyroid hormone replacement strategies. Awareness of concomitant DH in cirrhosis enables early recognition and treatment of thyroid dysfunction, improving outcomes.
Introduction
Decompensated hypothyroidism (DH), formerly known as myxedema coma, is a rare endocrine emergency with a 30% to 60% mortality rate. The liver plays an important role in thyroid hormone metabolism with the production of thyroid binding proteins and conversion of thyroid hormones. Differentiating DH from hepatic encephalopathy (HE) can be difficult due to overlapping symptoms.1 Manifestations of DH can mask those of decompensated cirrhosis and vice versa. Both share and have opposing pathophysiology and clinical consequences (Fig.). Concomitant presentation offers unique clinical challenges. We report a rare case of DH in a patient with cirrhosis requiring intensive medical care.FigVenn diagram comparing notable clinical findings in hypothyroidism and cirrhosis. The overlapping section represents shared clinical features, whereas unique findings for each condition are shown in the respective nonoverlapping areas. Findings designated in green were observed in our patient case. T4 = thyroxine; TSH = thyroid-stimulating hormone; T3 = triiodothyronine.
Case Report
A 79-year-old woman with a past medical history of hypertension (HTN), chronic kidney disease stage V, and advanced metabolic dysfunction–associated steatotic liver disease complicated by esophageal varices, recurrent ascites requiring weekly paracentesis, and multiple admissions for HE presented with 3 days of progressively worsening mental status and cold intolerance. Of note, she was hospitalized 2 months prior for HE and had been compliant with her home lactulose regimen.
On arrival, she was hypothermic (94.3 °F), hypertensive (178/65 mm Hg), and bradycardic (59 bpm). The respiratory rate and oxygen saturation were normal on room air. Pertinent examination findings included the following: (1) ill-appearing and frail, (2) lethargic, (3) moaned to questions, (4) distended but soft abdomen with wincing to palpation, (5) cool extremities, (6) hyporeflexia, (7) absent asterixis, and (8) alert and oriented ×0. Laboratory results revealed a severely elevated thyroid-stimulating hormone level (335.10 µUI/mL; reference [ref.] range, 0.40-4.50 µUI/mL; 2 months prior, 6.15 µUI/mL) and low free thyroxine level (0.2 ng/dL; ref. range, 0.8-1.8 ng/dL; 2 months prior, 1.5 ng/dL). Subsequently, an adrenocorticotropic hormone stimulation test was performed with a baseline cortisol level of 13.2 µg/dL and 60-minute cortisol level of 18.9 µg/dL, ruling out adrenal insufficiency. Other initial studies included the following: (1) aspartate aminotransferase level, 82 units/L (ref. range, 10-35 units/L); (2) alanine aminotransferase level, 21 units/L (ref. range, 10-35 units/L); (3) total bilirubin level, 2.2 mg/dL (ref. range, 0.2-1.3 mg/dL), (4) international normalized ratio, 1.8 (ref. range, 0.9-1.3); and (5) ammonia level, 96 µmol/L (2 months prior, 254 µmol/L; ref. range, 13-40 µmol/L).
Given her advanced age and severe comorbidities, intravenous (IV) thyroid replacement dosing was split over 3 days. Her thyroid replacement consisted of the following: (1) hospital day (HD) #0, IV levothyroxine 150 µg; (2) HD #1, IV levothyroxine 80 µg; (3) HD #2, IV levothyroxine 40 µg + 88 µg orally; (4) HD #3, IV levothyroxine 50 µg; and (5) HD #4, transitioned to stable dose of levothyroxine 88 µg orally daily. The free thyroxine level was trended daily and normalized by HD #1 and was 1.1 ng/dL on HD #4. She demonstrated robust improvement by HD #1 marked by improved mentation and resolution of hypothermia and bradycardia. By HD #4, she recovered to clinical baseline with a temperature of 98.1 °F, blood pressure of 142/63 mm Hg, and heart rate of 78 bpm. A summary of the hospital course with information including thyroid function and clinical status can be visualized in the Table.TableSummary of Hospital Course by Hospital Day, Thyroid-Stimulating Hormone Level (µIU/mL; Reference Range, 0.40-4.50 µIU/mL), Free Thyroxine Level (ng/dL; Reference Range, 0.8-1.8 ng/dL), Levothyroxine Dosing, and Clinical StatusHD #TSH (µIU/mL)Free T4 (ng/dL)LevothyroxineClinical status−2 mo6.151.5NoneHE admission03350.2IV 150 µgCritically ill1…1.2IV 80 µgRobust improvement2…1.0IV 40 µg + 88 µg orally…3…1.2IV 50 µg…4…1.188 µg orallyRecovery to baselineAbbreviations: HD = hospital day; HE, hepatic encephalopathy; IV = intravenous; T4 = thyroxine; TSH = thyroid-stimulating hormone.HD # “−2 mo” refers to a hospitalization for HE 2 months prior to this case.
Discussion
Our patient had signs/symptoms of sudden-onset DH with atypical features in a background of HE and HTN. Although diastolic HTN has been described in hypothyroidism, this patient had pronounced systolic HTN with a wide pulse pressure over 100 bpm. Cirrhosis is a state of hyperdynamic circulation with increased cardiac output and reduced systemic vascular resistance. We propose that without evidence of adrenal insufficiency, peripheral vascular HTN was compensatory for DH-induced low cardiac output, which later may have progressed to shock if untreated. Although hypothermia is uncommon in HE, patients with decompensated cirrhosis are at increased risk of sepsis, a potential cause of hypothermia. However, a broad infectious workup was negative on presentation. In the absence of infection, the hypothermia was attributed to DH via impaired metabolism and reduced heat production. Hypothyroidism is theorized to cause increased ammonia due to decreased protein synthesis, increased protein catabolism, decreased intestinal motility that promotes bacterial ammonia production, and decreased glutamine synthase activity.2 Rare cases such as this have been reported with hyperammonemia that did not improve with standard HE treatment and were found to have DH, which responded to levothyroxine treatment.3, 4, 5, 6 A low free triiodothyronine level has been associated with systemic inflammation, acute-on-chronic liver failure, and mortality, whereas a low thyroxine level has been associated with the development of advanced HE.7^,^8 Free thyroid hormone reduction is often indicative of thyroid compensation to a nonthyroidal illness, that is, euthyroid sick syndrome. She was not given hydrocortisone because the baseline cortisol was adequate and adrenocorticotropic hormone stimulation test was robust. IV levothyroxine was administered due to suspected low bioavailability due to gut edema observed in DH, and lower doses were chosen given arrhythmia risk related to age and other risk factors. Despite a very recent thyroid evaluation during her prior admission, thyroid-stimulating hormone was tested given the peculiar findings of hypothermia, bradycardia, and cold intolerance. This case also served as a testament to avoid anchoring bias that would lead to the assumption that her presentation was driven by HE similar to prior hospitalizations. It was not clear why the patient developed such drastic hypothyroidism despite demonstrating stable subclinical hypothyroidism just 2 months prior. There were no evident triggers such as adverse medication effects or infection. However, there have been reports of similar presentations of rapid progression to DH in elderly individuals with high antithyroid antibody titers.9 Antithyroid antibody was not evaluated in this patient, and thus, it cannot be determined whether this mechanism contributed to her presentation.
Conclusion
This case highlights the importance of recognizing DH as a potential contributor to altered mental status in patients with cirrhosis. The interplay between DH and HE presents unique diagnostic and management challenges, requiring a high index of suspicion and thorough evaluation. Our case underscores the need for repeated thyroid function testing in critically ill patients, even those with recent thyroid assessments, when atypical findings such as hypothermia, bradycardia, and cold intolerance are present. Furthermore, the paradoxical hemodynamic presentation of systolic HTN observed in our patient raises questions about compensatory mechanisms in cirrhosis that warrant further exploration. Tailoring the approach to IV thyroid replacement in these critical scenarios, with heavy consideration of the patient’s advanced age and comorbidities, offers a delicate perspective on the management of DH in patients with cirrhosis. By presenting this case, we aim to enhance awareness of DH in patients with advanced liver disease, promote early recognition, and optimize management strategies to improve patient outcomes.
Disclosure
The authors have no conflicts of interest to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Punekar P.Sharma A.K.Jain A.A study of thyroid dysfunction in cirrhosis of liver and correlation with severity of liver disease Indian J Endocrinol Metab 225201864565010.4103/ijem.IJEM_25_1830294575 PMC 6166553 · doi ↗ · pubmed ↗
- 2Rimar D.Kruzel-Davila E.Dori G.Baron E.Bitterman H.Hyperammonemic coma--barking up the wrong tree J Gen Intern Med 224200754955210.1007/s 11606-007-0131-617372808 PMC 1829435 · doi ↗ · pubmed ↗
- 3Thobe N.Pilger P.Jones M.P.Primary hypothyroidism masquerading as hepatic encephalopathy: case report and review of the literature Postgrad Med J 76897200042442610.1136/pmj.76.897.42410878207 PMC 1741656 · doi ↗ · pubmed ↗
- 4Yamamoto T.Takeuchi K.Okuda C.Symptomatic hypothyroidism in decompensated liver cirrhosis J Clin Gastroenterol 332200117217310.1097/00004836-200108000-0002011468452 · doi ↗ · pubmed ↗
- 5Khairy R.N.Mullen K.D.Hypothyroidism as a mimic of liver failure in a patient with cirrhosis Ann Intern Med 1464200731531610.7326/0003-4819-146-4-200702200-0002117310062 · doi ↗ · pubmed ↗
- 6Bassi R.Rayamajhi S.Essilfie-Quaye K.Randhawa J.Padam S.Uncontrolled primary hypothyroidism precipitating non-cirrhotic hyperammonemia: a unique interplay between the liver and thyroid Cureus 1642024 e 5786110.7759/cureus.57861 PMC 1107858338721206 · doi ↗ · pubmed ↗
- 7Hartl L.Simbrunner B.Jachs M.Lower free triiodothyronine (f T 3) levels in cirrhosis are linked to systemic inflammation, higher risk of acute-on-chronic liver failure, and mortality JHEP Rep 61202310095410.1016/j.jhepr.2023.100954 PMC 1073310138125301 · doi ↗ · pubmed ↗
- 8Bajaj J.S.Tandon P.O’Leary J.G.Admission serum metabolites and thyroxine predict advanced hepatic encephalopathy in a multicenter inpatient cirrhosis cohort Clin Gastroenterol Hepatol 214202310311040.e 310.1016/j.cgh.2022.03.04635436625 PMC 11000256 · doi ↗ · pubmed ↗