Fractionated Stereotactic Radiotherapy for Brain Metastases: A Moroccan Multicenter Experience
Fatima Safini, Zainab Oumouloud, Abdelkader Acharki, Issam Lalya, Nadia Benchakroun, Selma Kadiri, Mehdi El Ouartiti, Najib Derhem, Abdelmounaim Zayane, Abdenbi El Moutaoukkil, Khawla Lfara, Bouchra Amaoui

TL;DR
This study shares a Moroccan experience using stereotactic radiotherapy for brain metastases, showing effectiveness but calling for better guidelines.
Contribution
The paper presents a multicenter Moroccan experience on fractionated stereotactic radiotherapy for brain metastases.
Findings
The most common primary tumor was lung cancer, followed by breast cancer.
Overall survival at 24 months was 48.2%.
The majority of patients had fewer than three metastases.
Abstract
Introduction: Stereotactic radiotherapy is currently an essential therapeutic tool in the treatment of brain metastases. The aim of our study was to report a multicenter Moroccan experience on stereotactic radiotherapy using linear accelerators in the treatment of brain metastases. Material and methods: We conducted a multicenter retrospective study that included 130 patients treated at five centers in Morocco for brain metastases during the period between January 2021 and December 2024. All patients received fractionated stereotactic radiotherapy delivered by a linear accelerator. Statistical analysis of the data was performed using Jamovi version 2.3. Results: We collected 130 patients with 248 treated brain metastases. The mean age was 58.4 (24-88) with a female predominance (59.2%). The most common primary tumor was lung cancer (77 patients, 59.2%), followed by breast cancer (29…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
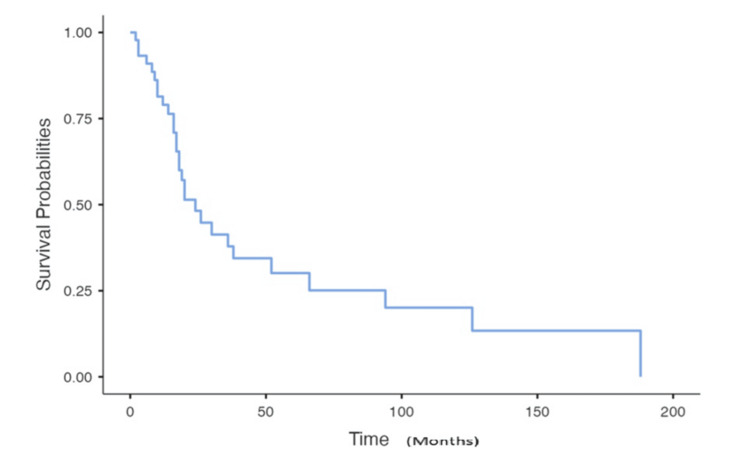 Figure 1
Figure 1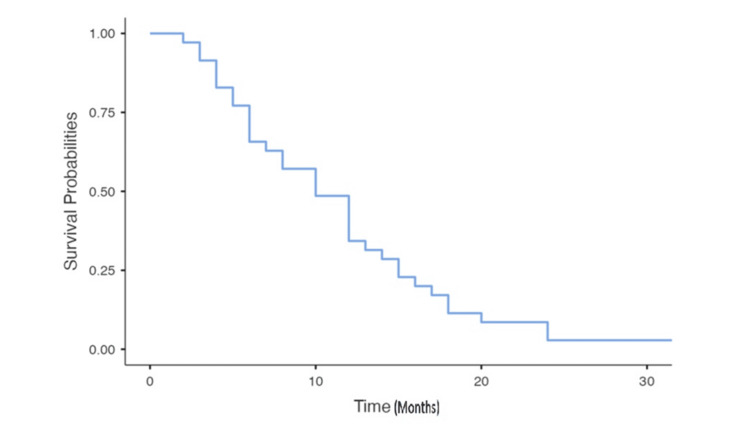 Figure 2
Figure 2| Characteristics | Value |
| Patient age (years), median | 58 (24-88) |
| Sex, n (%) | |
| Men | 77 (59.2%) |
| Women | 53 (40.8%) |
| Primary cancer, n (%) | |
| Lung cancer | 77 (59.2%) |
| Breast cancer | 29 (22.3%) |
| Gastrointestinal carcinoma | 10 (7.7%) |
| Malignant melanoma | 3 (2.3%) |
| Renal cell carcinoma | 3 (2.3%) |
| Gynecological cancer | 4 (3%) |
| Other | 4 (3%) |
| Histology | |
| ADK | 104 (73.5%) |
| SCC | 11 (8.5%) |
| CCC | 3 (2.3%) |
| Melanoma | 3 (2.3%) |
| Neuroendocrine tumors | 3 (2.3%) |
| Others | 6 (4.6%) |
| Characteristics | Value |
| WBRT before RS | |
| Yes | 9 (6.9%) |
| No | 121 (93.1%) |
| Metastasis surgery | |
| Yes | 6 (4.6%) |
| No | 124 (95.4%) |
| Systemic treatment | |
| Yes | 31 (23.8%) |
| Missing/unknown | 99 (76.2%) |
| Extracranial metastases, n (%) | |
| Yes | 48 (65.8%) |
| No | 25 (34.2%) |
| Missing/unknown | 9 (12.3%) |
| Time of occurrence | |
| Synchronous | 63 (48.5%) |
| Metachronous | 67 (51.5%) |
| Number of metastases | |
| 1 | 73 (56.6%) |
| 2 | 27 (20.9%) |
| 3 | 12 (9.3%) |
| 4 | 12 (9.3%) |
| ≥5 | 6 (3.9%) |
| Max diameter lesion (median value) (cm) | 2.2 (0.4-6.3) |
| Lesion volume (median value) (cm3) | 8 cc (0.05-89) |
| Radiation dose (Gy) | |
| 3 × 7 | 5 (4%) |
| 3 × 7.7 | 5 (4%) |
| 3 × 8 | 17 (13%) |
| 3 × 9 | 37 (28%) |
| 3 × 10 | 21 (16%) |
| 3 × 11 | 5 (4%) |
| 5 × 6 | 37 (28%) |
| 5 × 7 | 4 (3%) |
| Response of the metastases on 1st follow-up, n (%) | |
| Responsive disease | 17 (13%) |
| Stable disease | 18 (13.9%) |
| Progressive disease | 24 (18.5%) |
| Missing/unknown | 71 (54.6%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Glioma Diagnosis and Treatment · Advanced Radiotherapy Techniques
Introduction
Brain metastases (BM) continue to be a major significant cause of morbidity and mortality in patients with metastatic cancer. More than 100,000 persons are diagnosed annually, and approximately 10%-30% of cancer patients will develop BM during the course of their disease [1]. Cerebral stereotactic radiotherapy represents a major advance in the treatment of BM. This high-precision technique delivers high doses to the tumor while preserving the surrounding normal brain tissue, thus improving local control and quality of life for patients [2]. This radiotherapy can be performed either in a single fraction (stereotactic radiosurgery (SRS)) or in several fractions (fractionated stereotactic radiotherapy (FSRT)). In this study, we report on a multicenter Moroccan experience of stereotactic radiotherapy using a linear accelerator in the treatment of BM.
Materials and methods
This retrospective multicenter study was conducted across five radiotherapy institutions in Morocco: Ryad Oncologia Clinic (Casablanca), Nakhil Centre of Oncology (Rabat), Agadir International Hospital, Akdital (Agadir), Cheikh Maelainin Clinic (Agadir), and Atlantic Centre of Oncology (Agadir). We included patients irradiated in these different centers during the period between January 2021 and December 2024. All patients received FSRT, whether with single or multiple BM. All patients were treated with a linear accelerator. We excluded from our study patients treated with a single fraction or those treated with standard fractionation. Data were collected from patients' clinical records using a common data collection form, while respecting anonymity. Statistical analysis was performed using Jamovi version 2.3 (2022). The results of the analysis of quantitative variables were expressed as means and standard deviations, and those of categorical variables as numbers and frequencies. Kaplan-Meier curves were used to express overall survival and survival after the occurrence of BM.
Results
One hundred and thirty patients with 248 BM treated in the five centers during the years 2021 and 2024 were enrolled in this retrospective study. The mean age of our patients was 58.4 years (range 24-88 years). Male predominance was noted, with 78 men (59.2% of cases) and 53 women (40.8% of cases). As regards the primitive tumors, we noted a predominance of bronchopulmonary cancer (77 cases, 59.2%), followed by breast cancer (29 cases, 22.3%) and gastrointestinal cancer (10 cases, 7.7%). BM were metachronous in 67 patients, with a mean time to onset after diagnosis of the primitive tumor of 26 months. BM occurred in an oligometastatic context in 40 patients (67.8%). A summary of the characteristics of patients treated with FSRT is presented in Table 1.
The mean value of the maximum diameter of the lesions was 23.8 mm (4-63 mm). Majority of the lesions were smaller than 30 mm, with a median volume of 8 cc (0.05-89). Most patients were treated for a single BM (56.6%) or two metastases (20.9%), without prior brain radiotherapy in 93.1% of cases. For the planning target volume (PTV), a 2 mm margin was applied to the gross tumor volume (GTV) in the majority of cases, but other margins were used: 3 mm in 23% of cases and 1 mm in 16% of cases. The mono-isocentric technique was used in 84.9% of cases. Different dose fractionations were used. Radiation therapy was delivered in three fractions of 7-11 Gy in 89 cases (68.5%), followed by five fractions of 6-7 Gy in 41 cases (31.5%) with an average biologically effective dose with α/β = 10 (BED10) of 51 (Table 2).
Follow-up data were available for only 59 patients. After a median follow-up of 10.9 months since the onset of BM, we observed stability in 18 patients, complete response in 17 patients, and progression in 24 patients. Overall survival at 24 months was 48.2%, with a median survival after BM of 10 months (Figures 1, 2).
Overall survival according to Kaplan-Meier curves
Survival after the occurrence of brain metastases
Discussion
Radiotherapy in Morocco has made giant technological strides, with 39 anti-cancer centers (public and private sectors) and over 70 linear accelerators at last count in 2023, making Morocco one of the best-equipped countries in Africa [3]. Although stereotactic radiation has been used in Morocco for over a decade, the practice has only become widespread in the various regions of the country in the last five years. The treatment of BM, initially based on whole-brain radiation therapy (WBRT), has benefited from technical advances in radiotherapy, especially stereotactic radiotherapy. This technique reduced neurocognitive complications and ensured good local control [4,5]. The choice between SRS (monofraction) and FSRT depends on the characteristics of the BM (number, size, and location). FSRT is generally preferred to SRS in cases of large BM, proximity to critical organs at risk (brainstem, chiasma, optic nerves, and hippocampus), or prior irradiation or in patients with comorbidities, especially vascular ones [6]. In our series, all patients received FSRT regardless of tumor size and location. More than half the metastases were less than 3 cm in diameter, and prior irradiation was reported in only nine patients (6.9%). The number of metastases treated with FSRT can be as high as 10 lesions. The prospective trial by Shuto et al. whose mature data were published in 2018 with a 60-month follow-up in 784 patients with BM from a pulmonary primary demonstrated that overall survival and side effects were the same in the groups with two to four and with five to 10 metastases [7]. The other parameter used to decide whether or not SRS is feasible is the total cumulative volume of BM expressed in mL or cm^3^. Various threshold values have been proposed in the literature: 7 cm^3^ (a sphere 2.4 cm in diameter) in the guidelines of the American Association of Neurosurgeons [8], 15 cm^3^ in the study by Yamamoto et al., and 30 cm^3^ in the Anocef guidelines (a sphere 3.9 cm in diameter) [9]. Margins around the GTV remain debatable and vary in the literature between no margin and 2 mm [10]. Kirkpatrick et al. randomly compared a GTV margin of 1 mm with 3 mm. They found no difference in terms of local control or occurrence of radionecrosis [11]. In our study, we observed a disparity in margins between the different centers.
FSRT has been used to reduce the risk of radionecrosis compared with single-fraction SRS. Lehrer et al.'s meta-analysis, which included 24 studies, attempted to compare local control and toxicity outcomes between these two fractionations for large-volume metastases. The authors concluded that hypofractionated stereotactic radiotherapy (HFSRT) maintains good local control while reducing the risk of radionecrosis [12]. FSRT delivers a high BED10 Gy while reducing the dose to organs at risk. Note that a low BED is associated with poor local control. The minimum BED10 Gy should be greater than 50 Gy, but a very high BED is associated with complications such as radionecrosis. The dose and protocols to be delivered in FSRT are not well codified. Numerous protocols and fractionations have been published in the literature, but treatment in three or five fractions remains the most widely used. The dose per fraction varies between 4 and 10 Gy in 10 to three fractions. The study by Wu et al., which aimed to establish a dose-response relationship between physical dose (BED) and local control in patients treated with FSRT using a linear accelerator, emphasized the importance of the mean dose and the dose received at the center of the PTV [13]. In our Moroccan context, we unfortunately do not have any guidelines for stereotactic radiotherapy of BM. The choice of dose and fractionation depends on the experience of the doctors and the habits of each center.
This study has many limitations. We were unable to obtain local control or toxicity data. Also, given the retrospective nature of the study, the limited sample size, and the use of different doses, correlation analyses to determine prognostic and predictive factors were not possible. We were unable to collect control imaging and toxicity data. In this study, we have no data on the systemic treatment received by patients, with disparities in practice between different centers (different PTV margins, dose, and fractionation).
Conclusions
This multicenter study reports the first Moroccan experience with FSRT of BM using a linear accelerator. Although our study has a short follow-up time and few data on the evolution, it is an interesting experience that highlights the need to establish national recommendations in order to speak the same language, to have homogeneous data, and to develop national reference systems to improve our oncological results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of brain metastases Neurosurg Clin N Am Sacks P Rahman M 4814883120203292134510.1016/j.nec.2020.06.001 · doi ↗ · pubmed ↗
- 2Radiotherapy for brain metastases (Article in French)Cancer Radiother Latorzeff I Antoni D Gaudaire-Josset S Feuvret L Tallet-Richard A Truc G Noël G 0720 Suppl 201610.1016/j.canrad.2016.07.04127523410 · doi ↗ · pubmed ↗
- 3Stereotactic radiotherapy in Morocco: inventory and technological compatibility with the minimum requirements of international recommendations of good practice (Article in French)Cancer Radiother Lalya I Benchakroun N Sifat H 6766812720233748246510.1016/j.canrad.2023.06.007 · doi ↗ · pubmed ↗
- 4Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: a randomized clinical trial JAMA Brown PD Jaeckle K Ballman KV 40140931620162745894510.1001/jama.2016.9839 PMC 5313044 · doi ↗ · pubmed ↗
- 5Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial Lancet Oncol Chang EL Wefel JS Hess KR 103710441020091980120110.1016/S 1470-2045(09)70263-3 · doi ↗ · pubmed ↗
- 6Fractionated stereotactic intensity-modulated radiotherapy for large brain metastases: comprehensive analyses of dose-volume predictors of radiation-induced brain necrosis Cancers (Basel) Murai T Kasai Y Eguchi Y 16202410.3390/cancers 16193327 PMC 1148263939409947 · doi ↗ · pubmed ↗
- 7Multiinstitutional prospective observational study of stereotactic radiosurgery for patients with multiple brain metastases from non-small cell lung cancer (JLGK 0901 study-NSCLC)J Neurosurg Shuto T Akabane A Yamamoto M 869412920183054429110.3171/2018.7.GKS 181378 · doi ↗ · pubmed ↗
- 8Congress of Neurological Surgeons systematic review and evidence-based guidelines for the treatment of adults with metastatic brain tumors: executive summary Neurosurgery Olson JJ Kalkanis SN Ryken TC 5505528420193062921810.1093/neuros/nyy 540 · doi ↗ · pubmed ↗