Efficacy of Topical Phenytoin in the Management of Diabetic Foot Ulcers: A Systematic Review
Charles P Barry, Mohamed Shefan S Hameed, Abilash Sathyanarayanan

TL;DR
This review examines whether phenytoin is effective for treating diabetic foot ulcers but finds insufficient evidence to support its use.
Contribution
The study systematically evaluates the quality and outcomes of phenytoin trials for diabetic foot ulcers, highlighting methodological flaws.
Findings
23 studies were reviewed, with 20 recommending phenytoin, but most had poor methodological quality.
Lack of blinding and randomization details in most studies prevented a meta-analysis.
Current evidence does not support phenytoin's efficacy for diabetic foot ulcers.
Abstract
Phenytoin has been used as an anti-seizure medication since 1939. There has been interest in its healing properties, with many randomized controlled trials (RCTs) investigating and recommending its use in diabetic foot ulcer (DFU) disease. Despite this, the International Working Group on the Diabetic Foot (IWGDF) does not support its use. The objective of this systematic review was to assess the use of phenytoin in the treatment of DFU disease compared to a control. Systematic searches of Medline, Embase, Google Scholar, the Cochrane Library, and ClinicalTrials.gov were conducted on January 5, 2024, using the keywords "phenytoin", "diabetes", "ulcer", and "RCT". Methodological quality was assessed using the Risk of Bias 2 (RoB 2) tool. A total of 23 studies were included in the systematic review, of which 20 recommended the use of phenytoin. However, the quality of the studies was poor.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
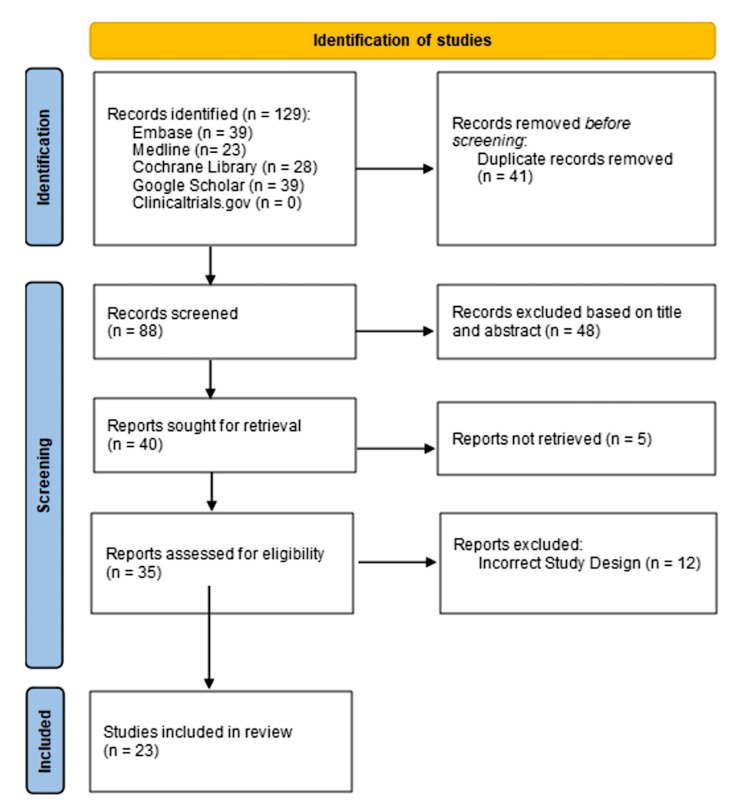 Figure 1
Figure 1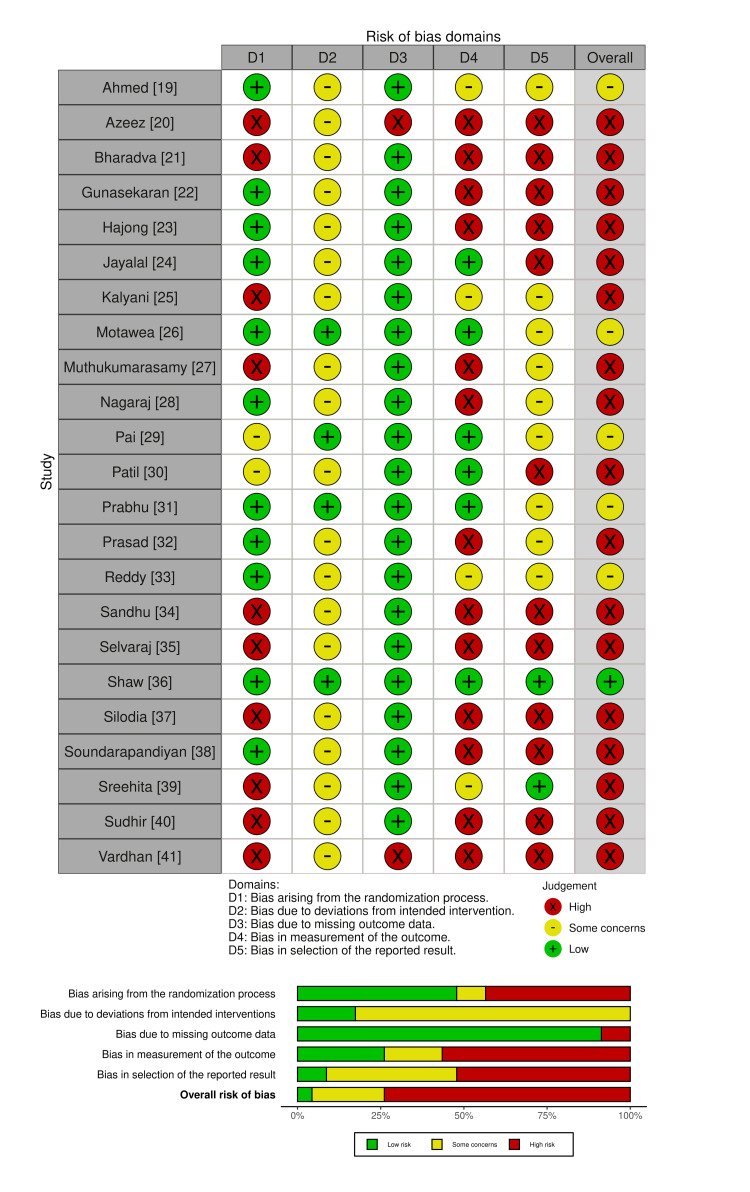 Figure 2
Figure 2| First Author (Year, Country) | Total Participants (Phenytoin, Control) | Phenytoin Arm | Control Arm | Ulcer Duration at Randomization (Weeks) | Vascular Disease† | Blinding/Allocation Concealment | Study Duration (Weeks) | Outcome Measures/Results |
| Ahmed [ | 60 (30, 30) | Phenytoin powder | Normal saline, povidone iodine, Vaseline | 4 | Excluded | §/lottery method | 8 | (1) Mean percentage reduction in ulcer area*, (2) Efficacy (>50% reduction in area) in N*, (3) Ulcer area baseline & study end |
| Azeez [ | 90 (45, 45) | Phenytoin powder | Povidone iodine | 0 | Excluded | § | 2 | (1) Mean rate of granulation tissue formation*, (2) Mean duration of hospital stay*, (3) Number of days required for healing, (4) Bacterial culture (positive or negative), (5) Side effects of topical phenytoin, (6) Skin graft uptake* |
| Bharadva [ | 56 (28, 28) | Phenytoin suspension | Povidone iodine | 0 | Included | § | 2 | (1) Wound discharge reduction*, (2) Slough reduction*, (3) Mean granulation tissue (pale/normal/absent)*, (4) Mean duration of hospital stay*, (5) Organisms isolated from the wound (6) Negative culture sensitivity |
| Gunasekaran [ | 60 (30, 30) | Phenytoin suspension | Normal saline | 0 | Excluded | §/computer randomized | 3 | (1) Negative culture percentage*, (2) Rate of granulation tissue formation*, (3) Ulcer surface area reduction, (4) Mean duration of hospital stay |
| Hajong [ | 100 (50, 50) | Phenytoin suspension | Normal saline | 0 | Included | §/computer randomized | 2 | (1) Time to 50% wound contracture area*, (2) Epithelialization time*, (3) Epithelialization time by grade of ulcer |
| Jayalal [ | 60 (30, 30) | Phenytoin suspension | Povidone iodine, saline wash, magnesium sulfate | 4 | Excluded | Observer-blind/lottery method | 1–3 | (1) Mean percentage surface area reduction*, (2) Number with >50% reduction in surface area*, (3) Number with granulation tissue present*, (4) Slough reduction*, (5) Mean duration of hospital stay*, (6) Pain (visual analogue scale)* |
| Kalyani [ | 30 (10, 10, 10) | Phenytoin | (1) Normal wound dressing, (2) topical insulin | 0 | Included | § | 4 | (1) Mean percentage reduction of wound area, (2) Mean percentage reduction of wound depth* |
| Motawea [ | 27 (9, 9, 9) | (1) Phenytoin nanostructured lipid carrier hydrogel, (2) Phenytoin hydrogel | Blank hydrogel | 0 | Excluded | Double-blind/block design | 8 | (1) Mean percentage reduction in wound area*, (2) Mean wound depth*, (3) Percentage wound healing* |
| Muthukumarasamy [ | 100 (50, 50) | Phenytoin powder | Occlusive dressing | 0 | Excluded | § | 5 | (1) Mean percentage reduction in ulcer area*, (2) Sough reduction*, (3) Negative wound cultures*, (4) Time to healthy granulation tissue*, (5) Time to complete healing*, (6) Clinical improvement*, (7) Wound discharge reduction |
| Nagaraj [ | 60 (20, 20, 20) | Phenytoin | (1) Insulin injected into wound, (2) normal saline dressing | 0 | Included | §/number lot approach | 4 | (1) Mean number of days for healing, (2) Mean difference in wound area before and after, (3) Mean difference in wound depth before and after, (4) Number of patients with granulation tissue (poor/satisfactory/healthy) |
| Pai [ | 70 (36, 34) | Phenytoin powder | Talcum powder and colloidal silicon dioxide | 0 | Included | Double-blind/§ | 6 | (1) Mean percentage reduction in ulcer area, (2) Time to disappearance of wound discharge, (3) Number of ulcers with negative wound swabs, (4) Quality of granulation tissue |
| Patil [ | 100 (50, 50) | Phenytoin suspension | Normal saline | 0 | Excluded | Observer-blind/lottery method | 6 | (1) Wound discharge reduction*, (2) Slough reduction*, (3) Granulation tissue quality (absent/pale/good/absent/pale/good)*, (4) Mean duration of hospital stay* |
| Prabhu [ | 97 (49, 48) | Phenytoin & metronidazole powder | Metronidazole powder | 4 | Included | Double-blind/block randomization | 2 | (1) Mean percentage reduction in ulcer area*, (2) Percentage increase in granulation tissue*, (3) Number of negative cultures, (4) Percentage of graft uptake* |
| Prasad [ | 50 (25, 25) | Phenytoin suspension | Povidone iodine | 0 | Included | §/lottery method | 2 | (1) Mean ulcer area*, (2) Rate of granulation tissue formation (as a percentage of ulcer area)*, (3) Negative wound culture*, (4) Mean duration of hospital stay, (5) Graft uptake* |
| Reddy [ | 60 (30, 30) | Phenytoin suspension | Normal saline | 0 | Excluded | §/computer randomized | 4 | (1) Mean wound area reduction* and (2) culture growth between day 0 & day 10* |
| Sandhu [ | 40 (20, 20) | Phenytoin suspension | Povidone iodine | 0 | Included | § | 2 | (1) Negative pus culture*, (2) Mean percentage of ulcer area covered by granulation tissue, (3) Mean duration of hospital stay, (4) Graft uptake* |
| Selvaraj [ | 100 (50, 50) | Phenytoin suspension | Povidone iodine | 0 | Excluded | § | 2 | (1) Mean percentage of ulcer area with granulation, (2) Mean ulcer surface area, (3) Mean duration of hospital stay, (4) Percentage negative culture, (5) Graft uptake |
| Shaw [ | 65 (29, 27)^ | Phenytoin-containing alginate dressing | Alginate dressing | 4 | Excluded | Double-blind/independently randomized | 16 | (1) Time to healing (survival analysis), (2) Percentage change in wound area, (3) Ulcers with positive wound swabs, (4) Serum phenytoin levels (<2.2mg/L), (5) Pain (McGill Pain Questionnaire & VAS) |
| Silodia [ | 50 (25, 25) | Phenytoin suspension | Povidone iodine | 0 | Excluded | § | 2 | (1) Number of ulcers with healthy granulation*, (2) Mean reduction in ulcer area*, (3) Number with >50% reduction in ulcer area* |
| Soundarapandiyan [ | 100 (50, 50) | Phenytoin suspension | Povidone iodine, magnesium sulfate dressing | 0 | Included | §/lottery method | 2 | (1) Percentage of ulcers with healthy granulation*, (2) Mean percentage reduction in ulcer area*, (3) Mean duration of hospital stay |
| Sreehita [ | 75 (25, 25, 25) | Phenytoin-injected dressing | (1) Sucralfate syrup dressing, (2) hydrogel cream dressing | 0 | Excluded | § | 10 | (1) Mean reduction in ulcer area week 4 & week 10, (2) Mean duration of hospital stay, (3) Abstinence from work, (4) Complete/Partial Healing |
| Sudhir [ | 70 (35, 35) | Phenytoin suspension | Povidone iodine | 2 | Excluded | § | 2 | (1) Number of ulcers with wound discharge*, (2) Number of ulcers with slough*, (3) Number of ulcers with good granulation*, (4) Mean percentage reduction in ulcer area day 7 & 14, (5) Mean duration of hospital stay*, (6) Mean number of dressings* |
| Vardhan [ | 70 (35, 35) | Phenytoin suspension | Povidone iodine | 0 | Included | § | 2 | (1) Mean duration of hospital stay*, (2) Patients with healthy granulation tissue* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetic Foot Ulcer Assessment and Management
Introduction and background
Diabetic foot ulcer (DFU) disease is one of the most common complications of diabetes, with estimates suggesting up to one-third develop a foot ulcer during their lifetime [1]. DFUs are the most common cause of lower limb amputation, a significant cause of morbidity and mortality for those with diabetes [2]. The yearly cost in England is estimated to be between £837 and 962 million; in the US, this estimate reaches $9-13 billion [3-4]. Worldwide, the prevalence of diabetes is increasing; this rise is estimated to be greater in low- and middle-income countries (LMIC) where resources and specialized services are more constrained [5]. The management of DFUs requires a multidisciplinary approach involving assessment at specialist foot care services. If severe, systemic antibiotics and imaging may be required. Surgical intervention is considered if signs of ischemia or necrosis are present [6]. Amongst topical therapies, except for sucrose-octasulfate dressings, the evidence for other compounds is poor. This is the case for antimicrobials, antiseptics, and phenytoin.
Phenytoin has been used as an anti-epileptic medication since 1939 [7]. Gingival hypertrophy was a recognized side effect, which generated the hypothesis that it could promote healing throughout the body [8,9]. The mechanism is not yet known, but studies suggest that it may promote collagen deposition, fibroblast migration, and angiogenesis [10,11]. Importantly, systemic absorption of phenytoin is not significant with topical use [12]. For these reasons, as well as its simple application and low cost, phenytoin has long been proposed as an agent that could promote healing in DFU disease. Many randomized controlled trials (RCTs) have investigated this with positive results. However, poor study design and high risk of bias have meant there is insufficient evidence for the International Working Group on the Diabetic Foot (IWGDF) to recommend topical phenytoin [13]. Prior systematic reviews have formed similar conclusions [13-15]. However, this area continues to attract interest, with at least one RCT being released every year for the last 10 years. This systematic review is the largest and most up-to-date evaluation of phenytoin use in DFU disease compared to a control.
Review
This systematic review is reported in accordance with the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. The predefined protocol was registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) with the registration number INPLASY202410023.
Eligibility criteria
The Patient, Intervention, Control, Outcome, and Study type (PICOS) tool was used to create the inclusion criteria: patients were those with diabetes-related foot ulcers, the intervention was phenytoin, the control included standard care or placebo, outcomes were identified as all healing-related outcomes, and the study type was RCTs.
Exclusion criteria included the following: (1) ulcers of other aetiologies, such as pressure ulcers or leprosy ulcers, and (2) comparative studies, systematic reviews, editorial letters, or case reports.
Selection of studies
The search was conducted independently by two authors using the following databases: Medline, Embase, Cochrane Library, ClinicalTrials.gov, and Google Scholar. The search strategies are outlined in the appendix. Databases were searched on January 5, 2024. Duplicates were removed. Two authors independently screened the studies against the eligibility criteria, first by the title and then by the abstract. Full texts were then retrieved. Any discrepancies were resolved by a third author.
Data extraction
Data extraction was carried out independently by two authors. This included the following variables: all healing-related outcomes and whether these were statistically significant, the number of patients, treatment arm details, ulcer duration at randomization, inclusion of vascular disease, blinding and allocation concealment, and study duration. Data were filled directly into two separate tables, which were then collated into one.
Data analysis
Data were analyzed descriptively due to their heterogeneity. Outcomes were grouped into similar categories for descriptive analysis. A meta-analysis was not completed (reasons explained below).
Quality assessment
The quality of each paper was independently assessed by two authors using the Risk of Bias 2 (RoB 2) tool [17]. Any discrepancies were resolved by the third author. The results were collated, and then the Robvis visualization tool was used to create the summary diagram [18].
Results
A total of 129 records were obtained from the systematic search. Studies were organized according to the inclusion and exclusion criteria discussed above. Following the removal of 41 duplicates and the screening of titles and abstracts, 48 additional studies were removed. This left 40 studies for full-text evaluation; five studies were not retrieved, and 12 were excluded due to incorrect study design. This left 23 studies for inclusion in the systematic review [19-41], which is depicted in Figure 1. Table 1 provides the characteristics of the included studies.
PRISMA flowchart for study identificationPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 1: Characteristics of the included studies: Indicates a finding (to support the beneficial effect of phenytoin) that was statistically significant (p < 0.05) as reported. It does NOT infer a methodologically reliable or clinically relevant effect.§: No information reported.†: If no explicit mention of excluding patients with vascular disease, it was assumed they were included.‡: Primary outcome in BOLD (majority of studies did not identify a primary outcome).^: Sample size was calculated.*
Quality Assessment
Overall, the quality of the studies was low, with 17 studies rated as having a high risk of bias and only one achieving a low risk. Ten studies did not adequately describe their randomization process. Only six studies had blinded assessors, and only four of those had blinded participants. Outcomes chosen for assessing healing varied significantly between the studies. Two studies lacked explanations for the missing outcome data, as summarized in Figure 2.
Traffic light and summary plot summarizing the quality assessment of the included studies
Interventions
Phenytoin was either delivered as a powder applied directly to the ulcer or as a suspension (dissolved in normal saline) that the dressings were soaked in. The dose of phenytoin used was based on the ulcer surface area for all studies.
Regarding control interventions, 14 studies used povidone iodine or normal saline [19-23,28,30,32-35,37,40,41]. Prabhu et al. used metronidazole powder, administered with phenytoin for the active intervention [31]. As both are powders, this ensured blinding was maintained when both the control and active intervention were delivered. Other control interventions included magnesium sulfate, hydrogel, occlusive dressings, talcum powder/colloidal silicon dioxide, and alginate dressing. Four studies included other treatment arms investigating injected insulin, sucralfate syrup dressing, and phenytoin nanostructured lipid carrier hydrogel; these outcomes have not been investigated as they are beyond the scope of this systematic review.
Outcomes
Quantification of the ulcer healing was assessed in three ways: ulcer area change, ulcer depth change, or time taken for ulcer closure. A total of 17 papers reported area change before and after, and 10 reported a significant difference between phenytoin and control. Wound depth change was reported by three papers, where two studies reported a significant difference. The time to complete healing was reported by three papers, with one finding a significant difference.
Hallmarks of healing were also used to assess the role of phenytoin in the healing process. These hallmarks include the quantification of granulation tissue, the absence of slough, the absence of wound discharge, a negative wound culture, and graft uptake. A total of 17 papers reported a change in granulation tissue, but the methods of measuring this varied, including the rate of formation, number with healthy or good granulation, time to healthy granulation, or percentage of the wound covered by granulation (of which 13 papers reported a significant positive effect in these outcomes). Five papers reported the absence of slough; all five were significant. Five papers reported a change in wound discharge; three were significant. A total of 11 papers reported a difference in wound swab culture results between phenytoin and the control; five of these differences were significant. Graft uptake was reported by five papers, and four papers reported improved graft uptake with phenytoin.
Other outcomes unrelated to healing included assessments of pain scores and the duration of hospital stay or time away from work. Two papers reported pain scores as an outcome; one reported a significant difference in pain scores between the phenytoin and control groups. The duration of hospital stay was reported by 12 papers; six papers reported reduced hospital stay with phenytoin compared to controls.
Discussion
The aim of this systematic review was to investigate the effect of phenytoin on DFU disease by examining RCTs comparing phenytoin to standard care/placebo. A total of 23 RCTs were identified, with 20 studies conducted in India and one each in Egypt, Pakistan, and the United Kingdom. Overall, 20 of the 23 studies reported results that recommended the use of phenytoin based on various outcomes, including an improved healing area, increased presence of granulation tissue, and absence of slough. However, these results need to be interpreted with caution.
Firstly, the quality of the studies was very poor. For example, 10 studies did not describe the randomization process, and 17 failed to implement blinding, including a lack of blinding in outcome assessment. Fundamental lapses in the randomization and blinding process mean that the risk of systematic error is high, leading to significant biases in these conclusions.
Secondly, there is a high risk of random error in these conclusions. Only one study described an appropriate a priori sample size calculation, and only four identified a primary endpoint for analysis. This introduces a high risk of bias due to random error and a potential for false positives resulting from multiple testing.
Thirdly, any attempt to minimize the above by performing a meta-analysis of the studies was not possible due to marked heterogeneity between the studies and non-compliance with current reporting standards. The main sources of heterogeneity were the time of randomization (ranging from ulcers at first presentation to 16 weeks), differences in the total duration of the active study period, the inclusion of ulcers with underlying vascular disease, and marked variation in the outcome measure. This was also expressed by Shaw et al. in their 2008 investigation of phenytoin use [14].
Finally, ulcer size data could theoretically be used to perform a meta-analysis to obtain an overall size effect by grouping studies with similar characteristics. However, the papers report ulcer sizes in various metrics (e.g., mean reduction in size, absolute sizes at the end of the study, and ulcer measurements at different time points), which limit the statistical feasibility of undertaking such a calculation. Furthermore, despite contacting various authors for raw data on ulcer sizes, we were unable to obtain the required information to conduct a reliable meta-analysis.
The results of this systematic review reaffirm the conclusions from the IWGDF guidelines, which do not recommend the use of phenytoin due to the low certainty of the evidence. Both Shaw et al. and Vas et al. also highlighted the varying methodological quality of the studies [14,15].
The strength of this study is that it is the most up-to-date systematic review of trials investigating phenytoin in DFU disease. The inclusion of multiple new studies during our review indicates a continued interest in this area. This systematic review also summarizes various outcomes that may serve as surrogate endpoints in future clinical trials, especially when designing multi-stage or multi-arm clinical trials. This will guide future researchers in planning their trials more efficiently.
The main limitation of our review is that, given the poor reporting in these studies and multiple positive results, there is likely to be significant publication bias despite a broad inclusion criterion for the review. In addition, there is a high regional skew in the origin of these studies (India is the main contributor); this may reflect a local interest in the intervention based on clinical context; however, the reason for this needs to be explored by funding organizations in the future.
Conclusions
In conclusion, many of the studies have recommended the use of phenytoin, with results suggesting that it has a beneficial effect on wound healing. However, the absence of blinding, insufficient randomization, and lack of sample size calculation indicate a high risk of bias. There was also marked heterogeneity between the studies, with varying durations, reported size metrics, and times of randomization. At present, the available evidence does not support the use of phenytoin. The results should be treated as hypothesis-generating conclusions. Further studies are required, with larger patient numbers and minimized risk of both systematic and random errors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diabetic foot ulcers and their recurrence N Engl J Med Armstrong DG Boulton AJ Bus SA 2367237537620172861467810.1056/NEJ Mra 1615439 · doi ↗ · pubmed ↗
- 2Chapter V: diabetic foot Eur J Vasc Endovasc Surg Lepäntalo M Apelqvist J Setacci C 607442201110.1016/S 1078-5884(11)60012-922172474 · doi ↗ · pubmed ↗
- 3The cost of diabetic foot ulcers and amputations to the National Health Service in England Diabet Med Kerr M Barron E Chadwick P 99510023620193100437010.1111/dme.13973 · doi ↗ · pubmed ↗
- 4Burden of diabetic foot ulcers for Medicare and private insurers Diabetes Care Rice JB Desai U Cummings AK Birnbaum HG Skornicki M Parsons NB 6516583720142418688210.2337/dc 13-2176 · doi ↗ · pubmed ↗
- 5Global estimates of the prevalence of diabetes for 2010 and 2030 Diabetes Res Clin Pract Shaw JE Sicree RA Zimmet PZ 4148720101989674610.1016/j.diabres.2009.10.007 · doi ↗ · pubmed ↗
- 6IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023)Clin Infect Dis SennevilleÉ Albalawi Z van Asten SA 28610202310.1093/cid/ciad 52737779457 · doi ↗ · pubmed ↗
- 7Phenytoin Stat Pearls [Internet] 8 2024 Gupta M Tripp J Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 551520/
- 8The use of Dilantin in the treatment of epilepsy Ann Intern Med Kimball O Horan T 787793131939